Download presentation
Presentation is loading. Please wait.

1
Question 18 Jo Dalgleish Eastern Health

2
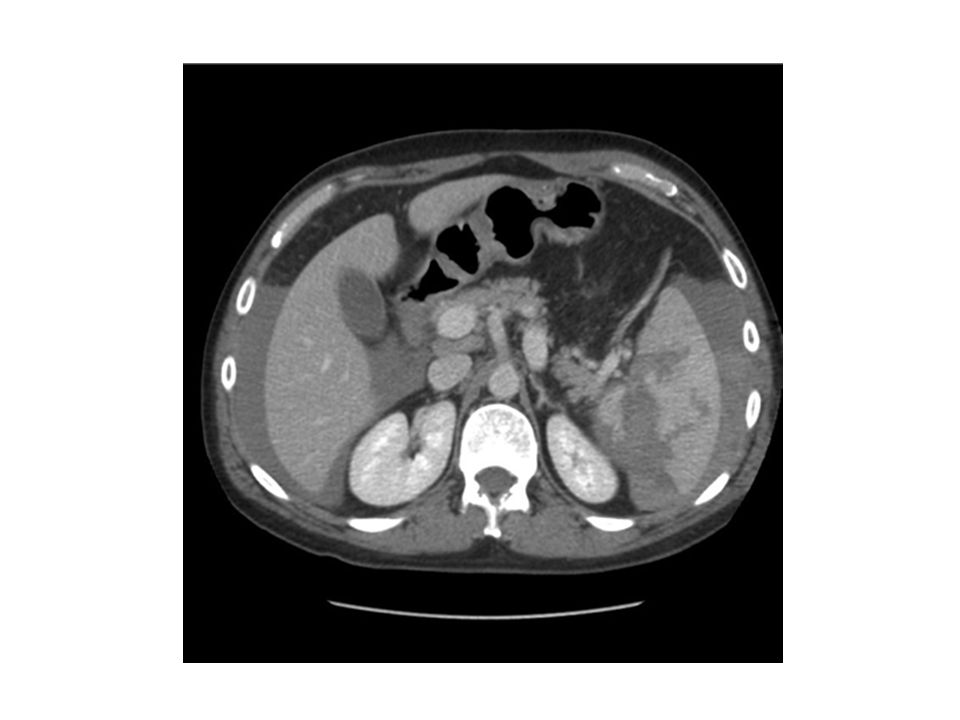
A 55 year old man is brought to the Emergency Department following a fall from a ladder. The patient was approximately 3 metres high and landed on concrete. On arrival he is awake and is complaining of severe abdominal pain. His observations are as follows: HR 110bpm BP 100/55mmHg RR 22/min O2 sats 100% on 6L O2 via Hudson mask GCS 15 (E4,V5,M6)
.")
4
1.What is the diagnosis (Provide 3 features on the CT to support your diagnosis) 1.The major Management options are conservative vs operative management. Describe 3 pros & 3 cons of each approach 2.Your registrar asks you about the correct ratios for massive transfusion. Describe your current ratio for massive transfusion and name one recent study to support your decision.

