Download presentation
Presentation is loading. Please wait.

1
Dolly Mehta 5-0236

2
Methicillin-resistant Staphylococcus aureus (MRSA)
Vancomycin-Resistant Enterococci (VRE) i.e. E. faecium TB Superbug: NDM-1 (New Delhi metallo-beta-lactamase bacteria)
 i.e. E. faecium. TB. Superbug: NDM-1 (New Delhi metallo-beta-lactamase. bacteria)")
3
Cell Wall Synthesis inhibitors Protein Synthesis inhibitors
Beta-Lactum Non Beta-Lactum Aminoglycosides Macrolides Streptogramins Lincosamides Oxazolidinones Tetracyclines Chloramphenicol Penicillins Cephalosporins Carbapenams Azetronam Vancomycin Fosfomycin Cycloserine Bacitracin Anti-tuberculosis and Anti-Leprosy (RNA, Cell wall, cell membrane) (special class of bacteria: Mycobacterium) Rifampin, Isoniazid, Pyrazinamide, Ethambutol/streptomycin Amikacin, linezolid, clindamycin Dapsone
 (special class of bacteria: Mycobacterium) Rifampin, Isoniazid, Pyrazinamide, Ethambutol/streptomycin. Amikacin, linezolid, clindamycin. Dapsone.")
4
Cell Wall Gram Positive Mycobacteium Gram Negative Cell wall AG PG
AG: Arabanioglactan PG: peptidoglycan Mycolic acid AG Cell wall Cell memb Mycobacteium Cell wall

5
Overview of cell wall synthesis
Peptidoglycan N acetylmuramic acid (NAM) NAM N acetylglucosamine (NAG) NAG Penta peptide Glycine
 NAM. N acetylglucosamine (NAG) NAG. Penta peptide Glycine.")
6
Bactoprenol (C55-carrier or lipid carrier)
D-ala L-ala alanine racemase D-ala D-ala D-ala D-ala D-ala M UDP D-glu L-lys D-ala-D-ala-ligase UMP P NAM Bactoprenol (C55-carrier or lipid carrier) NAG P BP M UDP L-ala periplasm autolysin NAM UDP NAM NAG NAG NAM NAM Mur-A NAG UDP NAM NAM NAM Glycosidic bond Peptide cross link Peptidoglycan units
 NAG. P. BP. M. UDP. L-ala. periplasm. autolysin. NAM. UDP. NAM. NAG. NAG. NAM. NAM. Mur-A. NAG. UDP. NAM. NAM. NAM. Glycosidic bond. Peptide cross link. Peptidoglycan units.")
7
P P periplasm P BP BP NAG NAM NAG NAM NAG NAM NAM NAM NAG NAM NAM NAM

8
(penicillin binding proteins)
BP periplasm NAG NAM NAG NAM NAG NAM NAM Peptide cross link Transpeptidase (penicillin binding proteins) NAM NAG NAM NAG NAM NAM NAM Glycosidic bond Transglycolase
 NAM. NAG. NAM. NAG. NAM. NAM. NAM. Glycosidic bond. Transglycolase.")
9
Cell wall synthesis inhibitors
D-ala alanine racemase D-ala D-ala cycloserine D-ala D-ala-D-ala-ligase D-ala L-ala D-ala D-ala D-ala D-ala vancomycin bacitracin NAG UDP MurA NAM P NAM fosfomycin Bactoprenol (C55-carrier or lipid carrier) NAG P P P BP BP PBP Beta-lactams periplasm Inhibits transglycolase reaction NAG NAM NAG NAM NAG NAM NAM Inhibits Transpeptidase reaction NAM NAG NAM NAG NAM NAM NAM
 NAG. P. P. P. BP. BP. PBP. Beta-lactams. periplasm. Inhibits transglycolase. reaction. NAG. NAM. NAG. NAM. NAG. NAM. NAM. Inhibits. Transpeptidase. reaction. NAM. NAG. NAM. NAG. NAM. NAM. NAM.")
10
Increased expression of efflux pumps (i.e P. aeruginosa)
Mechanism of resistance for beta-lactums Reduced penetration to site of action (Penn G); P. aeruginosa (lack porins) Production of b-lactamase Increased expression of efflux pumps (i.e P. aeruginosa) Elaboration of normal penicillin binding proteins (PBPs)
; P. aeruginosa (lack porins) Production of b-lactamase. Increased expression of efflux pumps (i.e P. aeruginosa) Elaboration of normal penicillin binding proteins (PBPs)")
11
Mechanism of Resistance for Vancomycin
modification of the D-Ala-D-Ala binding site in PG building block. D-Ala is replaced by D-lactate. P NAM P NAM

