Download presentation
Presentation is loading. Please wait.

1
SALIVARY GLAND DISEASES
DR.LINDA MAHER

2
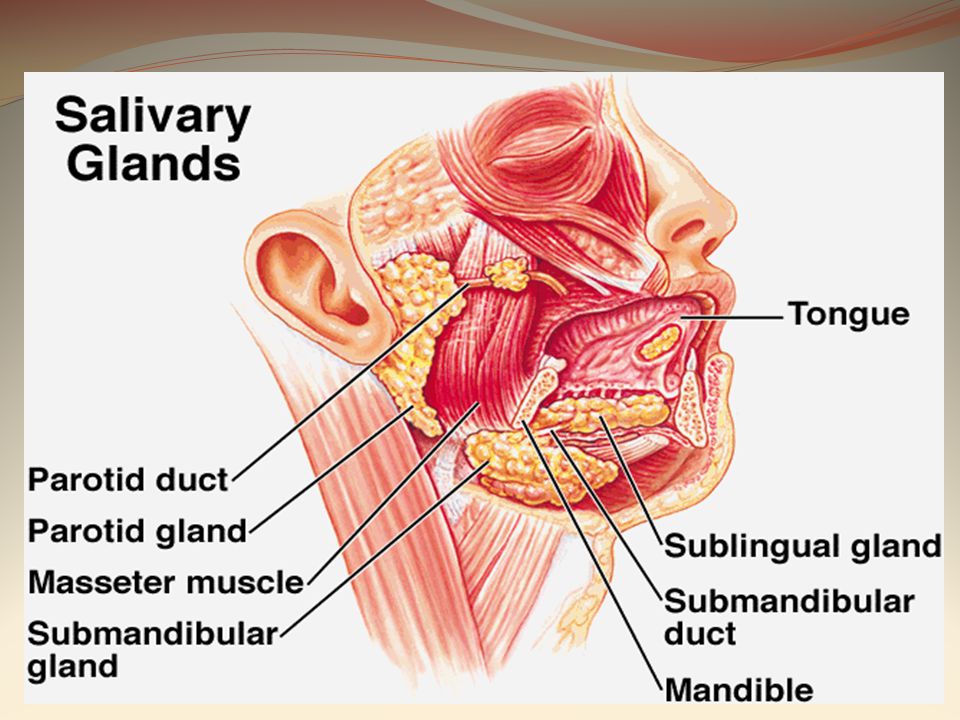
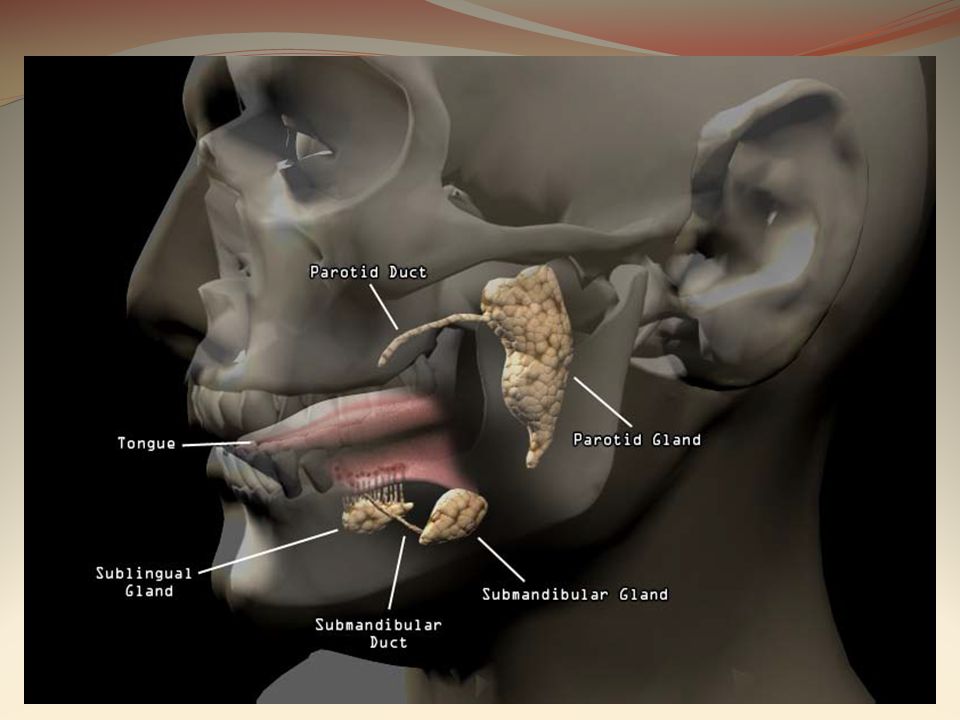
SALIVARY GLANDS CLASSIFIED INTO : 1\MAJOR SALIVARY GLANDS
group of glands that secretes saliva CLASSIFIED INTO : 1\MAJOR SALIVARY GLANDS 1 -parotid glands 2 -submandibular glands 3 -sublingual glands 2\MINOR SALIVARY GLANDS more than 400 small glands scattered all around the oral cavity(except the Gingiva and anterior palate)
")
5
Parotid gland: secretes watery (serous) saliva rich in enzymes
The peripheral branches of the facial nerve(CN VII) are intimately associated with the parotid gland. Stenson’s duct(on the buccal mucosa opposite to the maxillary second molar) Submandibular gland: serous and mucinous saliva Wharton’s duct(in the floor of the mouth on both sides of tongue frenulum ) Sublingual gland: secretes viscous saliva Multiple small ducts
 are intimately associated with the parotid gland. Stenson’s duct(on the buccal mucosa opposite to the maxillary second molar) Submandibular gland: serous and mucinous saliva. Wharton’s duct(in the floor of the mouth on both sides of tongue frenulum ) Sublingual gland: secretes viscous saliva. Multiple small ducts.")
6
Stinson's duct

