Download presentation
Presentation is loading. Please wait.

1
Hepatic Disorders: Hepatitis/Cirrhosis
Lisa Randall, RN, MSN, ACNS-BC RNSG 2432

2
Objectives Compare and contrast risk factors associated with hepatitis and cirrhosis Analyze the etiology and pathophysiology of hepatitis and cirrhosis Integrate diagnostic tests with etiology, pathophysiology, and signs/symptoms of both disorders Formulate relevant prioritized nursing diagnoses that address physical, pyschosocial, and learning needs and evaluate nursing interventions

3
Anatomy & Physiology

4
A Liver B Hepatic vein C Hepatic artery D Portal vein E Common bile duct F Stomach G Cystic duct H Gallbladder

5
Pathophysiology Largest organ Metabolic functions Bile synthesis
Hepatocytes Bile secretion Storage Mononuclear phagocyte system Kupffer cells Phagocytic activity

6
Metabolic functions Metabolism of glucose Protein Fatty acids
Cholesterol

7
Other Functions Immunologic Blood storage Plasma protein synthesis
Clotting Storage of vitamins and minerals Waste products of hemoglobin Bile formation and secretion Steroids and hormones Ammonia Drugs, ETOH, toxin metabolism

8
HEPATITIS

9
Pathophysiology Inflammation Hepatic cell necrosis
Proliferation/enlargement Kupffer cells Cholestasis Regeneration

11
Types Chronic Fulminant Toxic Hepatobillary

12
Hepatitis Types (Viral)
B C D E G *see handout

13
Clinical Manifestations
Acute Chronic Anorexia N/V RUQ pain Bowel irregularity Malaise HA Fever Arthralgias Uticaria Weight loss Jaundice Hepatomegaly Splenomegaly Pruritus Dark urine Bilirubinuria Light stools Fatigue Malaise Easy fatigability Hepatomegaly

14
Phases Preicteric Prodromal Icteric Jaundice Posticteric Convalescent

15
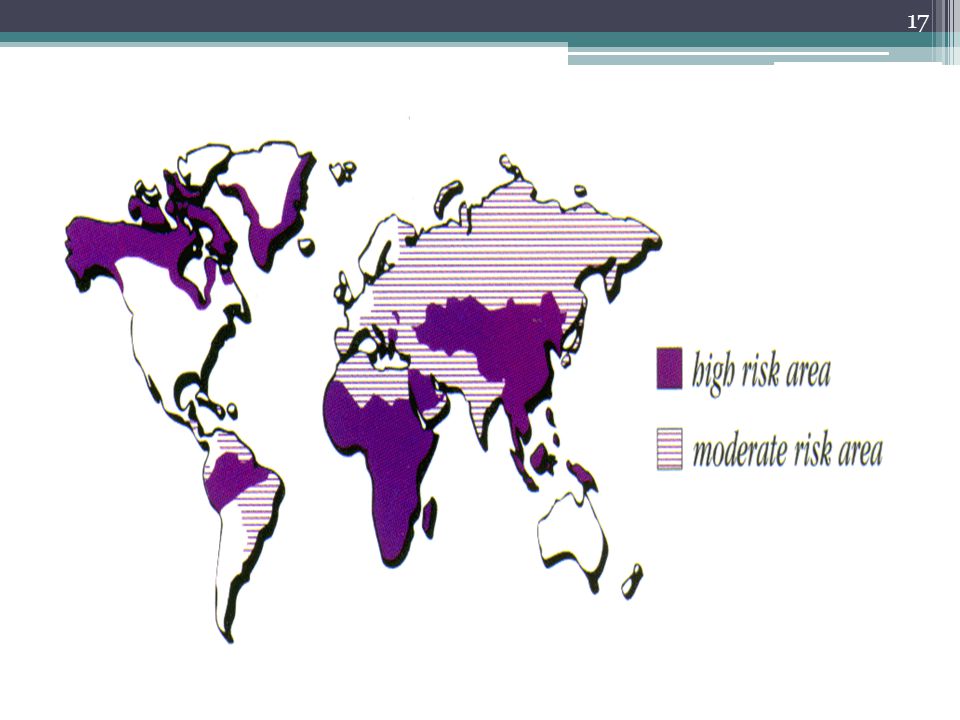
Hepatitis A Fecal/oral 15-50d S/S Labs Vaccine IgG Prevention
Light stools Dark urine Fatigue Fever Jaundice Labs Vaccine IgG Prevention