12
Case Study A 55-year-old man is brought to the local hospital emergency department by ambulance. His wife reports that he had been in his normal state of health until 3 days ago when he developed a fever and a productive cough. During the last 24 hours he has complained of a headache and is increasingly confused. His wife reports that his medical history is significant only for hypertension, for which he takes hydrochlorothiazide and lisinopril, and that he is allergic to amoxicillin. She says that he developed a rash many years ago when prescribed amoxicillin for bronchitis. In the emergency department, the man is febrile (38.7°C [101.7°F]), hypotensive (90/54 mm Hg), tachypneic (36/min), and tachycardic (110/min). He has no signs of meningismus but is oriented only to person. A stat chest x-ray shows a left lower lung consolidation consistent with pneumonia. The plan is to start empiric antibiotics and perform a lumbar puncture to rule out bacterial meningitis. What antibiotic regimen should be started to treat both pneumonia and meningitis? Does the history of amoxicillin rash affect the antibiotic choice? Why or why not?
, hypotensive (90/54 mm Hg), tachypneic (36/min), and tachycardic (110/min). He has no signs of meningismus but is oriented only to person. A stat chest x-ray shows a left lower lung consolidation consistent with pneumonia. The plan is to start empiric antibiotics and perform a lumbar puncture to rule out bacterial meningitis. What antibiotic regimen should be started to treat both pneumonia and meningitis Does the history of amoxicillin rash affect the antibiotic choice Why or why not")
13
b-lactamase Inhibitors Penicillin Cephalosporins Carbapenams
Clavulanic acid (“suicide inhibitor”) Sulbactum Tazobactum Penicillin Cephalosporins Cephalothin Cefazolin Cefoxitin, Cefotetan cefmetazole Ceftazidime, cefoperazone Cefepime Carbapenams Imepenam (combined with cilastatin; Primaxin) Meropenam Etrapenam Vancomycin Fosfomycin Monurol Penicillin G, Natural Penicillin V Repository forms of Penn G: Wycillin Bicillin Penicillinase resistant Penicillin (anti-staphyloccal penicillins) (strains not resistant to methacillin: nafcillin, oxacillin dicloxacilin) Ampicillin, Amoxicllin Ticarcillin : Anti-pesudomonal (i.v) Piperacillin Monobactum Azteronam (does not exhibit cross-allergy with Penn and Cef Excluding ceftazidime)
 Sulbactum. Tazobactum. Penicillin. Cephalosporins. Cephalothin. Cefazolin. Cefoxitin, Cefotetan. cefmetazole. Ceftazidime, cefoperazone. Cefepime. Carbapenams. Imepenam. (combined with cilastatin; Primaxin) Meropenam. Etrapenam. Vancomycin. Fosfomycin. Monurol. Penicillin G, Natural. Penicillin V. Repository forms of Penn G: Wycillin. Bicillin. Penicillinase resistant Penicillin. (anti-staphyloccal penicillins) (strains not resistant to. methacillin: nafcillin, oxacillin. dicloxacilin) Ampicillin, Amoxicllin. Ticarcillin : Anti-pesudomonal. (i.v) Piperacillin. Monobactum. Azteronam. (does not exhibit. cross-allergy with. Penn and Cef. Excluding. ceftazidime)")
14
Amoxicillin + clavulanate: Augementin (oral)
Ampicillin + Sulbactam: Unasyn Piperacillin +Tazobactam: Zosyn Ticarcillin and Clavulanate: Timentin

