Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2014 年 12 月 4 日 8:30-8:55 8階 医局 Ikeda Y, Shimada K, Teramoto T, Uchiyama S, Yamazaki T, Oikawa S, Sugawara M, Ando K, Murata M, Yokoyama K, Ishizuka N. Low-Dose Aspirin for Primary Prevention of Cardiovascular Events in Japanese Patients 60 Years or Older With Atherosclerotic Risk Factors: A Randomized Clinical Trial. JPPP JAMA. 2014 Nov 17. doi: 10.1001/jama.2014.15690. Jutkowitz E, Choi HK, Pizzi LT, Kuntz KM. Cost-effectiveness of allopurinol and febuxostat for the management of gout. Ann Intern Med. 2014 Nov 4;161(9):617-26. doi: 10.7326/M14-0227.
: doi: /M")
2
The Japanese Primary Prevention of Atherosclerosis With Aspirin for Diabetes (JPAD) trial JAMA. 2008;300(18):2134-2141
:")
3
Results ・ total 154 events occurred ・ primary end point; there is no significant difference ・ secondary - ; fatal coronary and cerebrovascular events > significantly (P=.0037)
")
4
2012 動脈硬化疾患予防ガイドライン

5
563)De Berardis G Sacco M,Strippoli GFM, etal: Aspirin fbr primary prevention of cardiovascular events in people with diabetes: meta, analysis of randomised controled trials BMJ 、 339:b4531,2009 564)Lonn E,Dagenais G Yusuf S, etal: Effects of vitamin E on cardiovascular and microvascular outcomes in high-risk patients with diabetes ・ Results of the HOPE study and MICRO-HOPE study ・ Diabetes Care'25:1919.1927.2002
De Berardis G Sacco M,Strippoli GFM, etal: Aspirin fbr primary prevention of cardiovascular events in people with diabetes: meta, analysis of randomised controled trials BMJ 、 339:b4531, )Lonn E,Dagenais G Yusuf S, etal: Effects of vitamin E on cardiovascular and microvascular outcomes in high-risk patients with diabetes ・ Results of the HOPE study and MICRO-HOPE study ・ Diabetes Care 25:")
6
3. Antiplatelet Agents Recommendations Consider aspirin therapy (75–162 mg/day) as a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk >10%). This includes most men aged >50 years or women aged >60 years who have at least one additional major risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria). C Aspirin should not be recommended for CVD prevention for adults with diabetes at low CVD risk (10-year CVD risk <5%, such as in men aged <50 years and women aged <60 years with no major additional CVD risk factors), since the potential adverse effects from bleeding likely offset the potential benefits. C In patients in these age-groups with multiple other risk factors (e.g., 10- year risk 5–10%), clinical judgment is required. E Use aspirin therapy (75–162 mg/day) as a secondary prevention strategy in those with diabetes with a history of CVD. A For patients with CVD and documented aspirin allergy, clopidogrel (75 mg/day) should be used. B Dual antiplatelet therapy is reasonable for up to a year after an acute coronary syndrome. B Diabetes Care. 2013 Jan;36(suppl 1):s1-s99.
 as a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk >10%). This includes most men aged >50 years or women aged >60 years who have at least one additional major risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria). C Aspirin should not be recommended for CVD prevention for adults with diabetes at low CVD risk (10-year CVD risk <5%, such as in men aged <50 years and women aged <60 years with no major additional CVD risk factors), since the potential adverse effects from bleeding likely offset the potential benefits. C In patients in these age-groups with multiple other risk factors (e.g., 10- year risk 5–10%), clinical judgment is required. E Use aspirin therapy (75–162 mg/day) as a secondary prevention strategy in those with diabetes with a history of CVD. A For patients with CVD and documented aspirin allergy, clopidogrel (75 mg/day) should be used. B Dual antiplatelet therapy is reasonable for up to a year after an acute coronary syndrome. B Diabetes Care Jan;36(suppl 1):s1-s99..")
