Download presentation
Presentation is loading. Please wait.

1
Polyarthralgia Tanya Potter Consultant Rheumatologist UHCW

2
Aims Differential diagnosis of polyarthralgia/polyarthritis Differential diagnosis of polyarthralgia/polyarthritis Investigation of joint pains Investigation of joint pains

3
What is polyarthralgia? What is polyarthralgia? What conditions present with polyarthralgia? What conditions present with polyarthralgia?

4
Inflammatory Inflammatory Mechanical Mechanical Pain syndromes Pain syndromes

5
How do you differentiate between mechanical and inflammatory symptoms?

6
Mechanical vs Inflammatory Inflammatory Mechanical Inflammatory Mechanical Immobility stiffness latter day Immobility stiffness latter day EMS>30-60 minsEMS 30-60 minsEMS<30-60 mins Better with activity and NSAIDsworse with activity Better with activity and NSAIDsworse with activity Joint swelling, erythema,heat instability Joint swelling, erythema,heat instability Systemic symptoms locking Systemic symptoms locking Multi-organ involvement trauma, strain overusage Multi-organ involvement trauma, strain overusage

7
Age and sex Incidence AGEFEMALEMALE Young adults Middle age Old age

8
Age and sex Incidence AGEFEMALEMALE Young adults RA Reactive arthritis SLE(Sero-ve) Middle age Old age
 Middle age Old age")
9
Age and sex Incidence AGEFEMALEMALE Young adults RA Reactive arthritis SLE(Sero-ve) Psoriatic arthritis (Sero-ve) Middle age RA Old age
 Psoriatic arthritis (Sero-ve) Middle age RA Old age")
10
Age and sex Incidence AGEFEMALEMALE Young adults RA Reactive arthritis SLE(Sero-ve) Psoriatic arthritis (Sero-ve) Middle age RA Old age OA Crystal arthritis
 Psoriatic arthritis (Sero-ve) Middle age RA Old age OA Crystal arthritis")
11
OA Clinical features Clinical features

12
Osteoarthritis Mechanical symptoms Mechanical symptoms Bony swelling, crepitus Bony swelling, crepitus DIP (Heberden), PIP (Bouchard), 1 st CMCJ, neck, lower back, hips, knees, 1 st MTP DIP (Heberden), PIP (Bouchard), 1 st CMCJ, neck, lower back, hips, knees, 1 st MTP
, PIP (Bouchard), 1 st CMCJ, neck, lower back, hips, knees, 1 st MTP DIP (Heberden), PIP (Bouchard), 1 st CMCJ, neck, lower back, hips, knees, 1 st MTP")
13
Pathophysiology?

14
Pathophysiology Imbalance between degradative and reparative connective tissue processes within joint leading to failure of joint Imbalance between degradative and reparative connective tissue processes within joint leading to failure of joint Occasional genetic association Occasional genetic association Pathological stresses may lead to micro trauma and inflammatory change Pathological stresses may lead to micro trauma and inflammatory change

15
Radiology - OA

16
Four cardinal features: Joint space narrowing Sclerosis Subchondral cysts Osteophytes

17
Other features associated with athralgia Prodromal events Prodromal events Associated conditions Associated conditions

18
CLUES Prodromal event eg GI/GU infection – reactive arthritis Prodromal event eg GI/GU infection – reactive arthritis Associated conditions eg psoriasis, colitis, iritis Associated conditions eg psoriasis, colitis, iritis

19
Pattern and Symmetry? Pattern and Symmetry?

20
CLUES Multi-organ disease Multi-organ disease Fibromyalgia symptoms Fibromyalgia symptoms

23
Rheumatoid Female ~ 1 in 100 Female ~ 1 in 100 symmetrical polyarthritis, targeting small joint and large symmetrical polyarthritis, targeting small joint and large DIP sparing DIP sparing

24
Pathophysiology Inflammatory condition Inflammatory condition Strong genetic component- HLA DR4 Strong genetic component- HLA DR4 Environmental effects Environmental effects Inflammation of synovium with high levels of chemokines and cytokines and resultant tissue damage Inflammation of synovium with high levels of chemokines and cytokines and resultant tissue damage o Systemic features?