15
Carboxypenicillin and Ureidiopenicillin (Tricarcillin, Pipericillin)
Cephalosporins Carbapenams Vancomycin Penicillin G/V Ist generation i.e. Cefazolin Imepenam (Primaxin) Pneumococcal Infections (S. pneumoniae) Pneumococcal Peumonia/meningitis (only penicillin sensitive) Streptococcal Infections Enterococcal endocarditis (+ ampilcillin) Meningococcal infections Syphilis Actinomycosis Clostridia Infections Listeria infections (along with Ampicillin) Prophylactic: Streptococcal and rheumatoid fever Skin and soft tissue infections caused by S aureus, S pyogens; Surgical prophylaxis Celluulitis, endocarditis lower respiratory tract infections Urinary tract infections (UTI) Intra-abdominal, gynecological, skin and soft tissues infections Methicillin-resistent staph infections: Peumonia, empyema, endocarditis,Osteolmyelitis Soft-tissues abscesses Enterococcal endocardiatis (+ aminoglycosides in patients with serious penn allergy) IIIrd generation Meropenam All forms of Gonorrhea Severe form of Lyme disease Pneumococcal Meningitis (+ vancomycin) (non-immunocompromised) Pneumococcal Peumonia Typhoid Therapeutic equivalent to Prixamin Fosfomycin Etrapenam uncomplicated UTI (acute cystitis) in women due to susceptible strains of Escherichia coli and Enterococcus faecalis Abdominal and pelvic infections by Gram + Aminopenicillin IVth generation Otitis media Dental infection and endocarditis prophylaxis Upper respiratory tract infections Urinary tract infections (UTI) Listeria monocytogenes Enterococcal infections Noscomal infections Neutrpenia with fever Ventilator-associated pneumonia Azteronam Resembles aminoglycosides Use for gram – infections in patients with B-lactum allegenicity Bacitracin topical Penicillinase-resistant penicillins (PRPs): Skin infections: cellulitis, impetigo, erysipelas Endocarditis, meningitis, and bacteremia from staphylococci Osteomyelitis and septic arthritis only when the organism is proven sensitive Amoxicillin + clavulanate: Augementin (oral): low risk febrile patients with neutropenia from cancer therapy, acute otitis in childerns, bite wounds, cellulitis and diabetic foot infections Ampicillin + Sulbactam: Unasyn: good for Gram+ cocci, Intra-abdominal and pelvic infections Piperacillin +Tazobactam: Zosyn: Appendicitis (complicated by rupture or abscess) and peritonotis, community and hospital acquired pneumonia, Postpartum endometritis, cellulitis Ticarcillin and Clavulanate: Timentin: Septicemia, Lower Respiratory Infections, UTI, Intra-abdominal, bone-joint, gynecological, skin and soft tissues infections Carboxypenicillin and Ureidiopenicillin (Tricarcillin, Pipericillin) In Neutropenic patients, Bacteremia, pneumonia, burns infections, UTI (resistant to Penn G and Ampicillin caused by Pseudomonas or indole + proteus Infections and enterobacter strains), Hospital-acquired and ventilator-associated pneumonia
 Pneumococcal Infections (S. pneumoniae) Pneumococcal Peumonia/meningitis. (only penicillin sensitive) Streptococcal Infections. Enterococcal endocarditis (+ ampilcillin) Meningococcal infections. Syphilis. Actinomycosis. Clostridia Infections. Listeria infections (along with Ampicillin) Prophylactic: Streptococcal and. rheumatoid fever. Skin and soft tissue infections caused by S aureus, S pyogens; Surgical prophylaxis. Celluulitis, endocarditis. lower respiratory tract infections. Urinary tract infections (UTI) Intra-abdominal, gynecological, skin and soft tissues infections. Methicillin-resistent staph infections: Peumonia, empyema, endocarditis,Osteolmyelitis. Soft-tissues abscesses. Enterococcal endocardiatis. (+ aminoglycosides in patients with serious penn allergy) IIIrd generation. Meropenam. All forms of Gonorrhea. Severe form of Lyme disease. Pneumococcal Meningitis (+ vancomycin) (non-immunocompromised) Pneumococcal Peumonia. Typhoid. Therapeutic equivalent to Prixamin. Fosfomycin. Etrapenam. uncomplicated UTI (acute cystitis) in women due to susceptible strains of Escherichia coli and Enterococcus faecalis. Abdominal and pelvic infections by Gram + Aminopenicillin. IVth generation. Otitis media. Dental infection and. endocarditis prophylaxis. Upper respiratory tract infections. Urinary tract infections (UTI) Listeria monocytogenes. Enterococcal infections. Noscomal infections. Neutrpenia with fever. Ventilator-associated pneumonia. Azteronam. Resembles aminoglycosides. Use for gram – infections in patients with B-lactum allegenicity. Bacitracin. topical. Penicillinase-resistant penicillins (PRPs): Skin infections: cellulitis, impetigo, erysipelas. Endocarditis, meningitis, and bacteremia from staphylococci. Osteomyelitis and septic arthritis only when the organism is proven sensitive. Amoxicillin + clavulanate: Augementin (oral): low risk febrile patients with neutropenia from cancer therapy, acute otitis in childerns, bite wounds, cellulitis and diabetic foot infections. Ampicillin + Sulbactam: Unasyn: good for Gram+ cocci, Intra-abdominal and pelvic infections. Piperacillin +Tazobactam: Zosyn: Appendicitis (complicated by rupture or abscess) and peritonotis, community and hospital acquired pneumonia, Postpartum endometritis, cellulitis. Ticarcillin and Clavulanate: Timentin: Septicemia, Lower Respiratory Infections, UTI, Intra-abdominal, bone-joint, gynecological, skin and soft tissues infections. Carboxypenicillin and Ureidiopenicillin. (Tricarcillin, Pipericillin) In Neutropenic patients, Bacteremia, pneumonia, burns infections, UTI (resistant to Penn G and Ampicillin caused by. Pseudomonas or indole + proteus Infections and. enterobacter strains), Hospital-acquired and ventilator-associated pneumonia.")
16
Untoward Effects Penicillin’s Vancomycin Cephalosporin’s
Hypersensitivity (macular rashes and anaphylaxis) “red neck syndrome” Ototoxicity (excessive high conc.) Hypersensitivity ~(0.7%-10%) Allergy to one penicillin risk to other penicillin's/cephalosporin’s (in clinical setting it is 1%) also cases with low and mild Penicillin allergy are low risk for cephalosporin’s) Cephalosporin’s Hypersensitivity Nephrotoxic increases with Aminoglycosides Diarrhea Intolerance to alcohol (cefotetan, cefoperazone) Thrombocytopenia/platelet dysfunction and disulfaram-like effect (apparent with these: cefamandole, cefmetazole, cefotetan,and cefoperazone), Vit K deficiency Penicilloic acid IgE Abs
 red neck syndrome Ototoxicity (excessive high conc.) Hypersensitivity ~(0.7%-10%) Allergy to one penicillin risk to other penicillin s/cephalosporin’s (in clinical setting it is 1%) also cases with low and mild Penicillin allergy are low risk for cephalosporin’s) Cephalosporin’s. Hypersensitivity. Nephrotoxic increases with. Aminoglycosides. Diarrhea. Intolerance to alcohol (cefotetan, cefoperazone) Thrombocytopenia/platelet dysfunction and disulfaram-like effect (apparent with these: cefamandole, cefmetazole, cefotetan,and cefoperazone), Vit K deficiency. Penicilloic acid. IgE Abs.")
17
Protein Synthesizing Machinery
Ribosome mRNA tRNA bacteria has 50S and 30 S subunit which forms 70 S polysome that slides on mRNA has A, P and E sites for binding with tRNA forms template for protein synthesis transcribed from DNA attaches to 30s ribosomes brings amino acids attaches to A, P and E sites of ribosomes