7
Treatment (CVD) In patients with known CVD, consider ACE inhibitor therapy C and use aspirin and statin therapy A (if not contraindicated) to reduce the risk of cardiovascular events. In patients with a prior MI, β-blockers should be continued for at least 2 years after the event. B In patients with symptomatic heart failure, avoid thiazolidinedione treatment. C In patients with stable CHF, metformin may be used if renal function is normal but should be avoided in unstable or hospitalized patients with CHF. B Diabetes Care. 2013 Jan;36(suppl 1):s1-s99.
:s1-s99..")
8
Treatment (Retinopathy) Promptly refer patients with any level of macular edema, severe NPDR, or any PDR to an ophthalmologist who is knowledgeable and experienced in the management and treatment of diabetic retinopathy. A Laser photocoagulation therapy is indicated to reduce the risk of vision loss in patients with high-risk PDR, clinically significant macular edema, and in some cases severe NPDR. A Anti-vascular endothelial growth factor (VEGF) therapy is indicated for diabetic macular edema. A The presence of retinopathy is not a contraindication to aspirin therapy for cardioprotection, as this therapy does not increase the risk of retinal hemorrhage. A Diabetes Care. 2013 Jan;36(suppl 1):s1-s99.
 therapy is indicated for diabetic macular edema. A The presence of retinopathy is not a contraindication to aspirin therapy for cardioprotection, as this therapy does not increase the risk of retinal hemorrhage. A Diabetes Care Jan;36(suppl 1):s1-s99..")
9
C. Older Adults Recommendations Older adults who are functional, cognitively intact, and have significant life expectancy should receive diabetes care with goals similar to those developed for younger adults. E Glycemic goals for some older adults might reasonably be relaxed, using individual criteria, but hyperglycemia leading to symptoms or risk of acute hyperglycemic complications should be avoided in all patients. E Other cardiovascular risk factors should be treated in older adults with consideration of the time frame of benefit and the individual patient. Treatment of hypertension is indicated in virtually all older adults, and lipid and aspirin therapy may benefit those with life expectancy at least equal to the time frame of primary or secondary prevention trials. E Screening for diabetes complications should be individualized in older adults, but particular attention should be paid to complications that would lead to functional impairment. E Diabetes Care. 2013 Jan;36(suppl 1):s1-s99.
:s1-s99..")
10
1 Graduate School of Advanced Science and Engineering, Waseda University, Tokyo, Japan 2 Department of Cardiology, Shin-Oyama City Hospital, Tochigi, Japan 3 Teikyo Academic Research Center, Teikyo University, Tokyo, Japan 4 Clinical Research Center for Medicine, International University of Health and Welfare, Tokyo, Japan 5 Clinical Research Support Center, Center for Epidemiology and Preventive Medicine, The University of Tokyo Hospital, Japan 6 Diabetes and Lifestyle Disease Center, Fukujuji Hospital, Tokyo, Japan 7 Department of Internal Medicine, Sugawara Medical Clinic, Tokyo, Japan 8 Department of Internal Medicine, Kitamura Memorial Clinic, Tokyo, Japan 9 Department of Laboratory Medicine, Keio University School of Medicine, Tokyo, Japan 10 Department of Hematology, Tokai University Hachioji Hospital, Tokyo, Japan 11 Clinical Trial Department, Cancer Institute Hospital, Tokyo, Japan. the Japanese Primary Prevention Project (JPPP) JAMA. doi:10.1001/jama.2014.15690
 JAMA. doi: /jama")
11
Importance Prevention of atherosclerotic cardiovascular diseases is an important public health priority in Japan due to an aging population. Objective To determine whether daily, low-dose aspirin reduces the incidence of cardiovascular events in older Japanese patients with multiple atherosclerotic risk factors.

