Download presentation
Presentation is loading. Please wait.

1
Project: Ghana Emergency Medicine Collaborative Document Title: Pulmonary Embolism Part 2 (2012) Author(s): Rockefeller A. Oteng, M.D., University of Michigan License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike-3.0 License: http://creativecommons.org/licenses/by-sa/3.0/ We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. These lectures have been modified in the process of making a publicly shareable version. The citation key on the following slide provides information about how you may share and adapt this material. Copyright holders of content included in this material should contact open.michigan@umich.edu with any questions, corrections, or clarification regarding the use of content. For more information about how to cite these materials visit http://open.umich.edu/privacy-and-terms-use. Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition. Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers. 1

2
Attribution Key for more information see: http://open.umich.edu/wiki/AttributionPolicy Use + Share + Adapt Make Your Own Assessment Creative Commons – Attribution License Creative Commons – Attribution Share Alike License Creative Commons – Attribution Noncommercial License Creative Commons – Attribution Noncommercial Share Alike License GNU – Free Documentation License Creative Commons – Zero Waiver Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in your jurisdiction may differ Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105) Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair. To use this content you should do your own independent analysis to determine whether or not your use will be Fair. { Content the copyright holder, author, or law permits you to use, share and adapt. } { Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. } { Content Open.Michigan has used under a Fair Use determination. } 2
) *laws in your jurisdiction may differ Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105) Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair. To use this content you should do your own independent analysis to determine whether or not your use will be Fair. { Content the copyright holder, author, or law permits you to use, share and adapt. } { Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. } { Content Open.Michigan has used under a Fair Use determination. } 2.")
3
Pulmonary Embolism Part 2 Rockefeller A. Oteng Ghana Emergency Medicine Collaborative

4
Diagnostic Evaluation Wells Clinical Prediction Rule for Pulmonary Embolism (PE) Clinical feature Points Clinical symptoms of DVT 3 Other diagnosis less likely than PE 3 Heart rate greater than 100 beats per minute 1.5 Immobilization or surgery within past 4 weeks 1.5 Previous DVT or PE 1.5 Hemoptysis 1 Malignancy 1 Total points PE = pulmonary embolism; DVT = deep venous thrombosis. Risk score interpretation (probability of PE): >6 points: high risk (78.4%); 2 to 6 points: moderate risk (27.8%); <2 points: low risk (3.4%)
: >6 points: high risk (78.4%); 2 to 6 points: moderate risk (27.8%); <2 points: low risk (3.4%).")
5
Diagnostic Evaluation Wells Clinical Prediction Rule for Deep Venous Thrombosis (DVT) Clinical featurePoints Active cancer (treatment within 6 months, or palliation) 1 Paralysis, paresis, or immobilization of lower extremity 1 Bedridden for more than 3 days because of surgery (within 4 weeks) 1 Localized tenderness along distribution of deep veins 1 Entire leg swollen 1 Unilateral calf swelling of greater than 3 cm (below tibial tuberosity) 1 Unilateral pitting edema1 Collateral superficial veins1 Alternative diagnosis as likely as or more likely than DVT -2 Total points DVT = deep venous thrombosis. Risk score interpretation (probability of DVT): >/=3 points: high risk (75%); 1 to 2 points: moderate risk (17%); <1 point: low risk (3%).
: >/=3 points: high risk (75%); 1 to 2 points: moderate risk (17%); <1 point: low risk (3%)..")
6
Diagnostic Evaluation Laboratory: – Routine laboratory findings are nonspecific. – Include leukocytosis – Increased erythrocyte sedimentation rate (ESR), and an elevated serum LDH or AST (SGOT) – normal serum bilirubin.
, and an elevated serum LDH or AST (SGOT) – normal serum bilirubin..")
7
Diagnostic Evaluation Arterial blood gas – Arterial blood gas (ABG) measurements and pulse oximetry have a limited role in diagnosing PE. – ABGs usually reveal hypoxemia Hypocapnia, Respiratory alkalosis.