18
uuu cca cau cca aug cca cau
MET uac P E A 50s uuu cca cau cca aug cca cau 30s

19
uuu cca cau cca aug cca cau
Pro uac P E A Met uac uuu cca cau cca aug cca cau

20
uuu cca cau cca aug cca cau
P E A Pro Met gga uuu cca cau cca aug cca cau

21
uuu cca cau cca aug cca cau
P E A Met Pro uuu cca cau cca aug cca cau

22
uuu cca cau cca aug cca cau
Aminoglycosides MET uac Binds 30S (irreversible inhibitor of protein synthesis) P E A 50s uuu cca cau cca aug cca cau 30s
 P. E. A. 50s. uuu cca cau cca aug cca cau. 30s.")
23
uuu cca cau cca aug cca cau
Pro uac Tetracycline Binds reversibly at 30 S ribosomal RNA Compete with tRNA P E A Met uac uuu cca cau cca aug cca cau

24
Macrolides, Lincosamide, Streptogramins
50S ribosomal RNA Blocks peptide translocation to P site P E A Met Pro uuu cca cau cca aug cca cau

25
Chloramphenicol, Clindamycin
50S ribosomal RNA Inhibit peptidyltransferase P E A Pro Met gga uuu cca cau cca aug cca cau

26
Oxazolidinones Inhibits ribosomal complex formation P E A 50s uuu cca cau cca aug cca cau 30s

27
Aminoglycosides concentration-dependent killing postantibiotic effect
Enter cell through porins but require electron transport to permeate the inner membrane Energy-Dependent Phase 1(EDP1) b) Create fissure enhancing AG uptake (EDP2 phase) Aminoglycosides concentration-dependent killing postantibiotic effect Peak and trough levels of Aminoglycosides therapeutic dose is achieved avoid toxicity Synergistic killing Along with beta-lactam or vancomycin
 b) Create fissure enhancing AG uptake (EDP2 phase) Aminoglycosides. concentration-dependent killing. postantibiotic effect. Peak and trough levels of Aminoglycosides. therapeutic. dose is achieved. avoid toxicity. Synergistic killing. Along with beta-lactam or vancomycin.")
28
Mechanisms of resistance for antibiotics inhibiting protein synthesis
Intracellular penetration AG, Tet, Mac Anaerobic conditions (AG) pH Efflux pumps (Tet, Mac) Low affinity of drug for bacterial ribosomes Modification of the ribosomal binding site (AG, Tet, Mac) acetylation, phosphorylation, adenylation of OH or NH2 gr (AG) Drug Inactivation Tet: enzyme inactivation Mac: (hydrolysis by esterase's)
 pH. Efflux pumps (Tet, Mac) Low affinity of drug for bacterial ribosomes. Modification of the ribosomal binding site. (AG, Tet, Mac) acetylation, phosphorylation, adenylation of OH or NH2 gr (AG) Drug Inactivation. Tet: enzyme inactivation. Mac: (hydrolysis by esterase s)")
29
Gentamicin Tetracycline Erythromycin Tobramycin Doxycycline
Aminoglycosides Macrolides Erythromycin Azithromycin Clarithromycin Ketolide (Telithromycin) Tetracyclines Tetracycline Doxycycline Minocycline Tigecycline Steptogramins Quinupristin/dalfopristin Chloramphenicol Gentamicin 2-deoxystreptamine Linocosamides Clindamycin Gentamicin Tobramycin Amikacin Streptomycin Neomycin Oxazolidinones Spectinomycin Linezolid
 Tetracyclines. Tetracycline. Doxycycline. Minocycline. Tigecycline. Steptogramins. Quinupristin/dalfopristin. Chloramphenicol. Gentamicin. 2-deoxystreptamine. Linocosamides. Clindamycin. Gentamicin. Tobramycin. Amikacin. Streptomycin. Neomycin. Oxazolidinones. Spectinomycin. Linezolid.")
30
Aminoglycosides Macrolides Tetracycline Chloramphenicol Gentamicin
MUST BE LIMITED Gentamicin Tobramycin Amikacin Erythromycin, Chlamydial urogenital infections (pregnancy) Chlamydial pneuominia in infants Diphtheria Pertussis Tetanus prophylaxis of rheumtoid fever Azithromycin Legionnaires disease Lymphogranuloma venereum Pneumonia by Chlamydia pneumonia Streptococcal infections Mycobacterial infections Toxoplasmosis encephalitis and diarrhea (in AIDS) Non specific urethritis Clarithromycin Helicobacter pylori infections Ketolide Respiratory tract infections (bronchitis, sinusitis) Community acquired pneumonia Tetracyclines Rickettsial infections Mycoplasma infections Peumonia, bronchitis, sinusitis caused by Chlamyda peumonia Brucellosis (along with rifampin or Streptomycin) Tuleremia Acne Doxycycline Rocky mountain fever Lymphogranuloma venereum Trachoma Anthrax cholera Typhoid fever Bacterial menegitis Anaerobic infections (intrabdominal or brain) Rickettsial infections Brucellosis (Gentamicin prefered due to low cost and long experience Steptogramins Dalfopristin (Synercid) (should be reserved for serious infections by multiple-drug-resitant gram+ along with Penn and Cef for serious UTI, bacteremia, infected burns, osteomyelitis, pneumonia, peritonitis and otitis along with vancomycin For bacterial endocarditis Never than a few days unless required Never mixed in same solution with Penn as it inactivates Infections caused by Vancomycin resistant strains Noscomal infections (Europe) Limezoid (Zyvox) should be reserved for serious infections by multiple-drug-resistant gram+ and vancomycin resistant or multi-drug resistant gram+ Streoptomycin With Penn for bacterial endocarditis Tularemia Plague Tuberculosis Clindamycin Lung abscess and anerobic lung and pleural space infections, encephalitis, vaginal infections Neomycin: topical Spectinomycin gonorrhea or gonorrhea in penicillin-allergic patients