16
Hepatitis B Percutaneous/permucosal Sexual contact Perinatal 45-180d
S/S 30% asymptomatic Flu Light stools Dark urine Fatigue Fever Jaundice Labs Prevention Vaccine IgG Safe sex No sharing of razors, toothbrushes, needles Chronicity Antivirals

18
Hepatitis C Percutnaeous/mucosal Sexual contact Perinatal 14-180d S/S
80% asymptomatic HBV Labs Prevention Safe sex No sharing of razors, toothbrushes, needles Chronicity Interferon antivirals

20
Hepatitis D HBV 2-26wk Labs Interferon HBV vaccine S/S

21
Hepatitis E Fecal/oral Contaminated water Poor sanitation 15-64d Labs
S/S HBV No vaccine

22
Diagnostics LFT ALP Serum bilirubin Liver biopsy Antigen specific

23
Treatment Diet Fluid management Bed rest Drug therapy
High cal/protein, low fat Vitamins (B, K) ETOH/Drugs Fluid management Bed rest Drug therapy Prevention of HAV and HBV Interferon Lamivudine Ribavirin Acetaminophen
 ETOH/Drugs. Fluid management. Bed rest. Drug therapy. Prevention of HAV and HBV. Interferon. Lamivudine. Ribavirin. Acetaminophen.")
24
Nursing Diagnoses Risk for infection (transmission)
Imbalanced nutrition Disturbed body image Knowledge deficit

25
Cirrhosis

26
Pathophysiology Caused by destruction of liver cells, fibrosis and nodule formation restricting blood and bile flow Normal hepatic blood pressure is near zero. Restriction of blood flow in liver dysfunction causes hypertension, and blood will attempt to find other pathways, bypass liver Results in significant impairment of liver function 80% destroyed before signs and symptoms Liver can regenerate itself if good nutrition, rest, and no alcohol

27
Types of Cirrhosis Classified by risk factors
Post necrotic Hepatitis Alcoholic Cirrhosis Laennec’s metabolic changes in liver, particularly fat Biliary obstructive Cardiac right side heart failure Drug induced INH, rifampin, Tylenol

28
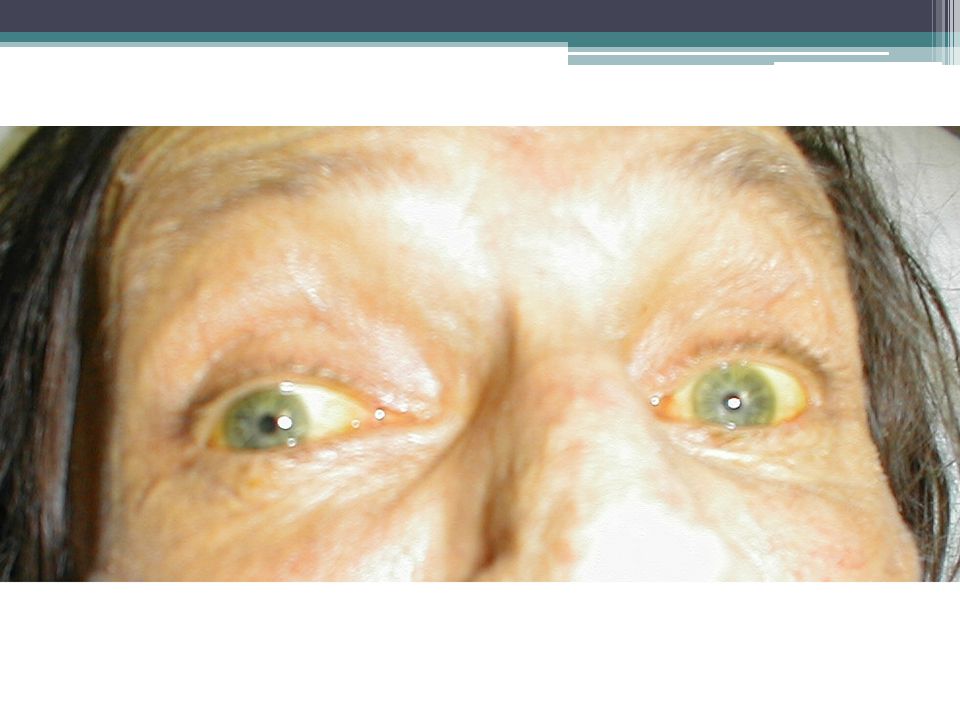
Signs & Symptoms Liver enlarged Dull pain RUQ Weakness Anorexia Skin
Sclera Portal hypertension Splenomegaly Ascites Esophageal varices Hepatic encephalopathy Hepatorenal Syndrome Liver failure

