Download presentation
Presentation is loading. Please wait.

1
Prenatal Care, Labor and Delivery
Susan M. Goltz, MD Northland OB/GYN

2
Objectives: 1. Review the anatomy and physiology of pregnancy.
2. Understand the basic evaluation and follow up of prenatal care. 3. Prepare for observation of the labor and delivery process and for your third year clinical rotation. 4. Have notes that you can review prior to the board examination.

3
Birth Statistics The number of births in the United States in was 4,116,000. The birth rate per 1,000 population was 14.1 in This compares to a high of 25 in and a low of 13.9 in 2002. The maternal mortality in 2004 was 540 in the United States. This rate may actually be higher but not all maternal deaths relating to obstetrical causes are reported. The leading causes of maternal death are hemorrhage, pulmonary embolism and pregnancy induced hypertension.

4
Birth Statistics The infant mortality rate is the number of infant deaths in the first year of life divided by the number of live births that year. It is reported per 1,000 live births so that different countries can be compared. In 2006 in the United States the IMR was 6.3.

5
Infant Mortality Rates in 2006
Rank Country Infant mortality rate (deaths/1,000 live births) 1 Angola 182.31 2 Sierra Leone 156.48 3 Afghanistan 154.67 4 Liberia 143.89 5 Niger 115.42 218 Iceland 3.25 219 Hong Kong 2.93 220 Japan 2.80 221 Sweden 2.75 222 Singapore 2.30
 1. Angola Sierra Leone Afghanistan Liberia Niger Iceland Hong Kong Japan Sweden Singapore")
6
Female Reproductive Anatomy
Vagina and perineum: increased vascularity and hyperemia are hallmarks of pregnancy. Vaginal wall smooth muscle hypertrophies and vaginal and cervical secretions increase. These changes are associated with one of the earliest physical signs of pregnancy: Chadwick’s sign is the change in color of the cervix and vagina to a purplish red or a dark blue due to the hyperemia of the tissues.

7
Female Reproductive Anatomy
The other named physical sign of early pregnancy is Hegar’s sign. Hegar’s sign occurs with the softening of the uterus in early pregnancy which leads to a “disappearance” of the isthmus between the cervix and the uterus when performing a bimanual examination.

8
Female Reproductive Anatomy
The ovaries become quiet during pregnancy: ovulation and follicle production stops. A single corpus luteum functions to support the pregnancy with progesterone production during the first 6-7 weeks of the pregnancy. The nonpregnant uterus weighs about 70 grams and has a capacity of 10 ml or less. The pregnant uterus contains a volume which averages 5 L but can be as much as 4 X that. The term uterus weighs about 1,100 grams.

9
Female Reproductive Anatomy
The mechanism of uterine growth is the stretching and hypertrophy of the myometrial cells. At about 12 weeks gestation the uterus can be palpated above the symphysis pubis. The abdominal wall stretches to accomodate the enlarging uterus. Striae gravidarum occur in about half of all pregnant women. These reddish streaks develop in the skin of the abdomen and sometimes in the skin over the breasts and thighs. They become silvery over time.

10
Female Reproductive Anatomy
Diastasis recti occurs when the muscles of the abdominal wall separate in the midline. The midline of the abdominal skin becomes darker during pregnancy. This is known as the linea nigra. Irregular brownish patches may occur on the skin of the face and neck causing the mask of pregnancy (chloasma or melasma gravidarum).
.")
11
Female Reproductive Anatomy
In early pregnancy the breasts become sensitive and tender. After the second month the breasts increase in size and become nodular.

12
Physiology of Pregnancy
Profound hemodynamic changes include the increase in plasma volume and an increase in cardiac output. These changes begin very early in pregnancy and persist until after delivery. The plasma volume increases by 40-50% and the red cell mass increases by only about 25%. This relative increase in plasma volume causes a decrease in the hemoglobin concentration – the physiologic anemia of prenancy.

13
Physiology of Pregnancy
As cardiac output increases and peripheral resistance decreases blood pressures drop during pregnancy. Toward the end of the pregnancy vasoconstriction occurs causing a rise in blood pressure. Respiratory changes in pregnancy can be attributed to three main factors: the mechanical effects of the enlarging uterus, the increased total body oxygen consumption and the stimulant effects of progesterone.

14
Physiology of Pregnancy
Total body oxygen consumption increases about percent in pregnancy. This is accompanied by mechanisms that support oxygen delivery: increases in cardiac output and alveolar ventilation. Most pregnant women have dyspnea. Pulmonary function tests are usually normal. It is thought that the dyspnea may be due to a marked change in the PCO2 which occurs in these women.

15
Physiology of Pregnancy
Renal plasma flow and the GFR increase early in pregnancy and plateau at about a 40% increase by the middle of the pregnancy. This results in lower levels of creatinine and urea in the serum. The insulin response is increased in early pregnancy and then insulin resistance emerges. If the resistance is great the patient is diagnosed with gestational diabetes.