 Chlamydial pneuominia in infants. Diphtheria. Pertussis. Tetanus. prophylaxis of rheumtoid fever. Azithromycin. Legionnaires disease. Lymphogranuloma venereum. Pneumonia by Chlamydia pneumonia. Streptococcal infections. Mycobacterial infections. Toxoplasmosis encephalitis. and diarrhea (in AIDS) Non specific urethritis. Clarithromycin. Helicobacter pylori infections. Ketolide. Respiratory tract infections (bronchitis, sinusitis) Community acquired pneumonia. Tetracyclines. Rickettsial infections. Mycoplasma infections. Peumonia, bronchitis, sinusitis caused by Chlamyda peumonia. Brucellosis (along with rifampin or Streptomycin) Tuleremia. Acne. Doxycycline. Rocky mountain fever. Lymphogranuloma venereum. Trachoma. Anthrax. cholera. Typhoid fever. Bacterial menegitis. Anaerobic infections. (intrabdominal or brain) Rickettsial infections. Brucellosis. (Gentamicin prefered due to. low cost and long experience. Steptogramins. Dalfopristin (Synercid) (should be reserved for serious infections by multiple-drug-resitant gram+ along with Penn and Cef. for serious UTI, bacteremia, infected burns, osteomyelitis, pneumonia, peritonitis and otitis. along with vancomycin. For bacterial endocarditis. Never than a few days unless required. Never mixed in same solution with Penn as it inactivates. Infections caused by. Vancomycin resistant strains. Noscomal infections (Europe) Limezoid (Zyvox) should be reserved for serious infections by multiple-drug-resistant gram+ and vancomycin resistant or multi-drug resistant gram+ Streoptomycin. With Penn for bacterial endocarditis. Tularemia. Plague. Tuberculosis. Clindamycin. Lung abscess and anerobic lung and pleural space infections, encephalitis, vaginal infections. Neomycin: topical. Spectinomycin. gonorrhea or gonorrhea in penicillin-allergic patients.")
31
Untoward Effects Linezolid Aminoglycosides Macrolides Chloramphenicol
Allergic reactions (fever, eosinophilia, skin eruptions) Cholestatic hepatitis Ketolide Nausea, vomiting Visual disturbances Pseudomembrane colitis Risk of ventricular arrhythmia Chloramphenicol Hematological toxicity (aplastic aneamia) Hypersensitity Gray baby syndrome Ototoxicity (vestibular or cochlear cells) (largely irreversible); Ethacrynic acid and furosemide further aggravate it Nephrotoxicity (8-26% of cases) (with cephalosporins) Neuromuscular blockade Clindamycin Diarrhoea Pseudomembrane colitis (lethal) Skin rashes May inhibit neuromuscular transmission or potentiate the effect of neuroblocker agents Tetracyclines Gastrointestinal Pseudomembrane colitis Photosensitivity Hepatic toxicity (pregnant woman) Renal toxicity (less with doxycycline) Fanconi syndrome with degraded Tet Permanent teeth discoloration in children's Linezolid Well-tolerated, but myelosuppression has been noted; platelets should be monitored in patients with risk of bleeding or if therapy >2 wks Palpitation, headache Dalfopristin Phelebitis Raise blood pressure if gibven along with other agents i.e. histamine
 Cholestatic hepatitis. Ketolide. Nausea, vomiting. Visual disturbances. Pseudomembrane colitis. Risk of ventricular arrhythmia. Chloramphenicol. Hematological toxicity. (aplastic aneamia) Hypersensitity. Gray baby syndrome. Ototoxicity (vestibular or cochlear cells) (largely irreversible); Ethacrynic acid and. furosemide further aggravate it. Nephrotoxicity (8-26% of cases) (with cephalosporins) Neuromuscular blockade. Clindamycin. Diarrhoea. Pseudomembrane colitis (lethal) Skin rashes. May inhibit neuromuscular transmission or potentiate the effect of neuroblocker agents. Tetracyclines. Gastrointestinal. Pseudomembrane colitis. Photosensitivity. Hepatic toxicity (pregnant woman) Renal toxicity (less with doxycycline) Fanconi syndrome with degraded Tet. Permanent teeth discoloration in. children s. Linezolid. Well-tolerated, but myelosuppression has been noted; platelets should be monitored in patients with risk of bleeding or if therapy >2 wks. Palpitation, headache. Dalfopristin. Phelebitis. Raise blood pressure if gibven along with other agents i.e. histamine.")
32
Erythromycin/clathrimycin/ketolide
Drug Interactions Chloramphenicol, Streptogramins CYP450 Prolong half lives of dicumbarol, warfarin Antiretroviral protease inhibitors rifabutin Erythromycin/clathrimycin/ketolide CYP3A4 Potentiates the effects of i.e. Carbamazepine, cotoicosteriods, cyclosporin, digoxin, warfarin Linezolid serotonin syndrome If given with Serotonergic drugs

