Download presentation
Presentation is loading. Please wait.

1
The role of adjuvant TACE after curative liver resection for HCC
Anthony Fong Prince of Wales Hospital

2
Hepatocellular Carcinoma
5th most common cancer in the world > 500,000 new cases per year 600,000 people die globally due to HCC each year 1. Surgeon Jun;3(3):210-5. The continuing challenge of hepatic cancer in Asia. Lai EC, Lau WY. J Am Coll Surg Jul;205(1):27-36. 2. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74–108
: The continuing challenge of hepatic cancer in Asia. Lai EC, Lau WY. J Am Coll Surg Jul;205(1): Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, CA Cancer J Clin 2005; 55: 74–108.")
3
Curative treatment for HCC
Surgical resection / transplantation Loco-regional ablation Radiofrequency ablation Microwave ablation

4
Surgical resection Poor survival rate despite curative resection
5-year survivals of 39% - 50% High recurrence rate 1,3,5 years recurrence rate : 30.1%, 62.3%, 79% respectively 1. Lang H, Sotiropoulos GC, Brokalaki EI, Schmitz KJ, Bertona C, Meyer G, Frilling A, Paul A, Malagó M, Broelsch CE. Survival and recurrence rates after resection for hepatocellular carcinoma in noncirrhotic livers. J Am Coll Surg Jul;205(1):27-36. 2. Dupont-Bierre E, Compagnon P, Raoul JL, Fayet G, de Lajarte-Thirouard AS, Boudjema K. Resection of hepatocellular carcinoma in noncirrhotic liver: analysis of risk factors for survival. J Am Coll Surg 2005; 201: 663–70 3. mamura H, Matsuyama Y, Tanaka E et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol 2003; 38: 200–7.
: Dupont-Bierre E, Compagnon P, Raoul JL, Fayet G, de Lajarte-Thirouard AS, Boudjema K. Resection of hepatocellular carcinoma in noncirrhotic liver: analysis of risk factors for survival. J Am Coll Surg 2005; 201: 663– mamura H, Matsuyama Y, Tanaka E et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol 2003; 38: 200–7.")
5
Adjuvant Therapy

6
Adjuvant Therapy Adjuvant therapy: TACE Systemic chemotherapy
Immunotherapy Interferon Acyclic retinoid acid

7
TransArterial ChemoEmbolization
TACE TransArterial ChemoEmbolization

8
TACE Survival benefit in un-resectable HCC
? TACE as an adjuvant treatment Llovet JM, Bruix J Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival Hepatology 37:429, 2003

9
TACE as adjuvant therapy after curative liver resection

10
TACE as adjuvant therapy
Izumi R, Shimizu K, Iyobe T et al. Postoperative adjuvant hepatic arterial infusion of Lipiodol containing anticancer drugs in patients with hepatocellular carcinoma. Hepatology 1994; 20: 295–301. Lai EC, Lo CM, Fan ST, Liu CL, Wong J. Postoperative adjuvant chemotherapy after curative resection of hepatocellular carcinoma: a randomized controlled trial. Arch Surg 1998; 133: 183–8. Li Q, Wang J, Sun Y, Cui YL, Juzi JT, Qian BY, Hao XS. Postoperative transhepatic arterial chemoembolization and portal vein chemotherapy for patients with hepatocellular carcinoma: a randomized study with 131 cases. Dig Surg. 2006;23(4): Zhong C, Guo RP, Li JQ et al. A randomized controlled trial of hepatectomy with adjuvant transcatheter arterial chemoembolization versus hepatectomy alone for Stage IIIA hepatocellular carcinoma. J Cancer Res Clin Oncol 2009; 135: 1437–45. Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg 2009; 198: 313–8.
: Zhong C, Guo RP, Li JQ et al. A randomized controlled trial of hepatectomy with adjuvant transcatheter arterial chemoembolization versus hepatectomy alone for Stage IIIA hepatocellular carcinoma. J Cancer Res Clin Oncol 2009; 135: 1437–45. Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg 2009; 198: 313–8.")
11
TACE as adjuvant therapy
Patient selection – tumor extent Timing for TACE Chemotherapy agent Side effects