5
What is the diagnosis (Provide 3 features on the CT to support your diagnosis) Splenic Injury/laceration/fracture (ideally with grade) – Use the CT injury grade for the supporting features – Be mindful that image is single slice and make sure the level of the scan fits anatomically eg where is the splenic hilum relative to the level of the kidneys – When describing free fluid in setting of trauma can conclude “likely blood “ – Note that on the CT the fluid around the liver has a definite level c/w free fluid not subcapsular haematoma. AAST Grade for Splenic Injury grade III – Subcapsular haematoma >50% of surface area or expanding – intraparenchymal haematoma >5 cm or expanding – laceration >3 cm depth or involving trabecular vessels – ruptured subcapsular or parenchymal haematoma grade IV – laceration involving segmental or hilar vessels with major devascularisation (>25% of spleen)
.")
6
The major Management options are conservative vs operative management. Describe 3 pros & 3 cons of each approach This is the section that most people struggled with & I think its because you are being too literal with Pro & Con For a question like this you need to list the reasons or the advantages and disadvantages of each approach taking into account the injury/pt vitals/your knowledge of splenic injury. Unfortunately none of the answers below take into account this pt/ the vital signs/ the CT image/ or an understanding of splenic injury. Conservative – Pro Not invasive ( seriously!!) No anaesthetic risk No surgical complications Cheaper Less resource intensive – Con Not definitive High failure rate Needs lots of transfusions Operative – Pro Definitive Mx (of what/for what) Treats other injuries (like what) successful – Con Invasive Anaesthetic risk Scar/ pain
 No anaesthetic risk No surgical complications Cheaper Less resource intensive – Con Not definitive High failure rate Needs lots of transfusions Operative – Pro Definitive Mx (of what/for what) Treats other injuries (like what) successful – Con Invasive Anaesthetic risk Scar/ pain.")
7
The major Management options are conservative vs operative management. Describe 3 pros & 3 cons of each approach NB all of this is NOT required to pass but to demonstrate the points that could be made The standard criteria for NOM are hemodynamic stability/ readily stabilizable; lack of rebound and guarding; blood transfusions ≤ 4 units GCS 15 age < 55 years no associated intra- or retroperitoneal injuries (on abdominal CT scan) that would require surgical intervention Nonoperative management (NOM) of blunt injury to the spleen in adults has become the standard of care in hemodynamically stable patients The risk of overwhelming postsplenectomy infection (OPSI) prompted the evolution toward preservation of the injured spleen. Angiography should be considered for patients with American Association for the Surgery of Trauma (AAST) grade of greater than III injuries, presence of a contrast blush, moderate hemoperitoneum, or evidence of ongoing splenic bleeding. Nonoperative management of splenic injuries should only be considered in an environment that provides capabilities for monitoring, serial clinical evaluations, and 24 hr access to surgeon/OR for urgent laparotomy. The main complications are bleeding and delayed hematoma rupture. Operative Mx Patients who have diffuse peritonitis or who are hemodynamically unstable after blunt abdominal trauma should be taken urgently