33
Case Study A 19-year-old woman with no significant past medical history presents to her college medical clinic complaining of a 2-week history of foul-smelling vaginal discharge. She denies any fever or abdominal pain but does report vaginal bleeding after sexual intercourse. When questioned about her sexual activity, she reports having vaginal intercourse, at times unprotected, with two men in the last 6 months. A pelvic examination is performed and is positive for mucopurulent discharge from the endocervical canal. No cervical motion tenderness is present. A first-catch urine specimen is obtained to be tested for chlamydia and gonococcus. A pregnancy test is also ordered as the patient reports she "missed her last period." Pending these results, the decision is made to treat her empirically for gonococcal and chlamydial cervicitis. What are two potential treatment options for her possible chlamydial infection? How does her potential pregnancy affect the treatment decision?

34
Case Study A 45-year-old man with no medical history was admitted to the intensive care unit (ICU) 10 days ago after suffering third-degree burns over 40% of his body. He had been relatively stable until the last 24 hours. Now he is febrile (39.5°C [103.1°F]), and his white blood cell count has risen from 8,500 to 20,000/mm3. He has also had an episode of hypotension (86/50 mm Hg) that responded to a fluid bolus. Blood cultures were obtained at the time of his fever and results are pending. The ICU attending physician is concerned about sepsis and decides to treat with empiric combination therapy directed against Pseudomonas. The combination therapy includes tobramycin. The patient weighs 70 kg (154 lb) and has an estimated creatinine clearance of 90 mL/min. How should tobramycin be dosed using once-daily and conventional dosing strategies? How should each regimen be monitored for efficacy and toxicity?
 10 days ago after suffering third-degree burns over 40% of his body. He had been relatively stable until the last 24 hours. Now he is febrile (39.5°C [103.1°F]), and his white blood cell count has risen from 8,500 to 20,000/mm3. He has also had an episode of hypotension (86/50 mm Hg) that responded to a fluid bolus. Blood cultures were obtained at the time of his fever and results are pending. The ICU attending physician is concerned about sepsis and decides to treat with empiric combination therapy directed against Pseudomonas. The combination therapy includes tobramycin. The patient weighs 70 kg (154 lb) and has an estimated creatinine clearance of 90 mL/min. How should tobramycin be dosed using once-daily and conventional dosing strategies How should each regimen be monitored for efficacy and toxicity")
35
Key facts about TB Second only to HIV/AIDS as the greatest killer worldwide In 2010, 8.8 million people fell ill with TB and 1.4 million died from TB. Over 95% of TB deaths occur in low- and middle-income countries, and it is among the top three causes of death for women aged 15 to 44. In 2009, there were about 10 million orphan children as a result of TB deaths among parents. 8 infants exposed to TB at Sacramento hospital (just yesterday) leading killer of people living with HIV causing one quarter of all deaths. Multi-drug resistant TB (MDR-TB) is present in virtually all countries surveyed. Millennium Development Goal to reverse the spread of TB by 2015.
 leading killer of people living with HIV causing one quarter of all deaths. Multi-drug resistant TB (MDR-TB) is present in virtually all countries surveyed. Millennium Development Goal to reverse the spread of TB by")