12
Patient selection for adjuvant TACE

13
TMN Staging for HCC T-staging N-staging M-staging
T1 - Solitary tumor without vascular invasion T2 - Solitary tumor with vascular invasion or multiple tumors none more than 5 cm T3 - Multiple tumors more than 5 cm or tumor involving a major branch of the portal or hepatic vein(s) T4 - Tumor(s) with direct invasion of adjacent organs other than the gallbladder or with perforation of visceral peritoneum N-staging N0 - Indicates no nodal involvement N1 - Indicates regional nodal involvement M-staging M0 - Indicates no distant metastasis M1 - Indicates metastasis presence beyond the liver Overall Staging Stage I T1 N0 M0 Stage II T2 Stage IIIA Stage IIIB Stage IIIC T3 T4 Tx N1 Stage IV Nx M1
 T4 - Tumor(s) with direct invasion of adjacent organs other than the gallbladder or with perforation of visceral peritoneum. N-staging. N0 - Indicates no nodal involvement. N1 - Indicates regional nodal involvement. M-staging. M0 - Indicates no distant metastasis. M1 - Indicates metastasis presence beyond the liver. Overall Staging. Stage I. T1. N0. M0. Stage II. T2. Stage IIIA Stage IIIB Stage IIIC. T3. T4. Tx. N1. Stage IV. Nx. M1.")
14
Median observation time (mths) Disease free survival (Tx vs Ctrl)
Author Tumor extent Sample size (Tx / Ctrl) Median observation time (mths) Disease free survival (Tx vs Ctrl) Overall survival Izumi (1994) Vessel involvement / intrahepatic spreading 50 (23/27) 28.7 1 yr 64.5% vs 43% 87% vs 81% 3 yr 32% vs 11.7% 50.3% vs28.8% Lai (1998) Negative in Lipiodol CT, Angiography and USG 1 mth after OT 66 (30/36) 28.3 50% vs 69% 65% vs 67% 18% vs 48% Li (2006) Solitary / Multiple tumor in one liver lobe 84 (39/45) Not mentioned 87.2% vs86.5% Not stated 60.7% vs47.8% Zhong (2009) Stage IIIa disease 118 (59/59) 20 29.7% vs 14% 80.7% vs56.5% 9.3% vs 3.5% 33.3% vs19.4% Peng HCC with PVTT (main or opposite branch <3 cm) 104 (51/53) 33.6 50.9% vs33.3% 33.8% vs 17% p = p = p = 0.04 p = 0.10 p = 0.345 p = 0.004 p = 0.048 p =
 Median observation time (mths) Disease free survival. (Tx vs Ctrl) Overall survival. Izumi. (1994) Vessel involvement / intrahepatic spreading. 50 (23/27) yr. 64.5% vs 43% 87% vs 81% 3 yr. 32% vs 11.7% 50.3% vs28.8% Lai. (1998) Negative in Lipiodol CT, Angiography and USG 1 mth after OT. 66 (30/36) % vs 69% 65% vs 67% 18% vs 48% Li. (2006) Solitary / Multiple tumor in one liver lobe. 84 (39/45) Not mentioned. 87.2% vs86.5% Not stated. 60.7% vs47.8% Zhong. (2009) Stage IIIa disease. 118 (59/59) % vs 14% 80.7% vs56.5% 9.3% vs 3.5% 33.3% vs19.4% Peng. HCC with PVTT (main or opposite branch <3 cm) 104 (51/53) % vs33.3% 33.8% vs 17% p = p = p = p = p = p = p = p =")
15
Patient selection for adjuvant TACE
High risk tumor Tumor size (>5 cm) Vascular invasion Multiple tumor nodules
 Vascular invasion. Multiple tumor nodules.")
16
Timing for TACE