7
Wharton's duct

8
(3)Sublingual fold with multiple sublingual gland openings
Sublingual fold with multiple sublingual gland openings")
9
MINOR SALIVARY GLANDS They lie just under mucosa.
Distributed over lips, cheeks ,posterior palate , floor of mouth & retro-molar area. Contribute 10% of total salivary volume.

10
SALIVA Healthy person secretes about ( 750-1500 ml of saliva / day)
FUNCTION OF SALIVA: 1\It facilitates swallowing 2\It keeps the mouth moist & aids speech 3\It serves as a solvent for molecules which stimulate the taste buds 4\It cleans the mouth, gum, & teeth. 5\It contains digestive enzymes

11
DIAGNOSTIC USES OF SALIVA:
1\The Use of Saliva Testing for Hormones 2\monitor drug use 3\screen for various diseases. 4\check for the presence of antibodies to the HIV virus. saliva is becoming a preferable diagnostic aid because it is the easiest to collect.

12
DISORDERS OF SALIVARY GLANDS
(1)OBSTRUCTIVE (2)FUNCTIONAL (3)INFECTIVE (4)CYSTS AND TUMORS
OBSTRUCTIVE. (2)FUNCTIONAL. (3)INFECTIVE. (4)CYSTS AND TUMORS.")
13
1\OBSTRUCTIVE SALIVARY GLAND DISEASE
Any Disease that causes obstruction of the ductal system of salivary glands. Tow major causes: 1-salivary calculi(stone) 2-duct strictures
 2-duct strictures.")
14
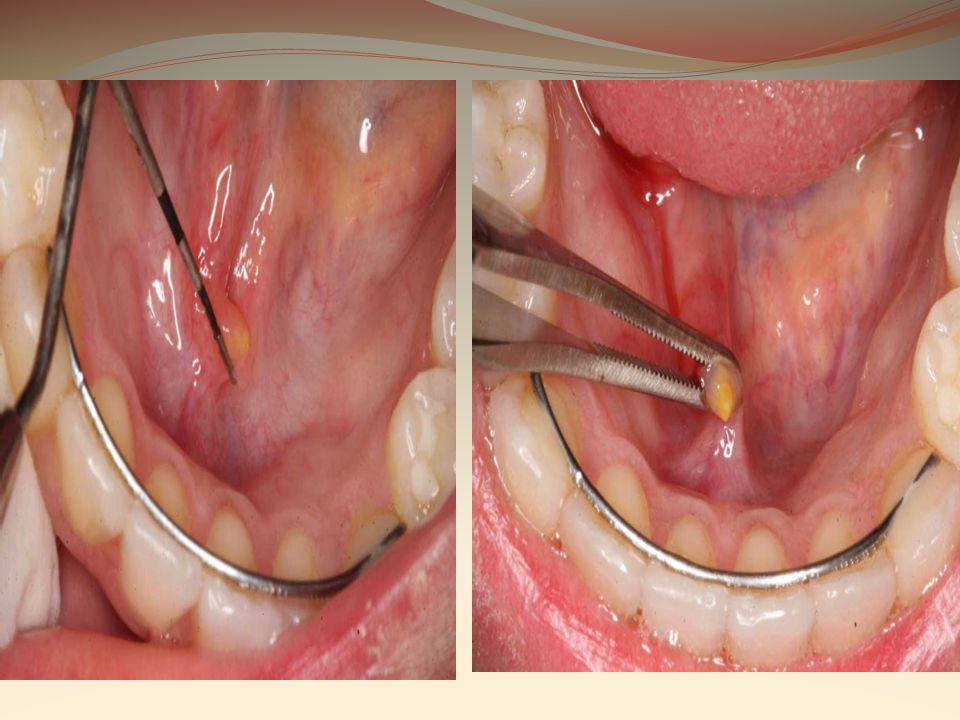
1\Salivary calculi CLINICAL FEATURES:
a stone can form in a salivary gland or duct 80% of salivary calculi form in the submandibular gland CLINICAL FEATURES: Usually the calculi are unilateral 1-The classical symptom is pain when the smell or taste of food stimulates salivary secretion. 2-ductal obstruction may lead to infection , pain and swelling of the gland 3-the stone can be seen and palpated in the floor of the mouth or can be deeply located and seen only in radiograph

