Download presentation
Presentation is loading. Please wait.

1
Screening for Tuberculosis Infection
Sample 2 Shea Rabley, RN, MN TB Center Webinar May 1, 2014 test

2
Disclosures None

3
Objectives List the 2 methods that can be used when screening TB Infection. Describe the difference between a TB reactor and a TB converter.

4
Why Screen for TB Infection?
Tuberculosis is one of the world’s deadliest diseases. At least one-third of the world’s population are infected with TB. At least one person becomes infected every second. Each year, approximately 8.6 million people around the world become sick with TB disease. TB kills 3 people every minute annually worldwide.

5
Why? There were an estimated 450,000 cases of multi-drug resistant (MDR) TB in 2012. TB is the leading killer of people who are HIV- infected. Children account for 500,000 new cases annually and 75,000 will die of TB disease. Approximately one in every 10 people with TB infection will progress to active TB at some point in their life; 5% in the first 2 years and the other 5% at some time over their lifespan.

6
Why? Foreign born persons comprised 64.6% of the cases of TB in the US in 2013. The key to controlling TB is accurately and efficiently identifying those who have the potential to become infected or to progress to TB disease once infected. Global organizations are beginning to acknowledge that to fight TB effectively, identifying and treating latent TB infection—as well as active TB disease—are vital.

7
Who Should be Tested? Persons at risk of exposure to person known to have TB disease OR Persons who once infected have conditions assoicated with an increased risk of progression from TB infection to TB disease.

8
Specifically Contacts to known cases
Persons with HIV or other diseases that weaken the immune system Persons with signs/symptoms of TB disease Persons from countries where TB is common (Latin America, Caribbean, Asia, Africa, Eastern Europe & Russia) People who live or work in facilities where TB is common: hospitals that care for persons with TB disease, homeless shelters, correctional facilities and other congregate settings (nursing homes, CRCFs, other locally defined facilities)
 People who live or work in facilities where TB is common: hospitals that care for persons with TB disease, homeless shelters, correctional facilities and other congregate settings (nursing homes, CRCFs, other locally defined facilities)")
9
Specifically Persons with: Radiological evidence of old healed TB
Low body weight or malnourished Conversions in their tuberculin test status Medical conditions such as: Diabetes Mellitus Silicosis Organ transplantation Chronic Renal Failure Cancers of head and neck Gastrectomy or jejunoileal bypass Conditions that require prolonged use of corticosteroids or other immunosuppressive agents (TNF-a antagonists, cancer chemotherapy)
")
10
How to Determine TB Infection
I. Tuberculin Skin Test – TST II. Interferon Gamma Release Assay - IGRA A. QuantiFERON-TB Gold In-tube – QFT-GIT B. T-Spot.TB – T-Spot

11
I. Tuberculin Skin Testing
In 1890, Robert Koch announced a cure for tuberculosis years after discovering the cause of TB Cure consisted of subcutaneous doses of tuberculin Subsequently found to be ineffective Ultimately became a widely-used diagnostic test for TB infection