26
Psoriatic arthritis Psoriasis 2-3% population Psoriasis 2-3% population 5-10% of these will develop Ps arthritis 5-10% of these will develop Ps arthritis Family history 55X more likely (40%) Family history 55X more likely (40%) Pathophysiology? Pathophysiology?

27
HLA B27 related arthritis HLA B27 related arthritis Arthritis and enthesitis possibly T cell driven, with tissue damage Arthritis and enthesitis possibly T cell driven, with tissue damage

28
Sero-ve Spondyloarthritis – psoriatic arthritis DIP, poly, dactylitis, DIP, poly, dactylitis, enthesitis, spinal enthesitis, spinal Younger age Younger age

30
Soft tissue swelling Soft tissue swelling Joint space narrowing Joint space narrowing Mouse ear erosions Mouse ear erosions Periostitis with new bone formation Periostitis with new bone formation DIP joint involvement DIP joint involvement

32
Polyarticular crystal arthropathy eg gout Chronic Chronic Tophi Tophi Erosions Erosions Older age Older age Nb pseudogout Nb pseudogout

34
polyarthalgia/polyarthritis ‘ o Multi-organ disease – CTD and vasculitis o Viral arthritis (eg parvovirus, rubella, hepatitis) o Medical conditions eg o diabetic cheiroarthropathy o Sarcoidosis-
 o Medical conditions eg o diabetic cheiroarthropathy o Sarcoidosis-")
35
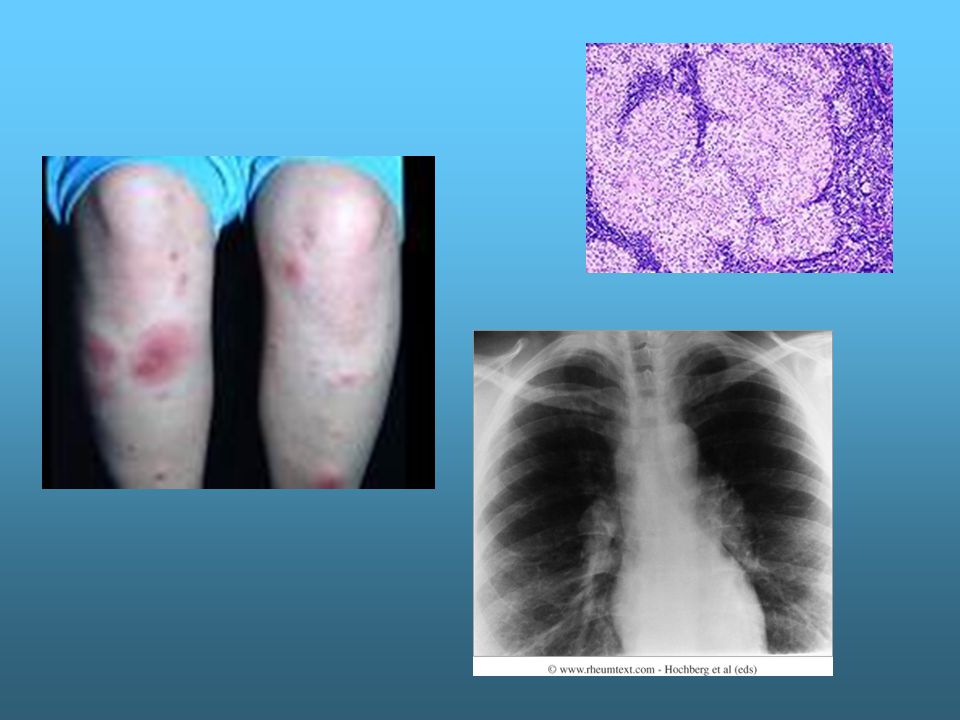
Sarcoid Acute or chronic Acute or chronic Multisystem disorder, non caseating granulomas Multisystem disorder, non caseating granulomas Acute: spring time (?viral) young adults sudden onset of lower limb arthritis and erythema nodosum & red eyes Acute: spring time (?viral) young adults sudden onset of lower limb arthritis and erythema nodosum & red eyes Fever and cough Fever and cough
 young adults sudden onset of lower limb arthritis and erythema nodosum & red eyes Acute: spring time ( viral) young adults sudden onset of lower limb arthritis and erythema nodosum & red eyes Fever and cough Fever and cough")
36
Ix Raised serum ACE Raised serum ACE Raised Ca Raised Ca ESR, CRP ESR, CRP Chest xray Chest xray