8
Diagnostic Evaluation Troponin : – Serum troponin I and troponin T are elevated in 30 to 50 percent of patients who have a moderate to large pulmonary embolism. – Presumed mechanism is acute right heart overload. Brain Naturetic Peptide: – Very non specific peptide – Large elevation can suggest poor prognosis

9
Diagnostic Evaluation Electrocardiogram – ECG abnormalities common in patients with and without PE – limiting the diagnostic usefulness of the ECG – Most common Ekg finding is a sinus tachycardia Or non specific ST and T wave changes – abnormalities historically considered to be suggestive of PE S1Q3T3 pattern, right ventricular strain, new incomplete right bundle branch block

10
Diagnostic Evaluation V/Q scan : – The most extensive evaluation of the accuracy of the ventilation-perfusion (V/Q) scan was the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) – Accuracy was based on comparison with the gold standard test of Pulmonary angiogram – The found clincally accuracy was best when combined with pretest probabilities
 scan was the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) – Accuracy was based on comparison with the gold standard test of Pulmonary angiogram – The found clincally accuracy was best when combined with pretest probabilities")
11
Diagnostic Evaluation V/Q scan : Patients with high clinical probability of PE and a high-probability V/Q scan had a 95 percent likelihood of having PE Patients with low clinical probability of PE and a low-probability V/Q scan had only a 4 percent likelihood of having PE A normal V/Q scan virtually excluded PE

12
Diagnostic Evaluation Ultrasound: – In some patients clinicians have attempted to use lower extremity Doppler's to evaluate – Studies show that many patients with PE are missed – Bilateral lower extremity doppler’s will decrease the rate of missed DVT – Operator dependent

13
Diagnostic Evaluation D-dimer: – D-dimer is a degradation product of cross-linked fibrin. It can be detected in serum using a variety of different assays: – Enzyme-linked immunosorbent assay (ELISA) (results in >8 hrs) – Quantitative rapid ELISA (results in 30 min) – Semi-quantitative rapid ELISA (results in 10 min) – Qualitative rapid ELISA (results in 10 min) – Quantitative latex agglutination assay (results in 10 to 15 min) – Semi-quantitative latex agglutination assay (results in 5 min)
 (results in >8 hrs) – Quantitative rapid ELISA (results in 30 min) – Semi-quantitative rapid ELISA (results in 10 min) – Qualitative rapid ELISA (results in 10 min) – Quantitative latex agglutination assay (results in 10 to 15 min) – Semi-quantitative latex agglutination assay (results in 5 min).")
14
Diagnostic Evaluation D-Dimer: For the quantitative assays, a level >500 ng/mL is usually considered abnormal They are best characterized as having good sensitivity and negative predictive value Poor specificity and positive predictive value.

15
Diagnostic Evaluation Angiography : – Pulmonary angiography is the definitive diagnostic technique or "gold standard" in the diagnosis of acute PE. – It is performed by injecting contrast into a pulmonary artery branch after percutaneous catheterization, usually via the femoral vein. A filling defect or abrupt cutoff of a small vessel is indicative of PE.

16
Diagnostic Evaluation Angiography: – A negative pulmonary angiogram excludes clinically relevant PE. – Pulmonary angiography is generally safe and well tolerated in the absence of hemodynamic instability caused by acute, severe pulmonary hypertension – Radiation exposure depends on the length and complexity of the procedure, and greater than CT.