12
Immune Response to Tuberculin
A positive test is result of a delayed-type hypersensitivity (DTH) response Reaction characterized by edema and formation of induration – a hard, raised area, not redness – measured in mm Reaction generally complete in hours DTH response detectable 2-10 weeks after initial infection
 response. Reaction characterized by edema and formation of induration – a hard, raised area, not redness – measured in mm. Reaction generally complete in hours. DTH response detectable 2-10 weeks after initial infection.")
13
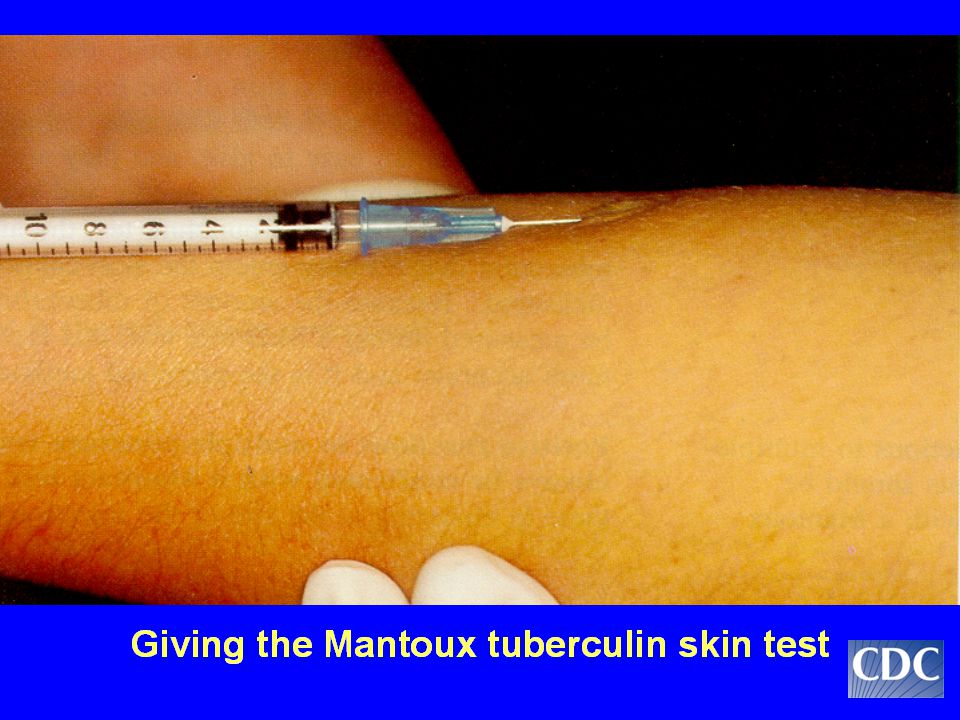
Mantoux Skin Testing Method
Developed by Charles Mantoux in 1908 The standard tuberculin skin test Two Purified Protein Derivative (PPD) antigen products licensed by FDA: - Tubersol - Aplisol Do not indiscriminately switch between brands of tuberculin antigen
 antigen products licensed by FDA: - Tubersol. - Aplisol. Do not indiscriminately switch between brands of tuberculin antigen.")
14
Administering the Tuberculin Skin Test
Inject intradermally 0.1 ml of 5 TU PPD tuberculin Produce wheal 6 mm to 10 mm in diameter Standardize your test procedure Follow standard precautions for infection control; gloves are not necessary

16
Needle Too Deep

17
Needle Too Shallow

19
Factors that May Affect the
Skin Test Reaction Type of Reaction Possible Cause False-positive Nontuberculous mycobacteria BCG vaccination Anergy False-negative Recent TB infection Very young age (<6 mos old) Live-virus vaccination Overwhelming TB disease or other infection
 Live-virus vaccination. Overwhelming TB disease or other infection.")
20
Storage and handling of PPD
Date and initial when vial is opened Discard 30 days after opening Draw up just prior to injection Store at ºF in a refrigerator or cooler with ice packs and keep out of direct light - antigen is sensitive to light and heat; these elements can affect antigen’s stability and potency

21
Boosting Some people with TB infection may have a negative skin test reaction when tested many years after initial infection The initial skin test may stimulate (boost) their ability to react to tuberculin Positive reactions to subsequent tests may be misinterpreted as new infection
 their ability to react to tuberculin. Positive reactions to subsequent tests may be misinterpreted as new infection.")
22
BCG Vaccination Bacillus of Calmette and Guerin
First officially used as TB vaccine in 1921 Poor efficacy but believed to be useful in some foreign countries to prevent serious extrapulmonary TB disease in infants & young children (TB meningitis & disseminated or miliary TB) Positive tuberculin reaction in BCG-vaccinated persons usually indicates infection with M.tuberculosis
 Positive tuberculin reaction in BCG-vaccinated persons usually indicates infection with M.tuberculosis.")
23
Recommendations for BCG Vaccination
Not recommended in the United States because: low risk of infection with M. tuberculosis variable effectiveness of BCG interpretation of tuberculin skin test result complicated by BCG

24
Reading the TST Results, based on cutpoint, and implications for further evaluation are based on: - the measurement, in millimeters, of the induration – not erythema and - the risk factors found in the persons targeted medical and social history.

26
Two-Step Testing Completed to establish a true baseline status for adults who will be retested periodically (ie: serial testing program): If first test positive, consider person infected If first test negative, give 2nd test 1-3 weeks later If second test positive, consider person infected If second test negative, consider person uninfected