for laparotomy associated intra- or retroperitoneal injuries (on abdominal CT scan) that require surgical intervention laparotomy or angiography with embolization in patients who have significant ongoing transfusion requirements and/or declining Hct. Complex/severe splenic injuries, age, pre-existent splenic diseases, number of units of transfused blood, brain injuries are no longer considered absolute contraindications for NOM To avoid permanently increasing the patient's susceptibility to bacterial infections (caused by splenectomy), manage splenic injuries nonoperatively when possible. A routine laparotomy is not indicated in the hemodynamically stable patient without peritonitis presenting with an isolated splenic injury
 that would require surgical intervention Nonoperative management (NOM) of blunt injury to the spleen in adults has become the standard of care in hemodynamically stable patients The risk of overwhelming postsplenectomy infection (OPSI) prompted the evolution toward preservation of the injured spleen. Angiography should be considered for patients with American Association for the Surgery of Trauma (AAST) grade of greater than III injuries, presence of a contrast blush, moderate hemoperitoneum, or evidence of ongoing splenic bleeding. Nonoperative management of splenic injuries should only be considered in an environment that provides capabilities for monitoring, serial clinical evaluations, and 24 hr access to surgeon/OR for urgent laparotomy. The main complications are bleeding and delayed hematoma rupture. Operative Mx Patients who have diffuse peritonitis or who are hemodynamically unstable after blunt abdominal trauma should be taken urgently for laparotomy associated intra- or retroperitoneal injuries (on abdominal CT scan) that require surgical intervention laparotomy or angiography with embolization in patients who have significant ongoing transfusion requirements and/or declining Hct. Complex/severe splenic injuries, age, pre-existent splenic diseases, number of units of transfused blood, brain injuries are no longer considered absolute contraindications for NOM To avoid permanently increasing the patient s susceptibility to bacterial infections (caused by splenectomy), manage splenic injuries nonoperatively when possible. A routine laparotomy is not indicated in the hemodynamically stable patient without peritonitis presenting with an isolated splenic injury.")
8
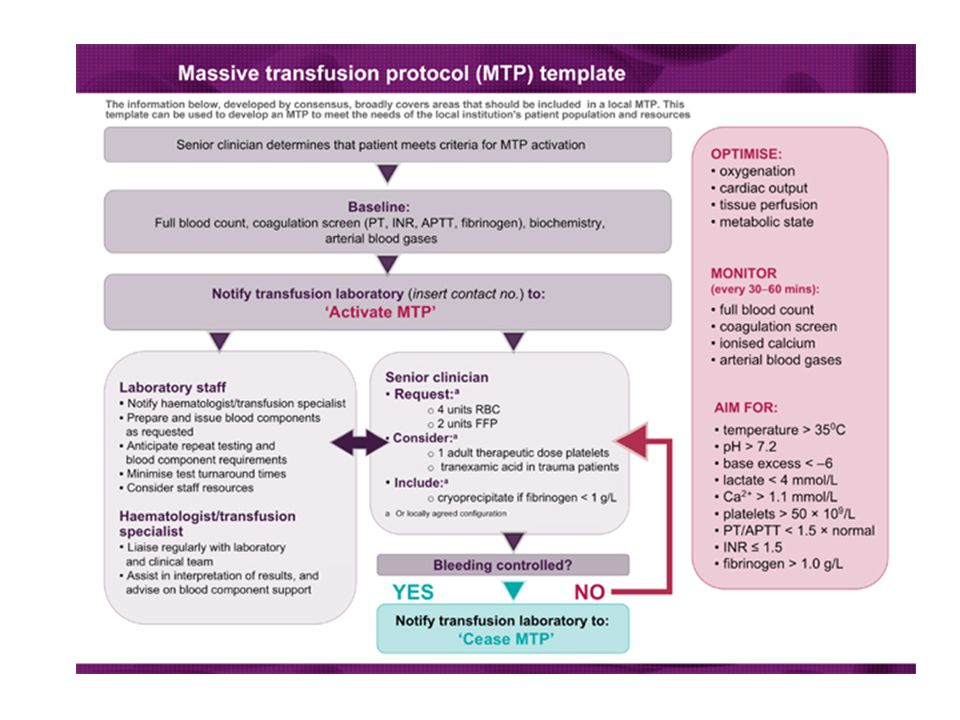
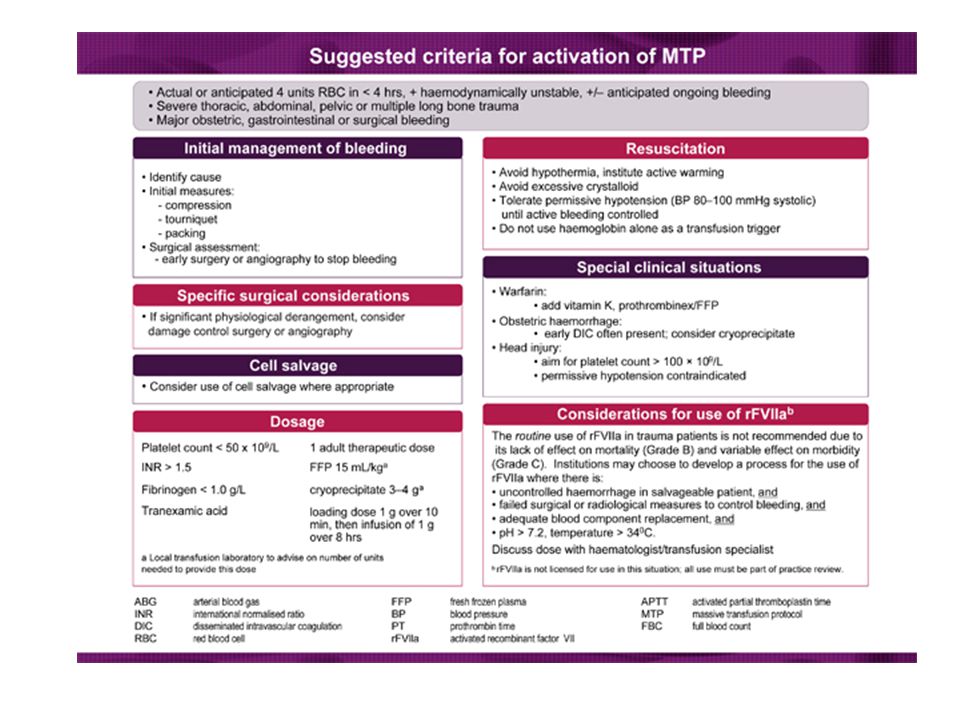
Your registrar asks you about the correct ratios for massive transfusion. Describe your current ratio for massive transfusion and name one recent study to support your decision. Needed to write ratio – 1:1:1 or 4:2:1 or similar Including the products – Rbc:FFP:Plts – Also adding (but not essential to pass) role of cryoprecip if fibrinogen < 1g/L Tranexamic Acid Name a study ( ideally from Mainstream/recognized journal) – PROPPR or PROMMTT – CRASH2 ( Tran.Ac) – Don’t put in any study in the hope the examiner won’t know or check.
 role of cryoprecip if fibrinogen < 1g/L Tranexamic Acid Name a study ( ideally from Mainstream/recognized journal) – PROPPR or PROMMTT – CRASH2 ( Tran.Ac) – Don’t put in any study in the hope the examiner won’t know or check..")
Similar presentations












. Straight to theatre? Time to laparotomy Trauma centre127 mins NCEPOD200 mins –NO CT110 mins –CT499 mins NO CT group unstable.>")





:>")