16
DIAGNOSIS: MANAGEMENT: Sialography Removal of the calculi by
1\milking and manipulation out of the orifice 2\surgical incision

17
2\salivary duct strictures
Strictures means Narrowing of the duct or papilla of a gland Mainly seen in the parotid gland AETIOLOGY: Chronic trauma(E.G. from projecting clasps or faulty restorations )leading to fibrosis
leading to fibrosis.")
19
CLINICAL FEATURES: DIAGNOSIS: Same as salivary calculi
(pin and swelling during meal time-can be infected causing further painful swellings) DIAGNOSIS: Sialography TREATMENT: Removal of the cause Dilation of the duct by bougies
 DIAGNOSIS: Sialography. TREATMENT: Removal of the cause. Dilation of the duct by bougies.")
20
2\FUNCTIONAL DISORDERS
Disorders of saliva production Can be : 1\sialorrhea (increase salivary production) 2\xerostomia or dry mouth (decrease salivary production)
 2\xerostomia or dry mouth (decrease salivary production)")
21
1\sialorrhea AETIOLOGY:
Increase saliva production also known as hyper salivation It is not a significant complain as any excess saliva can readily be swallowed. AETIOLOGY: 1\local reflex to oral infections or ulcerations or new dentures 2\nausea 3\false sialorhea(normal salivary flow with lack of neuromuscular control that leads to drooling)
")
23
2\Xerostomia (dry mouth)
Reduction in saliva production AETIOLOGY: 1\ORGANIC CAUSE:(sjogren’s syndrome-irradiation) 2\FUNCTIONAL CAUSE:(dehydration- persistent diarrhea and vomiting –hemorrhage) 3\SOME DRUGS
 2\FUNCTIONAL CAUSE:(dehydration- persistent diarrhea and vomiting –hemorrhage) 3\SOME DRUGS.")
24
SJOGREN’S SYNDROME 1\PRIMARY SJOGREN’S SYNDROME:
Combination of dry mouth and dry eye 2\SECONDARY SJOGREN’S SYNDROME Combination of dry mouth ,dry eye associated with rheumatoid arthritis AETIOLOGY: Sjogren's syndrome is an auto immune disease

25
CLINICAL FEATURES: ORAL MANIFISTATIONS: 1\The oral mucosa becomes dry ,often red shiny. 2\The tongue is red and the dorsum becomes lobulated 3\Calculus accumulation and rapidly progressive dental caries

27
Oral effects of low salivary production:
1\discomfort 2\difficulties with eating or swallowing 3\disturbed taste sensation 4\disturbance of speech 5\predisposition to infections