17
Timing for TACE Author Interval between TACE and surgery
Number of courses Outcome Izumi (1994) 21-84 days 1 Improved DFS Lai (1998) Both TACE and systemic chemo Mean : 50 days 3 course of TACE 2 monthly 8 doses of systemic chemo 6-weekly Decreased DFS Li (2006) 4 weeks 3 Course , 2 weekly No sig. difference in DFS Zhong (2009) 4-6 weeks Improve DFS and OS Peng (2009) 3-4 weeks, repeated once every 1-2 month 2-5 Improved OS
 days. 1. Improved DFS. Lai (1998) Both TACE and systemic chemo. Mean : 50 days. 3 course of TACE 2 monthly. 8 doses of systemic chemo 6-weekly. Decreased DFS. Li (2006) 4 weeks. 3 Course , 2 weekly. No sig. difference in DFS. Zhong (2009) 4-6 weeks. Improve DFS and OS. Peng (2009) 3-4 weeks, repeated once every 1-2 month Improved OS.")
18
Timing for TACE 4 weeks after hepatectomy
Single course already showed survival benefit

19
Chemotherapy agent

20
Agent for TACE Author TACE Agent Outcome Izumi (1994)
(20mg/m2) + Mitomycin C (10mg/m2), Lipiodol (3ml) Improved DFS Lai (1998) Systemic chemo : Epirubicin hydrochloride (40mg/m2) TACE : (10mg), Lipiodol (10ml) Decreased DLS Li (2006) (30mg), Mitomycin (20mg), (80-100mg) / (400mg) No sig. difference in DFS Zhong (2009) (200mg/m2), Mitomycin (6mg/m2), Lipiodol (4-5ml), hydrocholride (40mg/m2) Improve DFS and OS Peng (2009) 5-FU (500mg/m2), (30mg/m2), Lipiodol (10-20ml) Improved OS Doxorubicin Cisplatin Doxorubicin Cisplatin Carboplatin Carboplatin Epirubicin Doxorubicin
 + Mitomycin C (10mg/m2), Lipiodol (3ml) Improved DFS. Lai (1998) Systemic chemo : Epirubicin hydrochloride (40mg/m2) TACE : (10mg), Lipiodol (10ml) Decreased DLS. Li (2006) (30mg), Mitomycin (20mg), . (80-100mg) / (400mg) No sig. difference in DFS. Zhong (2009) (200mg/m2), Mitomycin (6mg/m2), Lipiodol (4-5ml), hydrocholride (40mg/m2) Improve DFS and OS. Peng (2009) 5-FU (500mg/m2), (30mg/m2), Lipiodol (10-20ml) Improved OS. Doxorubicin. Cisplatin. Doxorubicin. Cisplatin. Carboplatin. Carboplatin. Epirubicin. Doxorubicin.")
21
Agent for TACE Doxorubicin (Adriamycin) / Epirubicin Mitomycin 5-FU
Cisplatin / Carboplatin

22
Agents for TACE Cleared rapidly by the liver. Large difference in concentration between the liver and systemic circulation Effective primarily at high doses

23
Side effects

24
Author Side effects Serious side effects Izumi (1994) Fever, nausea Hepatic injury required ICU care, Biloma Lai (1998) Cellulitis Necrosis of lesser curve of stomach Li (2006) Nausea and loss of appetite, impaired liver function, leukopenia and thrombocytopenia. NIL Zhong (2009) Nausea / Vomiting (50.9%), Increase ALT (29.8%), Pain (19%), Increase in bilirubin (19%), Leukopenia (1.8%) Peng (2009) Fever (86%) , vomiting (66%), poor appetite (52%), Fatique (39%%)
 Cellulitis. Necrosis of lesser curve of stomach. Li (2006) Nausea and loss of appetite, impaired liver function, leukopenia and thrombocytopenia. NIL. Zhong (2009) Nausea / Vomiting (50.9%), Increase ALT (29.8%), Pain (19%), Increase in bilirubin (19%), Leukopenia (1.8%) Peng (2009) Fever (86%) , vomiting (66%), poor appetite (52%), Fatique (39%%)")
25
Side effects Fever Nausea / vomiting Impaired liver function
Leukopenia Pain Local complications