12
Design, Setting, and Participants The Japanese Primary Prevention Project (JPPP) was a multicenter, open-label, randomized, parallel-group trial. Patients (N = 14 464) were aged 60 to 85 years, presenting with hypertension, dyslipidemia, or diabetes mellitus recruited by primary care physicians at 1007 clinics in Japan between March 2005 and June 2007, and were followed up for up to 6.5 years, with last follow-up in May 2012. A multidisciplinary expert panel (blinded to treatment assignments) adjudicated study outcomes. Interventions Patients were randomized 1:1 to enteric-coated aspirin 100 mg/d or no aspirin in addition to ongoing medications. Main Outcomes and Measures Composite primary outcome was death from cardiovascular causes (myocardial infarction, stroke, and other cardiovascular causes), nonfatal stroke (ischemic or hemorrhagic, including undefined cerebrovascular events), and nonfatal myocardial infarction. Secondary outcomes included individual end points.
 were aged 60 to 85 years, presenting with hypertension, dyslipidemia, or diabetes mellitus recruited by primary care physicians at 1007 clinics in Japan between March 2005 and June 2007, and were followed up for up to 6.5 years, with last follow-up in May A multidisciplinary expert panel (blinded to treatment assignments) adjudicated study outcomes. Interventions Patients were randomized 1:1 to enteric-coated aspirin 100 mg/d or no aspirin in addition to ongoing medications. Main Outcomes and Measures Composite primary outcome was death