38
Outcome of acute: good, NSAIDs, oral prednisolone Outcome of acute: good, NSAIDs, oral prednisolone Chronic: afrocarribean Chronic: afrocarribean Grumbling lung disease, jt, muscle, liver disease Grumbling lung disease, jt, muscle, liver disease Treatment unclear- prednisolone, methotrexate Treatment unclear- prednisolone, methotrexate

39
What are CTD? Symptoms and signs?

40
Connective tissue disease Eg SLE, scleroderma, polymyositis, Sjogren’s Eg SLE, scleroderma, polymyositis, Sjogren’s Auto-immune Auto-immune Multi-organ Multi-organ Anti-nuclear antibodies Anti-nuclear antibodies

41
SLE Raynauds Raynauds Rashes Rashes Arthralgia Arthralgia Haem Haem CNS CNS Renal Renal Serositis Serositis thrombosis thrombosis

42
Sle- skin o Photosensitive rashes eg SLE o Discoid lupus

43
Sle- renal Significant cause of morbidity and mortality- condition and treatment Significant cause of morbidity and mortality- condition and treatment

44
Sjogrens syndrome o Destruction of exocrine glands o Dry eyes and mouth- caries o Liver, lungs, gut, arthralgia, MNM o Increased B cell lymphoma risk

45
Scleroderma o Localised (CREST) o Diffuse o Raynauds, finger ulcers o Sclerosis of most organs o GI, skin, ILD, renal crisis
 o Diffuse o Raynauds, finger ulcers o Sclerosis of most organs o GI, skin, ILD, renal crisis")
46
Myositis Inflammatory muscle condition Inflammatory muscle condition Demato or polymyosits Demato or polymyosits Proximal painless weakness Proximal painless weakness

47
What are the vasculitides and what type of symptoms and signs?

48
Vasculitis Small, medium, large vessel Small, medium, large vessel Eg MPA, Churg Strauss, PAN, Wegeners, GCA Eg MPA, Churg Strauss, PAN, Wegeners, GCA ANCA ANCA

49
Vasculitis- skin o Vasculitis – petechial, purpura, ulcer

50
Vasculitis Systemic, vasculitic ulcers/rashes, arthralgias/arthritis – non deforming Systemic, vasculitic ulcers/rashes, arthralgias/arthritis – non deforming Pulmonary – haemoptysis Pulmonary – haemoptysis

51
Vasculitis RENAL – URINE DIP + BP RENAL – URINE DIP + BP ENT –eg Wegener’s ENT –eg Wegener’s Neuropathy eg footdrop Neuropathy eg footdrop

52
PMR and GCA features?

53
Polymyalgia rheumatica and GCA Over 50’s Over 50’s Proximal inflammatory pain and stiffness Proximal inflammatory pain and stiffness GCA – large vessel arteritis GCA – large vessel arteritis Temporal headache, jaw claudication visual disturbance, systemic upset Temporal headache, jaw claudication visual disturbance, systemic upset Raised ESR and CRP – urgent steroids Raised ESR and CRP – urgent steroids TA biopsy TA biopsy

54
Fibromyalgia “All over pain” “All over pain” Fatigue Fatigue Sleep disturbance Sleep disturbance Depression Depression Anxiety Anxiety Irritable bowel Irritable bowel Tender spots Tender spots Diagnosis of exclusion Diagnosis of exclusion

55
Investigations Inflammatory arthritis – Inflammatory arthritis –

56
Investigations Inflammatory arthritis – RA Inflammatory arthritis – RA FBC, ESR, CRP, U+E, LFT, RF, anti-CCP, ANA, FBC, ESR, CRP, U+E, LFT, RF, anti-CCP, ANA, XR Hands and feet and chest XR Hands and feet and chest Viral – Parvovirus Viral – Parvovirus