17
Source Undetermined

18
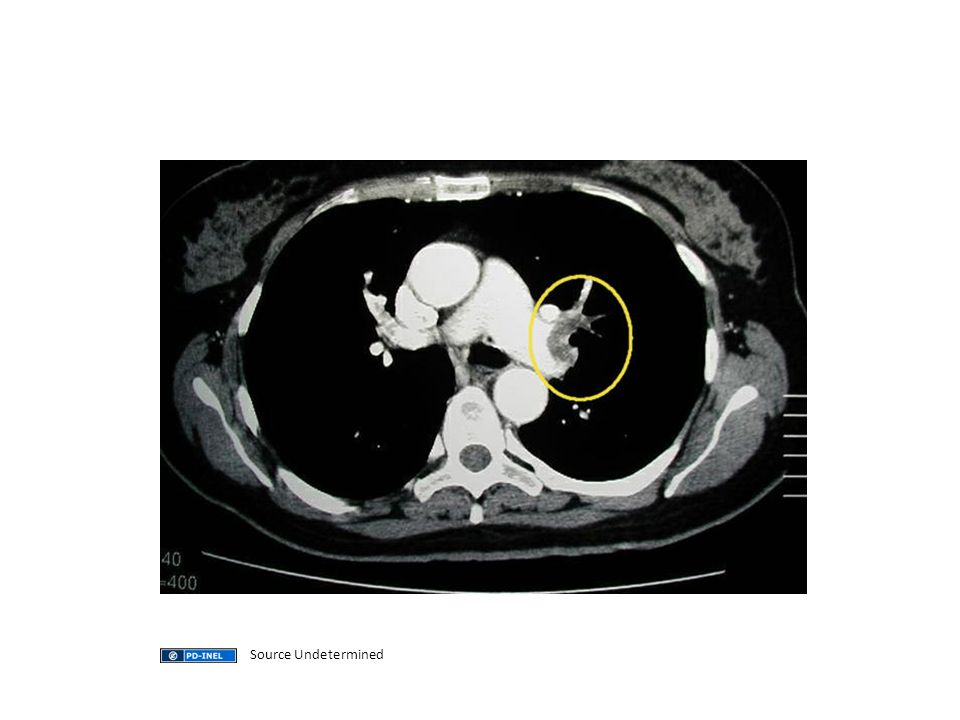
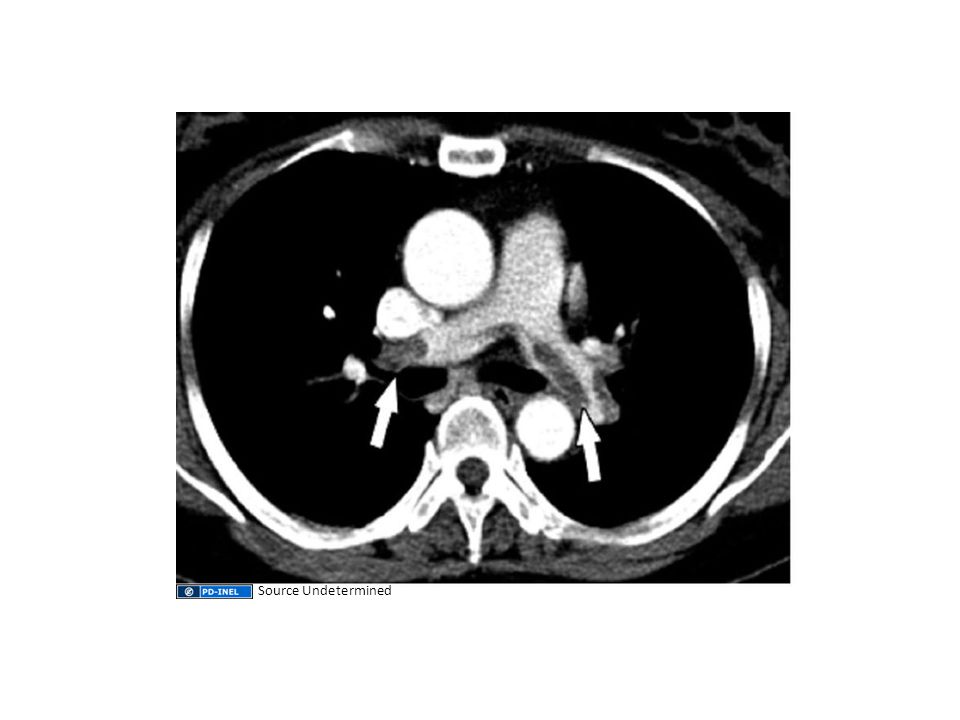
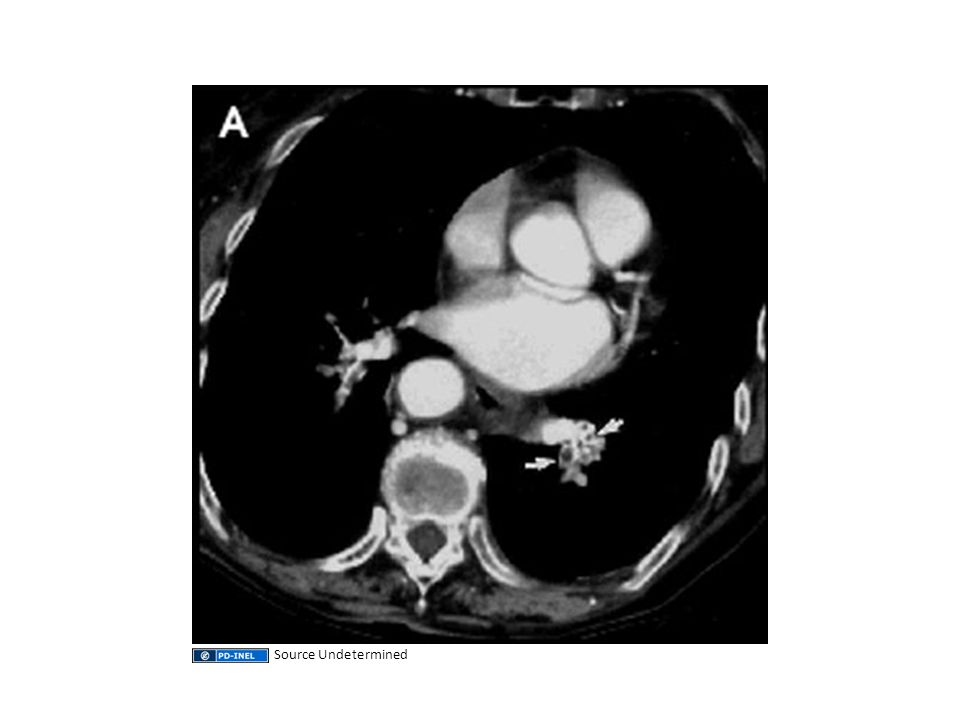
Diagnostic Evaluation Spiral CT: – Spiral (helical) CT scanning with intravenous contrast ( CT pulmonary angiography or CT-PA) is being used increasingly as a diagnostic modality for patients with suspected PE – Initial reports suggested that 98 percent of patients with PE were detected by CT-PA; however, that value decreased to 53 to 87 percent in subsequent studies
 CT scanning with intravenous contrast ( CT pulmonary angiography or CT-PA) is being used increasingly as a diagnostic modality for patients with suspected PE – Initial reports suggested that 98 percent of patients with PE were detected by CT-PA; however, that value decreased to 53 to 87 percent in subsequent studies")
19
Source Undetermined