from cardiovascular causes (myocardial infarction, stroke, and other cardiovascular causes), nonfatal stroke (ischemic or hemorrhagic, including undefined cerebrovascular events), and nonfatal myocardial infarction. Secondary outcomes included individual end points..")
14
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); CV, cardiovascular; DL, dyslipidemia; DM, diabetes mellitus; HbA1c, glycated hemoglobin; HT, hypertension. SI conversion factors: To convert total, LDL, and HDL cholesterol to mmol/L, multiply by 0.0259; triglycerides to mmol/L, multiply by 0.0113; glucose to mmol/L, multiply by 0.0555. a Calculated based on the Friedewald formula and direct measurements. b National Glycohemoglobin Standardization Program method. Table 1. Baseline Characteristics for Japanese Patients Receiving Aspirin or No Aspirin (Modified Intention-to-Treat Population)
.")
20
At present the choice of aspirin remains clear in several situations. Aspirin is indicated for patients at high short-term risk due to an acute vascular event and those undergoing certain vascular procedures; patients with any evidence of vascular disease should be given daily aspirin. On the other hand, patients at very low risk of vascular events should not take aspirin for prevention of vascular events, even at low dose. The ASCEND study involves aspirin for patients 40 years and older with type 1 or 2 diabetes 7,8 ; the ARRIVE study is testing aspirin in middle-aged and older patients who are at higher risk based on the presence of multiple CVD risk factors 9 ; and the ASPREE study is testing aspirin in individuals older than 70 years. 