36
X Mycobacterium Penicillin Cephallosprins Vancomycin Cell wall
Mycolic acid Cell wall Aminoglycosides Streptomycin(ist line) Kanamycin AG PG Amikacin AG: Arabanioglactan PG: peptidoglycan cycloserine Cell memb Mycobacterium tuberculosis: slow growing, dormant and aerobic bacterium. Mycolic acids fatty acids provide advantage Reside in Macrophages Active TB disease, Mtb complexes are always found in the upper air sacs of the lungs.
 Kanamycin. AG. PG. Amikacin. AG: Arabanioglactan. PG: peptidoglycan. cycloserine. Cell memb. Mycobacterium tuberculosis: slow growing, dormant and aerobic bacterium. Mycolic acids fatty acids provide advantage. Reside in Macrophages. Active TB disease, Mtb complexes are always found in the upper air sacs of the lungs.")
37
First-line Therapy Alternative Therapy “RIPE” Rifampin Isoniazid
Pyrazinamde Ethambutol Streptomycin Rifabutin Alternative Therapy Fluoroquinolones (Moxifloxacin, gatifloxacin) cycloserine capreomycin Kanamycin and amikacin ethionamide clofazimine aminosalicyclic acid
 cycloserine. capreomycin. Kanamycin and amikacin. ethionamide. clofazimine. aminosalicyclic acid.")
38
Inhibitors of cell wall and cell membrane
Ethionamide (alternate) Isoniazid (INH) Ethambutol arabinosyltransferase Arabinoglycan Pyrazinamide pyrazinoic acid (prodrug) pyrazinamidase disrupts mycobacterial cell membrane metabolism and transport functions (prodrug) Catalase-peroxidase (KatG) KasA INH AcpM Fatty acid Synthase II Mycolic acid synthesis
 Isoniazid (INH) Ethambutol. arabinosyltransferase. Arabinoglycan. Pyrazinamide. pyrazinoic acid. (prodrug) pyrazinamidase. disrupts mycobacterial cell membrane metabolism and transport functions. (prodrug) Catalase-peroxidase. (KatG) KasA. INH. AcpM. Fatty acid Synthase II. Mycolic acid synthesis.")
39
Targeting mycobacterium DNA or RNA
Rifamycin Fluoroquinolones (alternate) Inhibition of DNA synthesis and supercoling targets topoisomerase
 Inhibition of DNA synthesis and supercoling. targets topoisomerase.")
40
mycobacterium protein synthesis inhibitors
Inhibits folate synthesis: Aminosalicylic Acid (PAS) Streptomycin (toxic) Capreomycin/amikacin (alternate) Macrolides
 Streptomycin (toxic) Capreomycin/amikacin (alternate) Macrolides.")
41
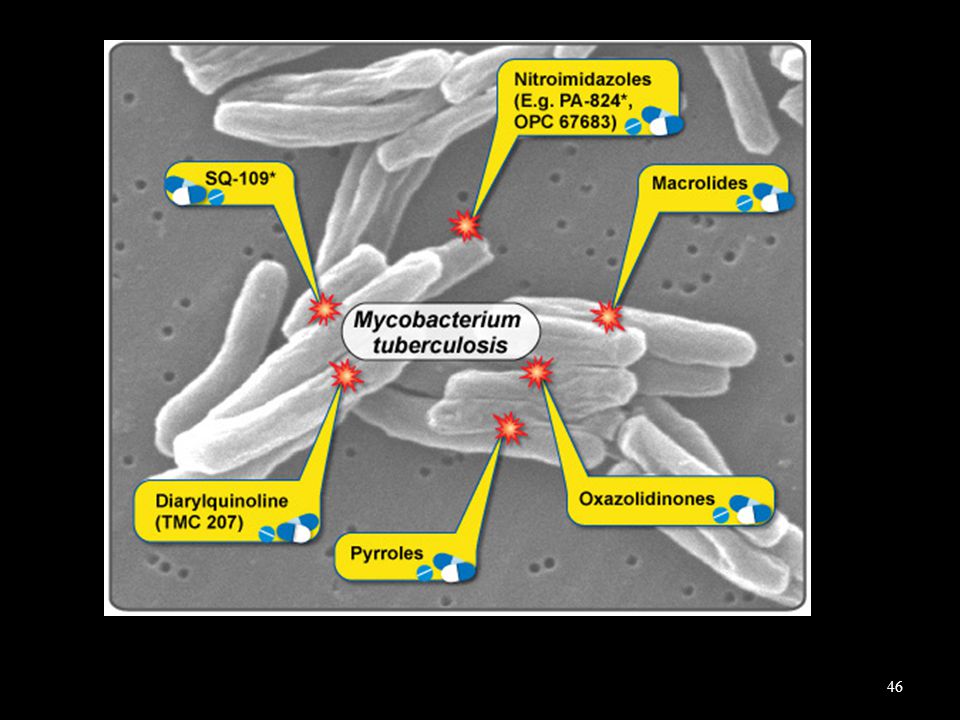
Experimentsl drugs targeting mycobacterium
TM-207 (R207910)
")
42
Mechanism of Mycobacterial Resistance
butol) Alteration of enzyme converting prodrug Ethionamide Pyrazinamde, Isoniazid inactive active
 Alteration of enzyme converting prodrug. Ethionamide. Pyrazinamde, Isoniazid. inactive. active.")
43
Alteration of target protein structure
Blocks the action of rifamycin, fluroquinolone, ethambutol, streptomycin, macrolide

44
Multidrug-Resistant Tuberculosis (MDR TB) and Possible Effective Treatments
 and Possible Effective Treatments")
45
Extensively Drug-Resistant Tuberculosis (XDR TB) Diminishing Options for Treatment
 Diminishing Options for Treatment")
47
Drug Interactions of Rifampin
induces Cytochrome P450 Rifabutin (can be used) Increases elimination of several drugs i.e cyclosporine, anticonvulsants Protease inhibitors
 Increases elimination of several drugs i.e cyclosporine, anticonvulsants. Protease inhibitors.")
48
Atypical Mycobacteria
Accounts for 10% of non-tuberculous or atypical mycobacterium infections generally non communicable less susceptible than M tuberculosis to antituberculous drugs erythromycin, sulfonamides, or tetracycline, which are not active against M tuberculosis, may be effective