57
Investigations ? CTD/vasculitis - ? CTD/vasculitis -

58
Investigations ? CTD/vasculitis - ANA, ANCA, complement ? CTD/vasculitis - ANA, ANCA, complement Urine dip and BP Urine dip and BP Organ based investigations Organ based investigations

59
Investigations Diffuse symptoms – CK, Ca, ALP, TFT Diffuse symptoms – CK, Ca, ALP, TFT Crystal – joint aspirate, radiology, urate, U+E Crystal – joint aspirate, radiology, urate, U+E

60
What is RF and what other conditions present with elevated RF?

61
Rheumatoid factor Autoantibody vs Fc portion of IgG – any isotype but typically IgM RF Acute infection eg infectious mononucleosis Chronic infection eg SBE, TB Inflammatory disease: CTD, Fibrosing alveolitis, Malignancy: Lymphoma, leukaemia 5% healthy population RF <15 usually not significant

62
Anti-CCP Anti-cyclic citrullinated peptide Anti-cyclic citrullinated peptide More specific for RA than RF More specific for RA than RF May predict erosive damage May predict erosive damage

63
What are the ANA and ENA?

64
ANA and ENA ANA 1/40 not significant unless associated with appropriate clinical scenario ANA 1/40 not significant unless associated with appropriate clinical scenario Also in RA, auto immune liver disease, neoplasia, healthy population… Also in RA, auto immune liver disease, neoplasia, healthy population…

65
ANA and ENA ENA – extractable nuclear antigens (ANA subtypes) ENA – extractable nuclear antigens (ANA subtypes) Anti-DNA - SLE Anti-DNA - SLE Anti-Ro and anti-La - Sjogrens Anti-Ro and anti-La - Sjogrens Scl 70 and anti-centromere – Scleroderma Scl 70 and anti-centromere – Scleroderma Anti-RNP – mixed CTD Anti-RNP – mixed CTD Anti-Jo1 - myositis Anti-Jo1 - myositis
 ENA – extractable nuclear antigens (ANA subtypes) Anti-DNA - SLE Anti-DNA - SLE Anti-Ro and anti-La - Sjogrens Anti-Ro and anti-La - Sjogrens Scl 70 and anti-centromere – Scleroderma Scl 70 and anti-centromere – Scleroderma Anti-RNP – mixed CTD Anti-RNP – mixed CTD Anti-Jo1 - myositis Anti-Jo1 - myositis")
66
What is ANCA ?

67
ANCA Antibodies vs specific antigens in cytoplasm of neutrophils Antibodies vs specific antigens in cytoplasm of neutrophils ANCA reactive to myeloperoxidase (MPO) – perinuclear pattern of staining P-ANCA eg microscopic polyarteritis ANCA reactive to myeloperoxidase (MPO) – perinuclear pattern of staining P-ANCA eg microscopic polyarteritis
 – perinuclear pattern of staining P-ANCA eg microscopic polyarteritis ANCA reactive to myeloperoxidase (MPO) – perinuclear pattern of staining P-ANCA eg microscopic polyarteritis")
68
ANCA ANCA reactive to proteinase 3 (PR3) – cytoplasmic pattern of staining C-ANCA eg Wegener’s granulomatosis ANCA reactive to proteinase 3 (PR3) – cytoplasmic pattern of staining C-ANCA eg Wegener’s granulomatosis
 – cytoplasmic pattern of staining C-ANCA eg Wegener’s granulomatosis ANCA reactive to proteinase 3 (PR3) – cytoplasmic pattern of staining C-ANCA eg Wegener’s granulomatosis")
69
Thank-you

Similar presentations






 25 th Nov 2013.>")
,FRCPLondon,FRCP Edin, FACP Rheum CONSULTANT RHEUMATOLOGIST Aut Even Hospital, Kilkenny Whitfield Clinic Waterford,The St.>")
 Etiology is.>")





 Dr. Raid Jastania. Vasculitis Inflammation of the walls of the vessels Causes of inflammation: –Infectious, physical, chemical,>")








 Aneurysms & Dissections Veins & Lymphatics Tumors.>")