10 Information from these studies will help refine guidelines that currently reserve aspirin for higher-risk patients. 78 9 10 JAMA. Published online November 17, 2014. doi:10.1001/jama.2014.16047

21
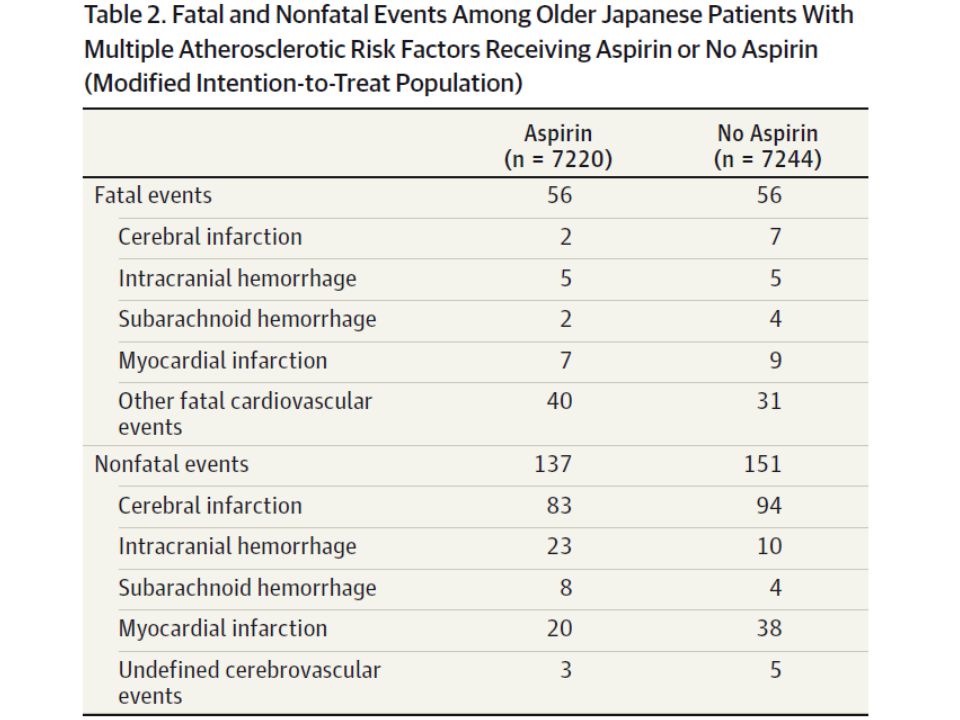
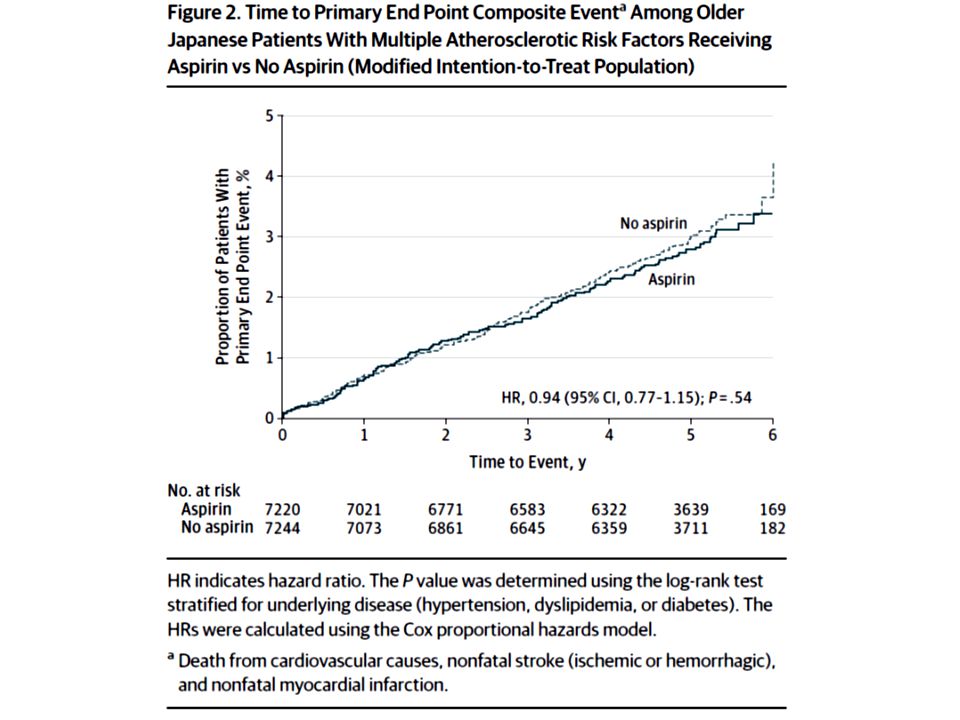
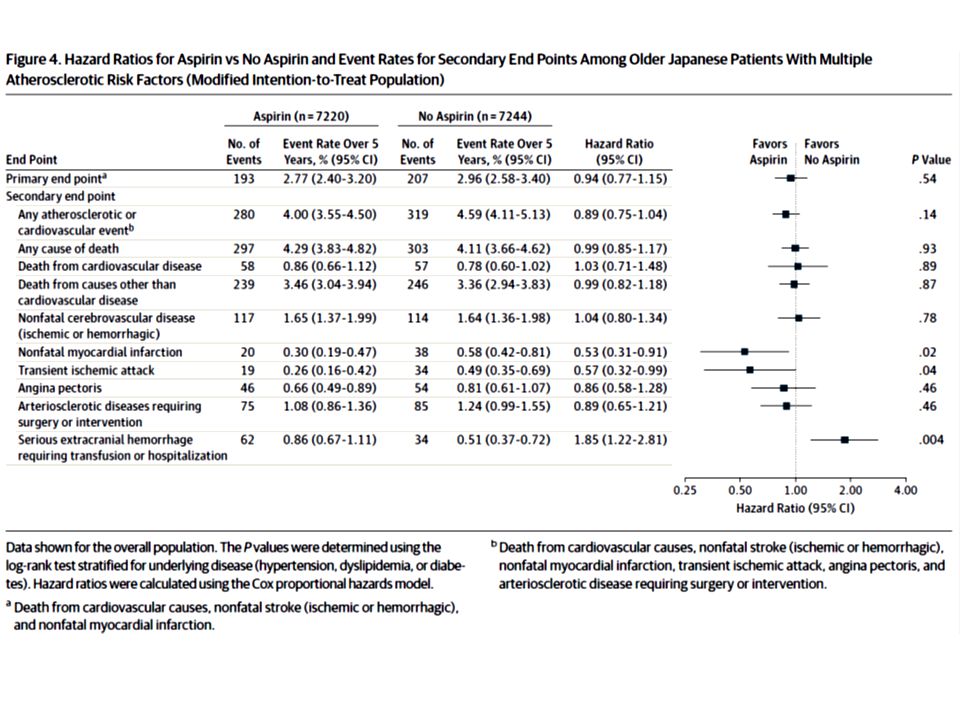
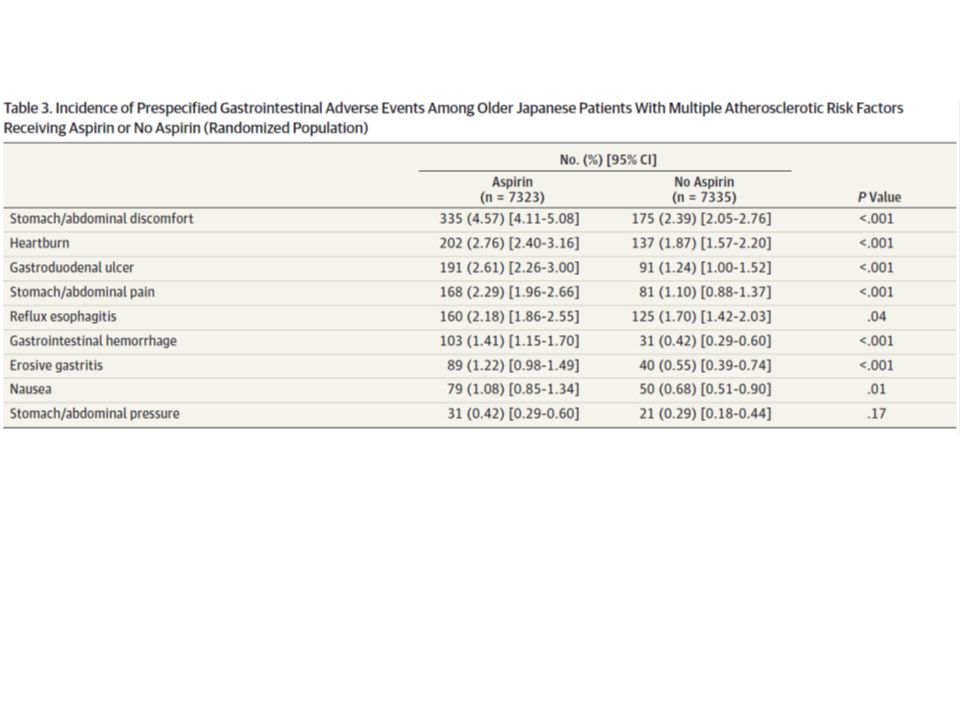
Results The study was terminated early by the data monitoring committee after a median follow-up of 5.02 years (interquartile range, 4.55–5.33) based on likely futility. In both the aspirin and no aspirin groups, 56 fatal events occurred. Patients with an occurrence of nonfatal stroke totaled 114 in the aspirin group and 108 in the no aspirin group; of nonfatal myocardial infarction, 20 in the aspirin group and 38 in the no aspirin group; of undefined cerebrovascular events, 3 in the aspirin group and 5 in the no aspirin group. The 5-year cumulative primary outcome event rate was not significantly different between the groups (2.77% [95% CI, 2.40%-3.20%] for aspirin vs 2.96% [95% CI, 2.58%-3.40%] for no aspirin; hazard ratio [HR], 0.94 [95% CI, 0.77- 1.15]; P =.54). Aspirin significantly reduced incidence of nonfatal myocardial infarction (0.30 [95% CI, 0.19-0.47] for aspirin vs 0.58 [95% CI, 0.42-0.81] for no aspirin; HR, 0.53 [95% CI, 0.31-0.91]; P =.02) and transient ischemic attack (0.26 [95% CI, 0.16-0.42] for aspirin vs 0.49 [95% CI, 