29
Signs & Symptoms

31
Jaundice Excess bilirubin Heptocellular Obstructive Hemolytic
Cirrhosis Obstructive Hemolytic Excessive destruction of RBCs Transfusion reaction Autoimmune Faulty hemoglobin Sickle cell

32
Diagnostics LFT CBC Coags Bilirubin Albumin Ammonia Esophagascopy
Liver biopsy *See Table 44.15

33
Liver Biopsy 3 types Complications Needle Laparoscopic Transvenous
Catheter Blood clotting problems Excess fluid Complications Puncture of lung or gallbladder Infection Bleeding Pain

35
Liver Biopsy Adequacy of clotting- PT/ INR, Platelets (Vit. K?)
Type and cross match for blood Stop aspirin, ibuprofen, and anticoagulants 1 wk. before Chest x-ray Consent form & NPO 4 to 8 hr. Vital signs & Empty bladder Supine position, R arm above head Hold breath after expiration when needle inserted Be very still during procedure – 20 minutes

36
After Needle Liver Biopsy
Pressure Right side minimum of 2 hrs flat hrs Vital signs & check for bleeding NPO X 2 hr after Assess for peritonitis, shock, & pneumothorax Rt. shoulder pain common caused by irritation of the diaphragm muscle usually radiates to the shoulder a few hours or days. Soreness at the incision site Tylenol avoid aspirin or ibuprofen for the first week because they decrease blood clotting, which is crucial for healing. Avoid coughing, straining, lifting x 1-2 weeks

37
Nursing Assessment LOC Reflexes Pupils Orientation Sensory/motor
Hyperreflexia Pupils Orientation Sensory/motor Asterexis Coordination Dysmetria Fluid/electrolytes Acid/base imbalances See table 44.17

39
Nursing care Safe environment Sustain life

40
Nursing Diagnoses Risk for infection (transmission)
Hepatitis Cirrhosis Risk for infection (transmission) Imbalanced nutrition Disturbed body image Knowledge deficit Excess fluid volume Disturbed thought process Ineffective protection Impaired skin integrity Imbalanced nutrition Knowledge deficit
 Imbalanced nutrition. Disturbed body image. Knowledge deficit. Excess fluid volume. Disturbed thought process. Ineffective protection. Impaired skin integrity. Imbalanced nutrition. Knowledge deficit.")
41
Treatment Diet Fluid management Drug therapy
Sodium restriction High carbs Mod fat 75-100gm protein 60-80gm/d (hep encephalopathy) Fluid management Drug therapy Diuretics Laxatives Anti-infective agents Surgical/medical interventions
 Fluid management. Drug therapy. Diuretics. Laxatives. Anti-infective agents. Surgical/medical interventions.")
42
Major Complications of Cirrhosis
Portal hypertension Variceal bleeding Ascites Spontaneous bacterial peritonitis Splenomegaly Hepatorenal syndrome Hepatic encephalopathy

43
Portal Hypertension Arteriovenous shunting Marked ascites
Caput medusae Dilated abdominal veins Esophageal varices Hemorrhoids Hyperslenism Mod anemia Neutropenia Thrombocytopenia

