Download presentation
Presentation is loading. Please wait.

1
Osteoporosis

2
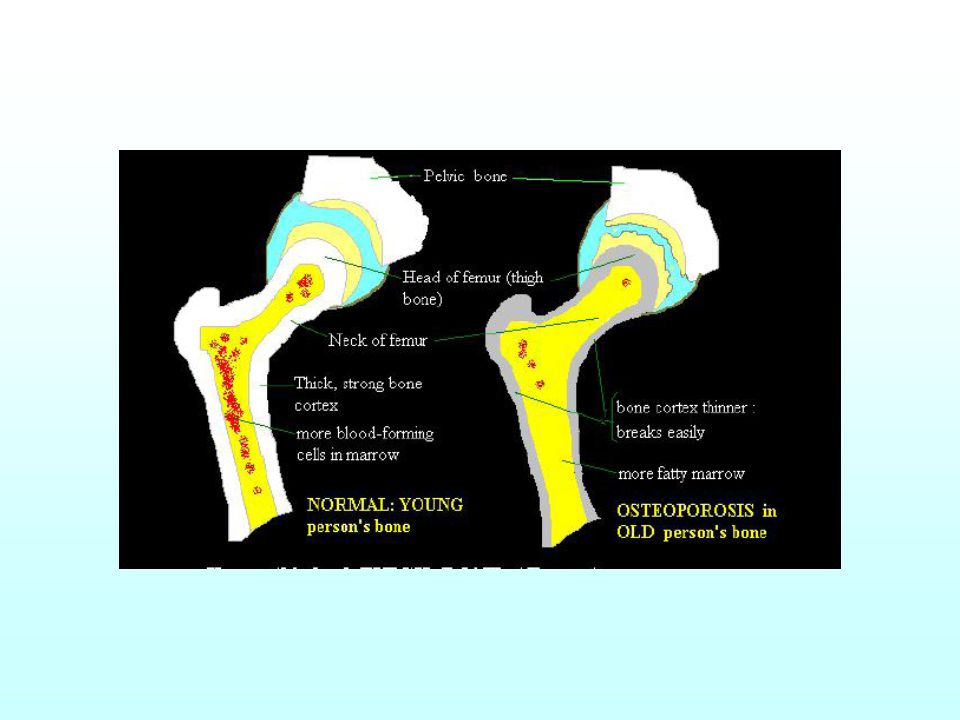
What is it? Systemic skeletal disease characterised by: –low bone mass –microarchitectural deterioration of bone tissue –resultant increase in fragility and risk of fracture

3
national osteoporosis society Why is it important? 1 in 3 women and 1 in 12 men over the age of 50 Every 3 minutes someone has a fracture due to osteoporosis ~2 million people in the Aus have osteoporosis 20,000 hip fractures/yr Aus 50,000 wrist fractures UK 120,000 spinal fractures UK Costs $7.4 billion each year

4
Bone Components Protein matrix of collagen fibres Bone mineral;an inorganic calcium compound hydroxyapatite

5
Osteoblasts; synthesise collagen and the control of mineralisation. Osteoclasts; resorb bone by pumping out H+ that dissolves the hydroxyapatite. Osteocytes; direct bone to form in the places where it is most needed. They may detect mechanical deformation and mediate the response of the osteoblasts

6
Idiopathic Osteoporosis Type 1 –postmenopausal women –accelerated loss of trabecular bone –# vertebral bodies, distal forearm –Oestrogen inhibits osteoclasts; postmenopause bone is resorbed faster

7
Idiopathic Osteoporosis Type 2 –women and men >70yrs –loss of trabecular and cortical bone –NOF, prox. Humerus, pelvis, prox tibia

8
Type 2... “ age related” increased breakdown by osteoclasts decreased bone formation by osteoblasts contribution of: –decreased oestrogen levels –Vitamin D deficiency –secondary Hyperparathyroidism Decreased activity ?decreased production of insulin-like growth factors

9
Secondary Osteoporosis Hyperparathyroidism Hyperthyroidism Hypogonadism Cushing’s Vit D –helps Ca+ absorbtion in the intestine. Low Vit D results in decreased plasma Ca+.. This increases PTH secretion -> More Ca+ is resorbed from bone Ca+ deficiency Malabsorption IMMOBILITY

10
Associated Mechanism not always understood –Rheumatoid Arthritis –COPD –ETOH dependance or >3 units/day –Myeloma –Chronic Liver Disease –Diabetes

11
Other Risk factors Female - lower peak bone mass, increased menopausal bone loss, longer life >60years FmHx (maternal) Caucasian or Asian Early menopause Prolonged Amenorrhoea at young age Low BMI (<19) History of fracture Smoker Sedentary
 Caucasian or Asian Early menopause Prolonged Amenorrhoea at young age Low BMI (<19) History of fracture Smoker Sedentary")
12
Medications Steroids –increased bone loss by suppressing osteoblasts –2.5% pop age>75 Phenytoin Heparin Chemotherapy - letrozole