23
PERC The following eight factors constitute the PE rule-out criteria (PERC): Age less than 50 years Heart rate less than 100 bpm Oxyhemoglobin saturation ≥95 percent No hemoptysis No estrogen use No prior DVT or PE No unilateral leg swelling No surgery or trauma requiring hospitalization within the past four weeks
: Age less than 50 years Heart rate less than 100 bpm Oxyhemoglobin saturation ≥95 percent No hemoptysis No estrogen use No prior DVT or PE No unilateral leg swelling No surgery or trauma requiring hospitalization within the past four weeks")
Similar presentations

: Prachi Agarwal M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Non-commercial–Share.>")
: Don M. Blumenthal, 2010 License: Unless otherwise noted, this material is made available under the terms of the Attribution – Non-commercial.>")
: Paul Conway, 2008-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")
: Michael Hortsch, Ph.D., 2010 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")
: Caroline Richardson, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Noncommercial–Share.>")
: Gerald Abrams, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Non-commercial–Share.>")
: John Doe, MD; Jane Doe, PhD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")
: John Doe, MD; Jane Doe, PhD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")

: Paul Conway, 2008-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")
: Prof. John T. Kakitahi, 2009-2012 Resource.>")
: Rockefeller A. Oteng (University of Michigan), MD 2012 License:>")

: Seetha Monrad, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Noncommercial–Share.>")
: University of Michigan Department of Emergency Medicine.>")
: Peter Moyer (Boston University), MD, MPH 2012 License: Unless otherwise.>")
: Dr. Roy William Mayega (Makerere.>")
: Brenda Gunderson, Ph.D., 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Non-commercial–Share.>")