0.35-0.69] for no aspirin; HR, 0.57 [95% CI, 0.32-0.99]; P =.04), and significantly increased the risk of extracranial hemorrhage requiring transfusion or hospitalization (0.86 [95% CI, 0.67-1.11] for aspirin vs 0.51 [95% CI, 0.37-0.72] for no aspirin; HR, 1.85 [95% CI, 1.22-2.81]; P =.004).
. Aspirin significantly reduced incidence of nonfatal myocardial infarction (0.30 [95% CI, ] for aspirin vs 0.58 [95% CI, ] for no aspirin; HR, 0.53 [95% CI, ]; P =.02) and transient ischemic attack (0.26 [95% CI, ] for aspirin vs 0.49 [95% CI, ] for no aspirin; HR, 0.57 [95% CI, ]; P =.04), and significantly increased the risk of extracranial hemorrhage requiring transfusion or hospitalization (0.86 [95% CI, ] for aspirin vs 0.51 [95% CI, ] for no aspirin; HR, 1.85 [95% CI, ]; P =.004)..")
22
Conclusions and Relevance Once-daily, low- dose aspirin did not significantly reduce the risk of the composite outcome of cardiovascular death, nonfatal stroke, and nonfatal myocardial infarction among Japanese patients 60 years or older with atherosclerotic risk factors. Trial Registration clinicaltrials.gov Identifier: NCT00225849.

23
Message アテローム性動脈硬化症リスク因子を有する高齢 日本人患者 ( 約 1/3 が糖尿病 )1 万 4464 人を対象 に、低用量アスピリン 1 日 1 回投与の心血管イベ ント予防効果を無作為化臨床試験で検証( JPPP 試験)。複合主要評価項目(心血管死、非致死性 脳卒中 / 心筋梗塞) 5 年累積発生率に有意差は見 られなかった(ハザード比 0.94 )。本試験は無 益性のため中止された。 リスク因子によるのかもしれないが。...
1 万 4464 人を対象 に、低用量アスピリン 1 日 1 回投与の心血管イベ ント予防効果を無作為化臨床試験で検証( JPPP 試験)。複合主要評価項目(心血管死、非致死性 脳卒中 / 心筋梗塞) 5 年累積発生率に有意差は見 られなかった(ハザード比 0.94 )。本試験は無 益性のため中止された。 リスク因子によるのかもしれないが。...")