28
OCULAR MANIFISTATIONS:
1\failure of tear secretion 2\inflammations in the eye 3\risk of vision loss

29
DIAGNOSIS: 1\low salivary flow rate 2\labial salivary gland biopsy 3\antibody screen TREATMENT: Salivary gland damage is irreversible Treat dry mouth with artificial saliva substitutes and frequent drinking of water Maintain good oral hygiene and caries control

30
3\INFECTIVE SALIVARY GLAND DISORDERS (SIALADENITIS)
CAN BE BACTERIAL,VIRAL OR FUNGAL THE MOST COMMON INFECTIVE DISEASES OF THE SALIVARY GLANDS: 1\mumps 2\suppurative parotitis

31
1\mumps AETIOLOGY: CLINICAL FEATURES:
Highly infectious salivary gland disease that causes painful swelling of the parotid gland and some times other glands. AETIOLOGY: Paramixovirus (mumps virus) CLINICAL FEATURES: 1\affect mainly children 2\headache , malaise ,fever and painful swelling of the parotids 3\permanent nerve damage may occur 4\after one infection the immunity is long lasting
 CLINICAL FEATURES: 1\affect mainly children. 2\headache , malaise ,fever and painful swelling of the parotids. 3\permanent nerve damage may occur. 4\after one infection the immunity is long lasting.")
33
DIAGNOSIS: Usually obvious from clinical manifestation Antibody screen MANAGEMENNT: Symptomatic treatment (analgesics- antipyretics) Supportive treatment (bed rest –fluid intake-warm or cold compress to the swollen glands to reduce the pain)
")
34
2\suppurative parotitis
It is a bacterial infection of one or both parotid glands AETIOLOGY: Staphylococcus aureus bacterial species Mostly seen in patients with severe xerostomia CLINICAL FEATURES: Pain on one or both parotid glands Swelling , redness and tenderness Pus exudates from the parotid duct If not treated may lead to abscess formation with fever and malaise.

36
DIAGNOSIS: Culture and sensitivity testing for the pus. TREATMENT: antibiotics

37
4\CYSTS AND TUMORS A)CYSTS OF SALIVARY GLANDS MUCOCELES:
The most common type of salivary cysts Affects minor salivary glands AETIOLOGY: Extravasations of saliva as result of damage to the duct of the salivary gland It is not a true cyst as it has no epithelial lining

38
CLINICAL FEATURES: Mucoceles most often form in the lower lip but occasionally on the buccal mucosa or floor of the mouth (mucoceles in the floor of the mouth is named ranula) Appear as rounded fleshy swelling about 1cm in diameter Then it become cystic ,hemispherical and bluish due to thin wall
 Appear as rounded fleshy swelling about 1cm in diameter. Then it become cystic ,hemispherical and bluish due to thin wall.")
39
ranula mucocele

40
TREATMENT: Surgical excision of the cyst with the underlying minor gland

41
B)TUMORS OF SALIVARY GLANDS
70% of salivary glands tumors develop in parotid gland and few affect the submandibular gland. Sublingual tumors are very rare. AETIOLOGY: Unknown but can result from irradiation to the head and neck region

42
CLASSIFICATION OF SALIVARY GLAND TUMORS:
S.G TUMORS EPETHELIAL BENIGN (ADENOMA) MALIGNANT (CARCINOMA) NON-EPETHELIAL SARCOMA LYMPHOMA
 MALIGNANT. (CARCINOMA) NON-EPETHELIAL. SARCOMA. LYMPHOMA.")
43
TYPICAL CLINICAL FEATURES OF SALIVARY GLAND TUMORS
BENIGN MALIGNANT 1-slowly growing 2-soft or rubbery in consistency 3-do not ulcerate 4-no associated nerve signs 1-fast growing and painful 2-hard consistency 3-may ulcerate and invade bone 4-cause cranial nerve palsies(dysfunction of the nerve affected)
")
44
Pleomorphic adenoma(benign)
Adenocarcinoma(malignant Pleomorphic adenoma(benign) Lymphoma(malignant)
 Lymphoma(malignant)")
45
DIAGNOSIS: MRI or CT-SCAN Biopsy and histological examination TRETMENT: 1\surgical excision for both malignant and benign tumors 2\if the tumor is malignant chemotherapy is indicated after excision

46
Thank you

Similar presentations



















.>")

 it is a tube with muscle walls throughout its length. it is lined by an epithelium.>")