44
Surgical/Medical Interventions
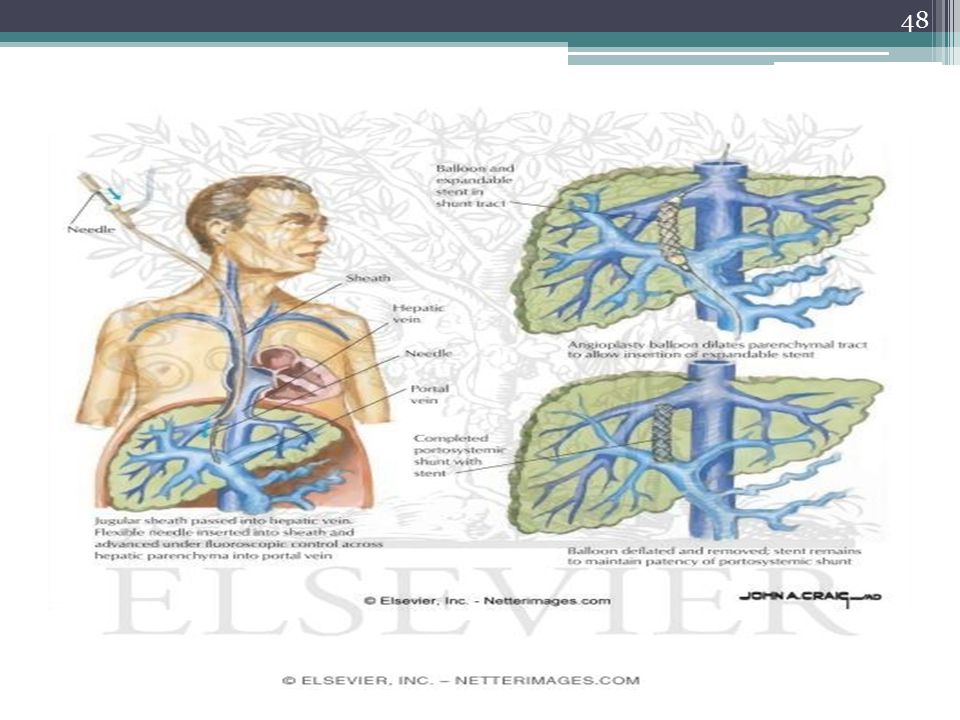
Paracentesis Gastric lavage Balloon tamponade Schlerotherapy Banding TIPS (transjugular intrahepatic portosystemic shunt) Liver transplant
 Liver transplant.")
45
Ascites Sodium restriction Bedrest initially Diuretics Fluid removal
Spironolactone Lasix HCTZ Fluid removal Paracentesis Peritoneovenous Shunt

46
Ascites Caput medusae

47
Paracentesis Only used if respiratory distress
Pt will loose grams of protein Pt in sitting position Empty bladder first Post--watch for hypotension, bleeding, shock & infection

50
Esophageal varices Collateral vessels
Complex of swollen, enlarged veins Portal hypertension 2/3-3/4 Bleeding LIFE-THREATENING

51
Esophageal varices treatment
Active bleeding Central line & pulmonary artery pressures Blood transfusions & fresh frozen plasma for clotting factors Somatostatin or Vasopressin – constrict gut vessels Airway/trach Later prevention of re-bleeding Beta-blockers Long-acting nitrates Soft food, chew well, avoid intra-abdominal pressure Protonix

53
Sclerotherapy sclerosant solution (ethanolamine oleate or sodium tetradecyl sulphate) Complications fever, dysphagia and chest pain, ulceration, stricture, and (rarely) perforation.
 perforation.")
54
Band ligation Fewer treatment sessions and complications than sclerotherapy.

55
Balloon tube tamponade
Tube is inserted through the mouth Correct placement within the stomach is checked by auscultation while injecting air through the gastric lumen Gastric balloon is then inflated with 200 ml of air Gastric balloon is pulled up against the esophagogastric junction, compressing the submucosal varices Tension is maintained by strapping a split tennis ball to the tube at the patient's mouth Complications gastric and esophageal ulceration aspiration pneumonia esophageal perforation.