16
Physiology of Pregnancy
The average weight gain of pregnancy is 12,500 gms (28 lbs.) Tissues and fluids Increase in weight (gms) Fetus 3400 Placenta 650 Amniotic fluid 800 Uterus 970 Breasts 405 Blood 1250 Interstitial fluid 1680 Maternal stores 3345 TOTAL 12,500 gms
 Tissues and fluids. Increase in weight (gms) Fetus Placenta Amniotic fluid Uterus Breasts Blood Interstitial fluid Maternal stores TOTAL. 12,500 gms.")
17
Prenatal Care The symptoms of pregnancy include amenorrhea, nausea, fatigue and breast tenderness. The confirmation of pregnancy is made by testing the urine or blood for human chorionic gonadotropin or a beta HCG. Other confirming tests include the detection of FHT’s by ausculation or visualization of a fetus on ultrasound.

18
Prenatal Care The objectives of prenatal care as defined by the American College of OB/GYN (ACOG) are to prevent and manage those conditions that cause poor pregnancy outcomes. These conditions include premature labor and delivery, IUGR, birth defects, hypertension, diabetes, perinatal infections and post-term pregnancy.
 are to prevent and manage those conditions that cause poor pregnancy outcomes. These conditions include premature labor and delivery, IUGR, birth defects, hypertension, diabetes, perinatal infections and post-term pregnancy.")
19
Prenatal Care The first visit consists of a thorough history with special emphasis on the menstrual history, contraceptive history and previous pregnancies. Medical, surgical and social histories are also important. Dating of the pregnancy is determined using Nagele’s rule: LNMP minus three months plus seven days This calculation is based on a 28 day cycle.

20
Prenatal Care The physical examination should be performed early in the pregnancy (before 12 weeks gestation) for accurate assessment of the uterine size to assist in dating the pregnancy. A pelvic examination as well as a thorough general examination is performed. Clinical pelvimetry is no longer emphasized.
 for accurate assessment of the uterine size to assist in dating the pregnancy. A pelvic examination as well as a thorough general examination is performed. Clinical pelvimetry is no longer emphasized.")
21
Prenatal Care Laboratory studies include cervical cytology, screening for gonorrhea and chlamydia, a CBC, UA/UC, blood group, Rh factor and an antibody screen. A test for syphilis is mandated by law in almost all states. A rubella antibody screen is recommended. Testing for HIV and Hepatitis B is also recommended.

22
Prenatal Care A thorough discussion about options for genetic testing must occur. The options for genetic testing include the following screening tests: First Trimester Screening, Quad Screen and Cystic Fibrosis testing. Diagnostic testing for genetic abnormalities include chorionic villus sampling and a genetic amniocentesis.

23
Prenatal Care Ultrasound
An ultrasound for dating is usually done at the first visit between 8-12 weeks. This is not necessary if the LNMP dating is based on a reliable history and if the exam between 8-12 weeks concurs with that dating. An earlier US may have been performed if the patient has a history of previous pregnancy loss or had a threatened abortion. An US at about 20 weeks gestation confirms the EDC, allows us to view the placental location and is an anomaly screen. Ultrasounds for dating become less accurate as the pregnancy progresses.

24
Prenatal Care Prenatal visits are arranged depending on the history and risk status of the patient. In general, the visits are every 4 weeks until 28 weeks, then every 2 weeks until 36 weeks and then weekly after that. At every visit a weight, BP, urine for glucose and protein are checked. FHT’s are auscultated or visualized on an US. The size of the uterus is estimated. An examination is performed (Leopold’s maneuvers) to estimate the presentation of the baby. Cervical exams are performed at 28 weeks to assess the risk for preterm birth and then at 36 weeks to confirm the presentation and to assess cervical change.
 to estimate the presentation of the baby. Cervical exams are performed at 28 weeks to assess the risk for preterm birth and then at 36 weeks to confirm the presentation and to assess cervical change.")
25
Leopold’s Maneuvers Leopold’s Manuevers

26
Prenatal Care Laboratory testing later in the pregnancy includes a glucose screen at about 28 weeks and group B strep testing at 36 weeks. Periodic Hgb checks are performed during the pregnancy depending on the history and previous values.

27
Labor – what causes it? On a molecular basis intracellular calcium concentration increases to trigger an enzymatic process that brings the actin protein structure to the myosin protein structure in the cytoplasm in the smooth muscle cells of the uterus. Gap junctions form along two smooth muscle cell interfaces. This allows communication between the cells which in turn allows the uterus to contract as a whole.

28
Labor Mechanisms of labor are the processes of accommodation of the fetus to the bony passage. The size and shape of the female pelvis are extremely important in obstetrics. The adult pelvis is comprised of the sacrum, the coccyx and two innominate bones. Each innominate bone is formed by the fusion of the ilium, the ischium, and the pubis.

29
Bone Structure of the Female Pelvis

30
Bone Structure of the Male Pelvis

31
Labor Labor is defined as progressive cervical effacement and dilatation resulting from regular uterine contractions. There are three stages of labor: First stage: begins with the onset of regular contractions and lasts until the cervix is completely dilated. Second stage: begins with complete dilatation and ends with the delivery of the baby. Third stage: delivery of the placenta and inspection and repair of the vagina, cervix and perineum.