49
Drugs active against atypical Mycobacteria
Species Clinical Features Treatment Options M kansasii Resembles tuberculosis Ciprofloxacin, clarithromycin, ethambutol, isoniazid, rifampin, trimethoprim- sulfamethoxazole M marinum Granulomatous cutaneous disease Amikacin, clarithromycin, ethambutol, doxycycline, minocycline, rifampin, trimethoprim-sulfamethoxazole M scrofulaceum Cervical adenitis in children Amikacin, erythromycin (or other macrolide), rifampin, streptomycin (Surgical excision is often curative and the treatment of choice.) M avium complex Pulmonary disease in patients with chronic lung disease; disseminated infection in AIDS Amikacin, azithromycin, clarithromycin, ciprofloxacin, ethambutol, rifabutin M chelonae Abscess, sinus tract, ulcer; bone, joint, tendon infection Amikacin, doxycycline, imipenem, macrolides, tobramycin M fortuitum Amikacin, cefoxitin, ciprofloxacin, doxycycline, ofloxacin, trimethoprim-sulfamethoxazole M ulcerans Skin ulcers Isoniazid, streptomycin, rifampin, minocycline (Surgical excision may be effective
, rifampin, streptomycin (Surgical excision is often curative and the treatment of choice.) M avium complex Pulmonary disease in patients with chronic lung disease; disseminated infection in AIDS. Amikacin, azithromycin, clarithromycin, ciprofloxacin, ethambutol, rifabutin. M chelonae Abscess, sinus tract, ulcer; bone, joint, tendon infection. Amikacin, doxycycline, imipenem, macrolides, tobramycin. M fortuitum Amikacin, cefoxitin, ciprofloxacin, doxycycline, ofloxacin, trimethoprim-sulfamethoxazole. M ulcerans Skin ulcers. Isoniazid, streptomycin, rifampin, minocycline (Surgical excision may be effective.")
50
Leprosy Mycobacterium leprae chronic ID skin, peripheral nerves and mucous membranes (eyes, respiratory tract). also known as Hansen's disease as bacillus causing it was discovered by G.A. Hansen in 1873. common in warm, wet areas in the tropics & subtropics.

51
inhibits folate synthesis in bacteria
Multidrug therapy Sulphones (Dapsones) inhibits folate synthesis in bacteria Rifampin Clofazimine (LAMPRENE) Phenazine dye binds GC rich mycobacterial DNA; anti-inflammatory
 inhibits folate synthesis in bacteria. Rifampin. Clofazimine (LAMPRENE) Phenazine dye. binds GC rich mycobacterial DNA; anti-inflammatory.")
52
Sulphone syndrome: fever, jaundice, malaise
exacerbation of lepromatos leprosy Untoward Effects Dapsone Clofazimine skin discoloration ranging from red-brown to nearly black

53
Case Study A 45-year-old homeless man presents to the emergency department complaining of a 2-month history of fatigue, weight loss (10 kg), fevers, night sweats, and a productive cough. He is currently living on the street but has spent time in homeless shelters and prison in the last several years. He reports drinking 2–3 pints of hard alcohol per day for the last 15 years, and also reports a history of intravenous drug use. In the emergency department, a chest x-ray shows a right apical infiltrate. Given the high suspicion for pulmonary tuberculosis, the patient is placed in respiratory isolation. His first sputum smear shows many acid-fast bacilli, and a rapid HIV antibody test returns with a positive result. What drugs should be started for treatment of presumptive pulmonary tuberculosis? Does the patient have a heightened risk of developing medication toxicity? If so, which medication(s) would be likely to cause toxicity?
, fevers, night sweats, and a productive cough. He is currently living on the street but has spent time in homeless shelters and prison in the last several years. He reports drinking 2–3 pints of hard alcohol per day for the last 15 years, and also reports a history of intravenous drug use. In the emergency department, a chest x-ray shows a right apical infiltrate. Given the high suspicion for pulmonary tuberculosis, the patient is placed in respiratory isolation. His first sputum smear shows many acid-fast bacilli, and a rapid HIV antibody test returns with a positive result. What drugs should be started for treatment of presumptive pulmonary tuberculosis Does the patient have a heightened risk of developing medication toxicity If so, which medication(s) would be likely to cause toxicity")
54
A man is admitted with E. coli bacteremia
A man is admitted with E. coli bacteremia. Which of the following is the most appropriate therapy? Vancomycin Linezolid Quinolones, aminoglycosides, carbapenems, piperacillin, ticarcillin, or aztreonam Doxycycline Clindamycin Oxacillin A 34-year-old woman presents with facial pain, a discolored nasal discharge, bad taste in her mouth, and fever. On physical examination she has facial tenderness. What is the most appropriate management? Linezolid Amoxicillin / clavulanic acid and a decongestant Gentamycin Erythromycin and a decongestant

55
Objectives 1. Know the components of bacterial cell wall and basis of protein synthesis. 2.Know the classification of penicillins and cephalosporins according to their chemical structure and their antimicrobial spectrum. 3. Know the mechanism of antimicrobial activity for penicillins, cephalosporins, bacitracin. cyclosporin. aztreonam, imipenem, vancomycin, aminoglycosides, tetracyclines, macrolides, chloramphenicol, lincosamide, streptogramins, oxazolidinones,. 4. Know the mechanisms of bacterial resistance for antimicrobial drugs. 5. Know the most common adverse effects of the antimicrobial drugs. 6. Know the most common applications of these antibiotics for the treatment of disease.

Similar presentations





 Prof. Azza Elmedany.>")