25
製品名アロプリノール錠 100mg 「ケミファ」 成分名アロプリノール 薬価 7.70 円 先発医薬品名/会社ザイロリック錠 100 /グラクソ・スミスク ライン 薬価基準収載医薬品コード 3943001F1012 レセプト電算処理コード 620856215 商品名 単位 薬価 フェブリク錠 10mg 錠 31.10 円 フェブリク錠 20mg 錠 56.40 円 フェブリク錠 40mg 錠 106.60 円 Prices for 30 tablets of allopurinol 300mg (generic) $4.00 0.04 per 100mg Febuxostat 80 mg Prices — Generic Version $0.6-2.0 0.3-1.0 per 40mg
 $ per 100mg Febuxostat 80 mg Prices — Generic Version $ per 40mg")
26
Ann Intern Med. 2014;161:617-626. doi:10.7326/M14-0227 Mr. Jutkowitz and Dr. Kuntz: Division of Health Policy and Management, School of Public Health, University of Minnesota, MMC 729, 420 Delaware Street SE, Minneapolis, MN 55455. Dr. Choi: Division of Rheumatology, Allergy, and Immunology, Massachusetts General Hospital, Harvard Medical School, 55 Fruit Street, Bulfinch 165, Boston, MA 02114. Dr. Pizzi: Thomas Jefferson University, Jefferson School of Pharmacy, 901 Walnut Street, Health Professions Academic Building, Philadelphia, PA 19017.

27
Background: Gout is the most common inflammatory arthritis in the United States. Objective: To evaluate the cost- effectiveness of urate-lowering treatment strategies for the management of gout.

28
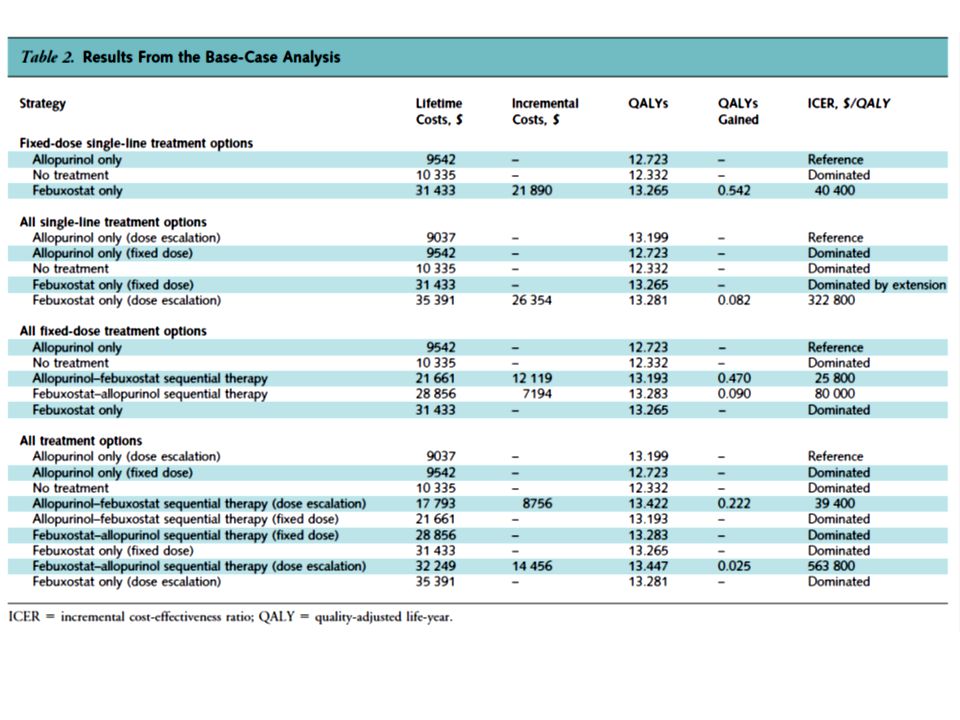
Design: Markov model. Data Sources: Published literature and expert opinion. Target Population: Patients for whom allopurinol or febuxostat is a suitable initial urate-lowering treatment. Time Horizon: Lifetime. Perspective: Health care payer. Intervention: 5 urate-lowering treatment strategies were evaluated: no treatment; allopurinol- or febuxostat-only therapy; allopurinol–febuxostat sequential therapy; and febuxostat–allopurinol sequential therapy. Two dosing scenarios were investigated: fixed dose (80 mg of febuxostat daily, 0.80 success rate; 300 mg of allopurinol daily, 0.39 success rate) and dose escalation (≤120 mg of febuxostat daily, 0.82 success rate; ≤800 mg of allopurinol daily, 0.78 success rate). Outcome Measures: Discounted costs, discounted quality- adjusted life-years, and incremental cost-effectiveness ratios.
 and dose escalation (≤120 mg of febuxostat daily, 0.82 success rate; ≤800 mg of allopurinol daily, 0.78 success rate). Outcome Measures: Discounted costs, discounted quality- adjusted life-years, and incremental cost-effectiveness ratios..")
