Download presentation
Presentation is loading. Please wait.

1
Knee Injuries Idan Ilsar, MD Arthroscopy and Sport Injury Unit
Department of Orthopaedic Surgery Hadassah – Hebrew University Medical Center

2
Today’s Menu Meniscal tears Anterior Cruciate Ligament (ACL) tears
Stress fractures

3
Meniscal injuries Prevalence …… (under-reported)
Surgical incidence is 60-70/100,000/y

4
Meniscal anatomy

5
Meniscal anatomy

6
Meniscal fibers orientation
Most of the collagen fibers aligned longitudinally Some fibers aligned radially - to hold the longitudinal fibers together These longitudinally oriented fibers allow for dissipation of compressive forces via hoop stresses

7
Meniscus In the past: “vestigial remnants of a muscle within the knee”
Meniscal tear “Cut it out”

8
Meniscus - functions In the present: Load sharers Shock absorber
Secondary knee stabilizers Proprioception Joint lubrication Nutrition of articular cartilage

9
Tears of medial meniscus > lateral meniscus
Meniscal motion in ROM Tears of medial meniscus > lateral meniscus LM>MM

10
Meniscal blood supply Peripheral 20-30% of MM Peripheral 10-25% of LM
Periphery White Red Peripheral 20-30% of MM Peripheral 10-25% of LM

11
Meniscal tears

12
Patient’s history (traumatic)
Twisting injury Swelling – after several hours-days (synovitis) Pain Limp Locking
 Pain. Limp. Locking.")
13
Physical examination Swelling Intra-articular fluid
Joint-line tenderness Locked knee (Quadriceps atrophy if prolonged)
")
14
McMurry Test

15
Apley’s Test

16
Imaging X-Ray Ultrasound CT Bone scan SPECT MRI

17
Knee x-ray AP (standing) Tunnel Lat
 Tunnel Lat")
18
Standing vs. Prone Rt Knee, 41y male

19
X- ray Knee alignment Osteoarthritis Osteonecrosis (AVN)
Chondrocalcinosis LBs (fracture)
")
20
Ultrasound Effusion Baker’s cyst Meniscal excursion But:
Operator – dependent Can’t visualize interior aspects