26
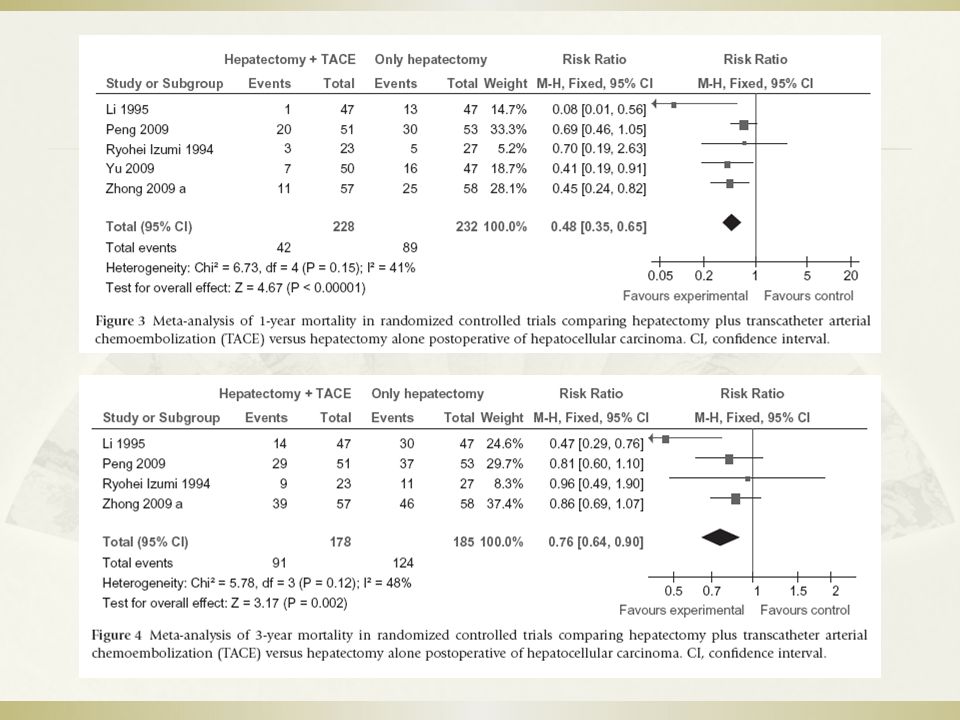
Meta-analysis

28
Meta-analysis - Abstract

29
Our experience

30
Our experience 13 Patients underwent adjuvant TACE after liver resection of curative intent Criteria of adjuvant TACE : Large tumor (>5 cm) Satellite nodules Vascular invasion Close surgical margin
 Satellite nodules. Vascular invasion. Close surgical margin.")
31
Duration between OT and TACE
Operation Tumor size (cm) Margin (cm) Vascular invasion Multiple tumor Duration between OT and TACE Disease Free survival Overall Survival FU peroid (mth) Seg6 /7 Wedge resection 5.1 1.5 Y N 4 3 Right hepatectomy 3.5 0.3 8 7 Lap Seg 5 wedge resection 6 9 4.3 10 14 Left Hepatectomy 0.5 3.2 5.8 15 0.2 7.5 5 17 1 20 28 30 38 43
 Margin (cm) Vascular invasion. Multiple tumor. Duration between OT and TACE. Disease Free survival. Overall Survival. FU peroid (mth) Seg6 /7 Wedge resection Y. N Right hepatectomy Lap Seg 5 wedge resection Left Hepatectomy")
32
Our experience Follow up peroid 3-43 mths (median 15mths) Tumor Size
1.5 – 14cm (Median 5.1cm) Vascular invasion 61.5% Surgical margin cm (Median 1cm) Presence of multiple tumors 46%
 Vascular invasion. 61.5% Surgical margin cm (Median 1cm) Presence of multiple tumors. 46%")
33
Our experience 2 Patients had recurrence (15%)
Both from lung metastasis Disease free survival : 3 mths / 15 mths 1 mortality from recurrence (Overall survival 15mths)
")
34
Conclusion Role of adjuvant TACE after curative liver resection is still controversial Some trials showed promising results in patients with advanced disease TACE is well tolerated in most studies Need further large scale study for evaluation

35
Thank you

Similar presentations








 for Liver Tumour Dr Dai Wing Chiu Queen Mary Hospital.>")