32
Cervical Dilatation and Effacement

33
Cervical Dilatation and Effacement

34
Labor The mechanisms of labor that allow the baby to adapt to the pelvis during the second stage are as follows: descent, flexion, internal rotation, extension, external rotation and expulsion. Descent occurs progressively – the other movements are superimposed upon it.

35
Mechanism of Labor

36
Labor It is important to determine the presentation of the fetus.
The presenting part is determined by an abdominal examination, a cervical examination or an ultrasound. Common presentations include vertex, face, brow, shoulder and breech. Vertex presentations are usually occiput anterior. However, they can be occiput transverse or occiput posterior.

37
Fetal Presentations

39
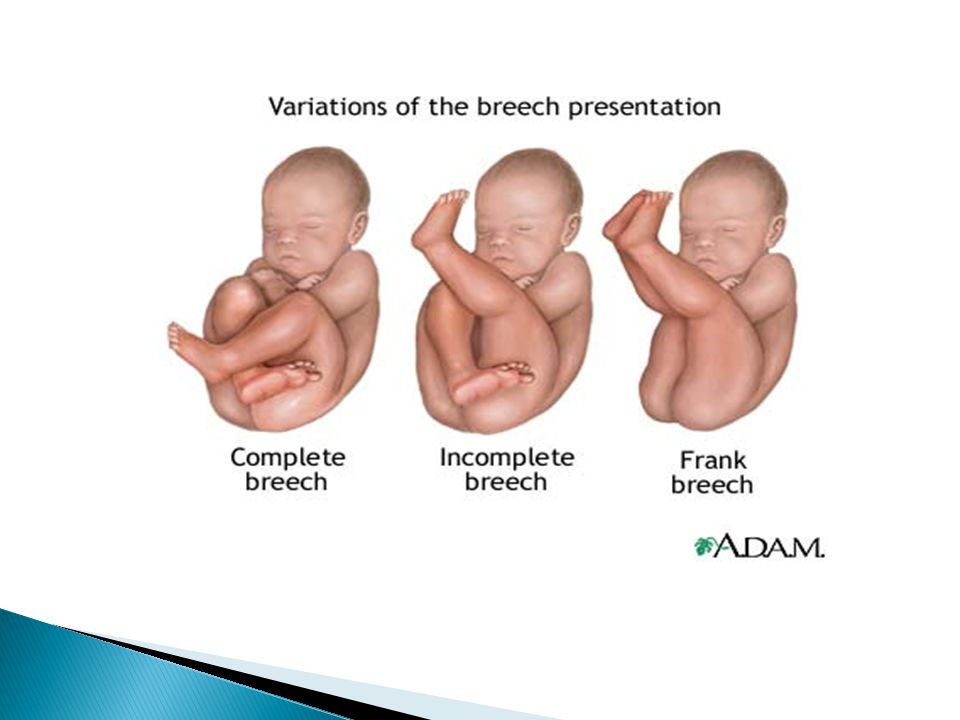
Labor Breech presentation occurs when the presenting part is the fetal buttocks or lower extremities. The incidence of breech presentation is 3% of all deliveries. Diagnosis is made by the Leopold’s exam, a cervical exam or an US. If US is unavailable an Xray will confirm breech presentation. Management of breech presentation is to offer an external cephalic version.

40
Labor The standard of care in many communities is to deliver breech presentations routinely by cesarean section. This avoids the complications of a vaginal breech delivery which includes an umbilical cord prolapse, birth asphyxia and birth trauma.

42
Labor Separation of the placenta usually occurs within 5-10 minutes after birth. The signs of placental separation are: a fresh show of blood, lengthening of the umbilical cord, an upward rise of the uterine fundus and the fundus becomes firm. Perineal lacerations are classified as follows: First degree – involving the mucosa or skin Second degree – extending into the submucosal tissues Third degree – involving the anal sphincter Fourth degree – involving the rectal mucosa

43
Labor Cesarean section is defined as delivery of the fetus through an incision in the abdominal and uterine walls. Currently the rate of C-sections in the US ranges from 10% of all deliveries to about 40% depending on the location. The most frequent indication for a C-section is dystocia. Other common indications are fetal distress, malpresentation, maternal indications, placental indications or a previous classical incision.

44
Obstetrical Analgesia and Anesthesia
Options for a patient in labor and for a vaginal birth include the following: “breathing” techniques, acupuncture, hypnosis, Tens unit, local anesthetic, intrathecal, epidural, paracervical block, pudendal nerve block and IV narcotics. Options for a C-section include: epidural, spinal or a general anesthetic.

45
Complications of Pregnancy
Complications of pregnancy include abortion, ectopic pregnancy, congenital malformations, multiple gestation, hypertension and diabetes. Complications of delivery include preterm and post term deliveries as well as fetal growth restriction and intrauterine fetal demise. Other complications include dystocia and obstetric hemorrhage.

46
Hospital Rotation You will meet twice with an attending physician using the birth model, Noelle, and reviewing the births that you have observed. You will be assigned to or will choose one of the hospitals to observe the births. Please introduce yourself to the resident on call, the RN and the attending physician. Goals and objectives will be set by the school.

Similar presentations