27
Key Definitions Reactor - an individual with a + skin test reaction (size interpreted as “positive” based on risk factors) with no clear documentation or history of being skin tested in the last two years. Convertor – any individual with a negative skin test documented as baseline but who developed positive reaction with increase in reaction size of >10 mm within the past two years or a change from negative to positive on an IGRA.
 with no clear documentation or history of being skin tested in the last two years. Convertor – any individual with a negative skin test documented as baseline but who developed positive reaction with increase in reaction size of >10 mm within the past two years or a change from negative to positive on an IGRA.")
28
II. Interferon Gamma Release Assay (IGRA)
IGRAs measure the cell-mediated response to specific TB antigens in whole blood. WBCs in TB infected persons release INF-g when mixed with antigens derived from MTB. Initially, these tests were called a blood assay for mycobacterium tuberculosis or BAMT. Currently there are two (2) IGRAs in use: A. QuantiFERON-TB Gold In-tube (QFT-GIT) B. T-Spot .TB (T-Spot)
 IGRAs in use: A. QuantiFERON-TB Gold In-tube (QFT-GIT) B. T-Spot .TB (T-Spot)")
29
Advantages Requires a single patient visit
Results not subject to reader bias and error Greater sensitivity and specificity – not affected by BCG or most nontuberculous mycobacteria Results are usually available within 24 hours. Does not “boost” responses measured by subsequent tests (as TSTs do).
.")
30
Disadvantages More costly than TST – or assumed to be so…
Not recommended for use in children < five (5) years of age Blood must be processed in 8-30 hours Can have false positive, false negative or indeterminate test results
 years of age. Blood must be processed in 8-30 hours. Can have false positive, false negative or indeterminate test results.")
31
Factors that May Affect the
IGRA Result Type of Reaction Possible Cause False-positive Stage of infection Co-morbid conditions that affect immune functions Issues with collection tubes Improper collection, transport, running or interpretation of the result False-negative Delay in incubation Improper collection, transport, running or interpretation of the result

32
QuantiFERON-TB Gold In-Tube
QFT-GIT requires 3 tubes provided by the lab – GRP - each designed to allow only 1ml of blood to enter. Gray – Negative Control or Nil – “background noise” Red – Antigen – Response of the test Purple – Positive Control or Mitogen – shows immune status and correct handling & incubation of the tubes Will receive a numeric as well as a positive, negative or indeterminate result. The result is based on IFN-g concentration Positive - > 0.35 Negative - < 0.35 Indeterminate - < 0.35 or > 0.35 if Nil > 8.0 & any result in Mitogen tube OR any result in antigen & mitogen with > 8.0 in Nil

33
T-Spot.TB T-Spot uses 1 standard green top tube, but requires differing amounts of blood: 6 ml: Adults & children over 9 years old 4 ml: Children 2 to 9 years old 2 ml: Children up to 2 years old Interpretation of Results: Interferon-gamma is captured and presented as spots from T cells sensitized to Mycobacterium tuberculosis antigens. There are 4 panels used. Results are interpreted by subtracting the spot count in the negative (NIL) control from the spot count in Panels A and B. The 4th panel is the anitgen panel or positive control. Results are reported as positive, negative, borderline and indeterminate.
 control from the spot count in Panels A and B. The 4th panel is the anitgen panel or positive control. Results are reported as positive, negative, borderline and indeterminate.")
34
In Conclusion Choose a test for TB screening based on the individual factors associated with each person and the facts surrounding the need for testing.

35
My Pets and Peeves Miss Peaches Speed TST vs PPD Reactor Convertor

36
References CDC. Targeted Testing and Treatment of Latent Tuberculosis Infection. June 9, CDC. Testing for Tuberculosis. April 27, CDC. Trends in Tuberculosis – United States. MMWR.63 (11); March 24, CDC. Updated Guidelines for Using Interferon Gamma Release Assays to Detect Mycobacterium tuberculosis Infection. United States. June 25, Celestis (Qiagen). QuantiFERON-TB Gold – Frequently Asked Questions – Health Professionals Oxfordimmunotec. T-Spot.TB – The Easy TB Test Qiagen. QuantiFERON Technology support/spotlight/qft_technology-spotlightpages/. WHO. Reach the 3 Million. Stop TB Partnership DAY_BROCHURE_14March.pdf.
; March 24, CDC. Updated Guidelines for Using Interferon Gamma Release Assays to Detect Mycobacterium tuberculosis Infection. United States. June 25, s_cid=rr5905a1_e. Celestis (Qiagen). QuantiFERON-TB Gold – Frequently Asked Questions – Health Professionals Oxfordimmunotec. T-Spot.TB – The Easy TB Test Qiagen. QuantiFERON Technology support/spotlight/qft_technology-spotlightpages/. WHO. Reach the 3 Million. Stop TB Partnership DAY_BROCHURE_14March.pdf.")
38
Questions & Discussion

Similar presentations















>")


 Facts>")

 PHCL 442 Lab Discussion Jamilah Al-Saidan, M.Sc.>")