56
Minnesota Tube Sengstaken-Blakemore tube – has only 3 lumens
**Respiratory assessment**

57
Hepatic encephalopathy
Neuropsychiatric manifestation Decreased liver detoxification>>> Increased ammonia Terminal complication Changes in LOC Asterixis

58
Treatment HE Reduce ammonia Lactulose Neomycin sulfate Cathartics
Enemas Liver transplantation

59
Hepatorenal syndrome Portal HTN + liver decompensation
Systemic vasodilation Decreased arterial BF Renal vasoconstriction Functional renal failure Azotemia Oliguria Liver transplantation

60
Liver Transplant

61
Liver Transplant

62
Liver transplant complications
Rejection 70% Medications Infection immunosuppression Cancer

63
Patient Teaching Therapeutic communication Diet* Exercise
Lifestyle modifications Drugs Follow-up Resources

65
Legal/Ethical Considerations
Advance directives Palliative care Organ donation

66
Donors Live donor Liver regenerates
5 years Survival rates increase / shorter wait time Medical and psychological evaluations Potential donors evaluated for: liver disease, alcohol or drug abuse, cancer, or infection. hepatitis, AIDS, and other infections. matched according to blood type and body size. Age, race, and sex are not considered. Cadaver donor have to wait for brain dead donor

67
Review Pathophysiology Cirrhosis Portal hyperetension Liver failure
Encephalopathy Hepato-renal syndrome Signs & Symptoms Treatment Nsg. Care Complications

68
Question A client presenting with ascites s/t liver failure is being evaluated for fluid balance. Which of the following provides the best indicator of fluid status? a. I&O b. LFT c. caloric intake and serum protein levels d. daily weight

69
Question When providing DC teaching to the patient with cirrhosis, his wife asks the RN to explain why there is so much emphasis on bleeding precautions. Which of the following provides the most appropriate response? a. “The liver affected by cirrhosis is unable to produce clotting factors.” b. “The low protein diet will result in reduced clotting factors.” c. “The increased production of bile decreases clotting factors.” d. “The required medications reduce clotting factors.”

70
Question When explaining the rationale for the use of lactulose syrup ot the patient with chronic cirrhosis, the nurse would choose which of the following statements? a. “lactulose reduces constipation, which is a frequent complaint with cirrhosis.” b. lactulose suppresses the metabolism of ammonia and aids in its elimination through feces.” c. lactulose helps to reverse cirrhosis of the liver.” d. lactulose can be taken intermittingly to reduce side effects.”

71
Question The patient has just had a liver biopsy. Which of the following nursing actions would be the priority after the biopsy? A. monitor pulse and BP every 30 minutes until stable and then hourly for up to 24 hours. B. ambulate every 4 hours for the first day, as long as the patient can tolerate it. C. measure urine specific gravity every 8 hours for the next 48 hours. D. maintain NPO status for 24 hours post-biopsy.

72
Question A male client is being treated for ruptured esophageal varices with a Sengstaken-Blakemore tube. His VS have been stable, and the suction port is draining scant amounts of drainage. He suddenly becomes acutely dyspneic, and oximetry reveals an O2 sat of 74%. The nurse’s immediate action is to A. release the esophageal balloon B. release the gastric balloon C. increase the suction D. irrigate the gastric balloon

73
Question A newly admitted client with cirrhosis of the liver has a distended abdomen and the umbilicus is protruding. The nurse knows the pathological basis for this is A. increased fluid intake resulting from excessive use of alcohol causing overhydration B. increased size of the liver resulting in abdominal distention C. hypoalbuminemia causing fluid to leave the vascular system and enter the peritoneal cavity D. shunting of the blood to the collateral circulation in the esophagus resulting in decreased blood volume and accumulation of fluid

74
Case Study

Similar presentations














 that progresses to cirrhosis Replacement of liver tissue.>")
. Presents at 2am with a big haematemesis Unable to give a history.>")




>")