21
CT scan Fractures Dislocations

22
MRI

23
Treatment Analgesics NSAIDS Rest, Ice, Compression, Elevation
Elastic bandage Physical therapy

24
Arthroscopy

25
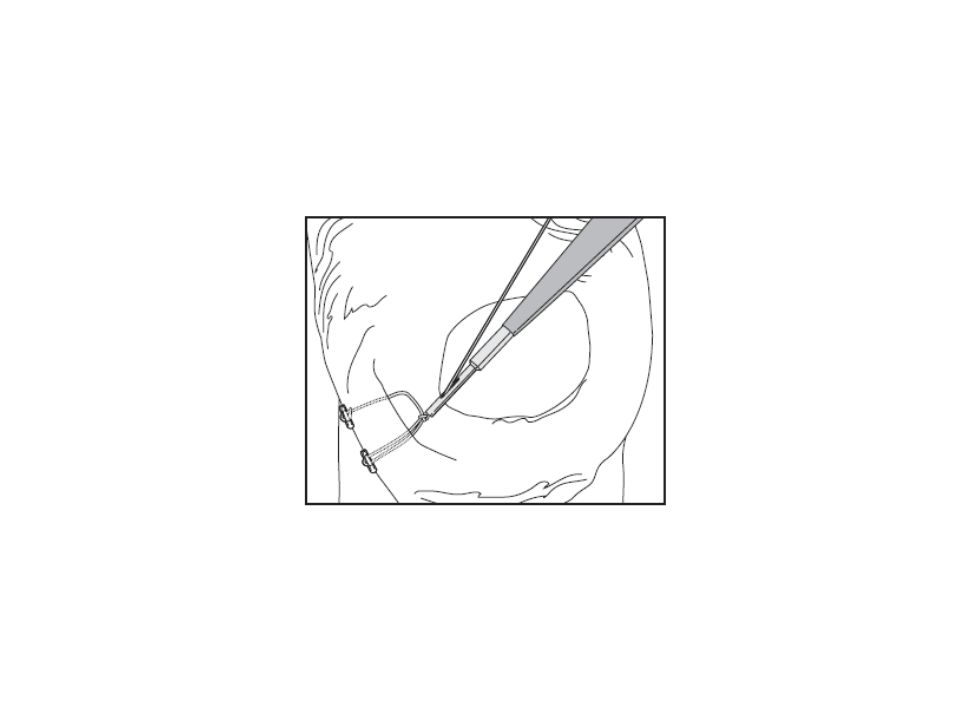
Outside-In repair

26
Suture meniscus

28
PHLM tear

29
PHMM tear

30
Future Options

31
Meniscus implant

32
ACL tear

33
ACL Anatomy ACL = two-bundle ligament small anteromedial
large posterolateral

34
ACL Mechanics The anteromedial band is tight in flexion, providing the primary restraint, whereas the posterolateral portion of this ligament is tight in extension.

35
ACL History and PE Incidence: 30 cases /100 000 people/ year
Noncontact deceleration, jumping, or cutting action Valgus-external rotation (hyperextension) A “pop” is frequently heard or felt Rapid swelling = hemarthrosis
 A pop is frequently heard or felt. Rapid swelling = hemarthrosis.")
36
Physical examination Test LACHMAN Anterior drawer PIVOT SHIFT

37
X-Ray SEGOND fracture avulsion fracture of the lateral capsule
pathognomonic of ACL tear

38
MRI Normal ACL

39
MRI ACL Tear

40
Treatment Non operative
If a nonoperative approach is chosen, it should include an aggressive rehabilitation program and counseling about activity level Early Rehab: Reduce swelling ROM Quad/Hamstrings

41
Treatment Non operative
The use of a functional knee brace is controversial and has not been shown to reduce the incidence of re-injury significantly if a patient returns to high-level sports

42
Treatment Operative Primary repair was advocated by some authors in the 1950s Although the short-term results were encouraging, long-term retrospective and prospective reviews showed that as many as 40% to 50% failed within 5 years.

43
Treatment : Operative ACL Reconstruction Extraarticular Intraarticular
Autografts : Patellar tendon Hamstring ligament double loop Allograft

44
ACL reconstruction Normal ACL Complete ACL tear= “empty notch”

45
ACL reconstruction surgery

46
Stress fracture

47
Overload injury Stress fracture
Etiology: More load More repeats Combination The emphasis is CHANGE

48
X Ray

49
Bone Scan

50
Pathophysiology Wolff’s Law: change in external stress leads to change in shape and strength of bone bone re-models in response to stress ABRUPT Increase in duration, intensity, frequency without adequate rest (re-modeling) Stress fracture: imbalance between bone resorption and formation Microfracture -> continued load -> stress fracture
 Stress fracture: imbalance between bone resorption and formation. Microfracture -> continued load -> stress fracture.")
51
Anatomic Location Tibia - 39.5% Metatarsals - 21.6% Fibula - 12.2%
Navicular - 8.0% Femur - 6.4% Pelvis - 1.9%

52
Tibial stress fracture
Local tenderness over middle – distal 1/3rd No swelling/redness

53
Treatment

54
IDF study Recruits Shoes, insoles, Biphosphonates – no reduction of SF incidence Good night sleep, length of marches – 60% reduction FINESTONE, A., and C. MILGROM. How Stress Fracture Incidence Was Lowered in the Israeli Army: A 25-yr Struggle. Med. Sci. Sports Exerc (11S):S623-S629
:S623-S629.")
55
Treatment "Rest"

56
“Rest” = relative rest Stationary cycling Elyptical Swimming
Avoid running/jumping

57
Return to sports סרגל מאמצים

58
“Cousin” of stress fractures
Shin Splints Medial tibial stress syndrome (MTSS) / tibial periostitis Runners, flat feet Tibia Diffuse tenderness “Cousin” of stress fractures Similar treatment
 / tibial periostitis. Runners, flat feet. Tibia. Diffuse tenderness. Cousin of stress fractures. Similar treatment.")
59
Thank you for listening

Similar presentations



>")