30
Table 1. Model Inputs* SUA serum uric acid. * When probabilities in studies were not reported on a monthly basis, the authors adjusted using rates and then transformed rates into monthly probabilities. All cost estimates are reported in 2013 U.S. dollars. † The upper range for the effectiveness of febuxostat was based on 10% of the mean value. ‡ Probability was assumed to persist for the first year of receiving allopurinol. § Probability is conditional on experiencing the syndrome. Probability of switching is only for scenarios that model a switch strategy. The probability of switching due to being in an uncontrolled state is conditional on patients remaining in the uncontrolled-on-therapy state for 3 mo. If patients remain in the uncontrolled-on-therapy state for 9 mo and have not already switched, then they immediately change therapies. ¶ Probability of switching is only for scenarios that model a switch strategy. Switching due to an adverse event is conditional on patients experiencing an adverse event within 3 mo of starting therapy. Patients can switch therapy because of an adverse event, regardless of being in a controlled or an uncontrolled state. ** Discontinuation due to therapeutic failure is defined as the probability of discontinuing treatment conditional on staying in an uncontrolled state for a given period. †† Discontinuation due to adverse event is conditional on experiencing an adverse event and is assumed to persist for the first 3 mo of treatment. ‡‡ Utility associated with having the hypersensitivity syndrome is 0.35 regardless of the state in which a person resides. §§ The low estimate in the price range is 50% of the mean value. The high estimate is the upper 95% CI derived from the probabilistic sensitivity analysis. The low estimate in the price range is derived from single technology appraisal submission to the U.K. National Institute for Health and Care Excellence. The high estimate in the range is 50% of the mean estimate.

34
The acceptability curve shows the urate- lowering therapy strategy with the highest probability of being cost-effective for a given willingness- topay threshold. When willingness-to-pay per QALY is less than $40 100, dose escalation of allopurinol alone is the optimal treatment. QALY = quality- adjusted life-year.

35
Results of Base-Case Analysis: In both dosing scenarios, allopurinol-only therapy was cost-saving. Dose-escalation allopurinol–febuxostat sequential therapy was more costly but more effective than dose-escalation allopurinol therapy, with an incremental cost-effectiveness ratio of $39 400 per quality-adjusted life-year. Results of Sensitivity Analysis: The relative rankings of treatments did not change. Our results were relatively sensitive to several potential variations of model assumptions; however, the cost-effectiveness ratios of dose escalation with allopurinol–febuxostat sequential therapy remained lower than the willingness-to-pay threshold of $109 000 per quality- adjusted life-year.

36
Limitation: Long-term outcome data for patients with gout, including medication adherence, are limited. Conclusion: Allopurinol single therapy is cost- saving compared with no treatment. Dose- escalation allopurinol–febuxostat sequential therapy is cost-effective compared with accepted willingness-to-pay thresholds. Primary Funding Source:Agency for Healthcare Research and Quality.

37
Message 既発表論文や専門家の意見から、痛風管理での尿 酸降下治療戦略の費用対効果をマルコフモデルで 検証。用量増加シナリオにおいて、費用削減効果 が高かったアロプリノール単独療法に比べアロプ リノール - フェブキソスタット継続療法で費用は 増加するが効果が高く、質調整生存年当たりの増 分費用対効果比( ICER )は 3 万 9400 ドルと推算 された。
は 3 万 9400 ドルと推算 された。")
Similar presentations









>")



 The LIPID Study Group N Engl J Med 1998;339:1349-57.>")












>")