14
Presentation Either with fracture or case finding otherwise asymptomatic

15
Kinds of Fracture “Low trauma fractures” “fragility fractures” WHO: # caused by injury insufficient to break normal bone - minimal standing height, or no trauma at all

17
Vertebral crush # Acute or Chronic Asymptomatic in 2/3rds Pain Kyphosis Instability Decreased Height

18
Hip Fracture 70% mortality at one-year if not fixed 30% one year mortality 40% severely disabled at one year

20
RED FLAG identification Investigations –FBC –ESR –LFTs –U&E –Ca/Phos/ALP –Immunoglobulins –Electrophoresis/BJP –TFTs

21
Diagnosis without fracture Don’t use XR for diagnosis unless reported as “severe osteopenia” (then get DXA scan) Ultrasound of calcaneus - not useful
 Ultrasound of calcaneus - not useful")
22
DEXA Scan Dual-energy X-Ray absorptiometry two beams of single energy pass through bone. The denser the bone the more the beams are attenuated. BMD is then compared to a reference range of young adults with average bone density, this is expressed in standard deviations: T scores : –0 and -1 SD - within normal range –-1 and -2.5 SD- osteopenia –below -2.5SD- osteoporosis (WHO definition) a Z score is also calculated. This compares BMD with a reference range of those the same age.
 a Z score is also calculated. This compares BMD with a reference range of those the same age..")
23
only do DXA scan as a “casefinding strategy, rather than for population screening” it predicts future fracture with high specificity, but low sensitivity

24
Treatment -Drugs Calcium and vitamin D Bisphosphonates. Strontium Hormone replacement therapy (HRT) Selective Estrogen Receptor Modulators (SERMs) Testosterone recombinant Parathyroid Hormone
 Selective Estrogen Receptor Modulators (SERMs) Testosterone recombinant Parathyroid Hormone.")
25
Bisphosphonates. Block mineralisation and osteoclastic bone resorption 2nd and 3rd generation have more anti-resorptive properties cyclic Etidronate (1st gen) - needs to be cyclical to stop osteomalacia developing, (2/52 etidronate, 10/52 calcium)
 - needs to be cyclical to stop osteomalacia developing, (2/52 etidronate, 10/52 calcium).")
26
Side Effects not in renal failure! Jaw osteonecrosis Upper GI side effects must be taken upright and stay sitting or standing without food or drink for 30+ mins

27
Bisphosphonates... Alendronate (2nd gen) - can cause oesophageal ulceration. Most data is from daily dosing, but current recommendations are for weekly Risedronate. (3rd gen) - cylic side chain Ibandronate (not yet available here) - iv preparation or once monthy oral tablet. Evidence not direct Zolendronic Acid - once yearly infusion. NO evidence for osteoporosis - high risk of Osteonecrosis Reduce vertebral and non-vertebral, including hip
 - cylic side chain Ibandronate (not yet available here) - iv preparation or once monthy oral tablet. Evidence not direct Zolendronic Acid - once yearly infusion. NO evidence for osteoporosis - high risk of Osteonecrosis Reduce vertebral and non-vertebral, including hip.")
28
Strontium Sachet drink - daily side effects - diarrhoea and headache Reduce vertebral and non-vertebral, including hip

29
Other treatment SERMs –(selective oestrogen receptor modulators) – Raloxifene –decreases risk of ER+ve breast cancer – Increases risk of DVT/PE – Used mainly if intolerant of bisphosphonates –reduces risk of vertebral fractures only
 – Raloxifene –decreases risk of ER+ve breast cancer – Increases risk of DVT/PE – Used mainly if intolerant of bisphosphonates –reduces risk of vertebral fractures only")
30
Teriparatide –recombinant 1-34 parathyroid hormone –sc daily injection –Reduce vertebral and non-vertebral, but NOT hip –EXPENSIVE!

31
HRT –risk outweighs benefits? –Young women with high risk of fracture and symtomatic menopause

32
Vitamin D and Calcium Contentious preventative treatment 2 french nursing home studies demonstrate decrease in fractures primary care randomised study from York shows no change (BMJ 30th April 05) Aberdeen study shows similar results (Lancet 28th April 05) However - ALL other agents were trialled whilst taking both Calcium and Vit D
 Aberdeen study shows similar results (Lancet 28th April 05) However - ALL other agents were trialled whilst taking both Calcium and Vit D")
33
Non-pharmacological Weight loaded exercise stop smoking “bone-friendly diet” decrease ETOH consumption avoid high doses Vitamin A (ie cod liver oil!) Reduce risk of falls
 Reduce risk of falls")
Similar presentations









>")












