Download presentation
Presentation is loading. Please wait.

1
Post Partum Period Chapters 15 & 16 High Risk Chapter 22
Mary L. Dunlap MSN Fall 2015

2
Post Partum Begins immediately after child birth through the 6th post partum week Reproductive track returns to nonpregnant state Adaptation to the maternal role and modification to the family system

3
Safety for Mother and Infant
Prevent infant abductions Check ID bands Educate mother about safety measures

4
Infant ID Bands

5
Security Band

6
Clinical Assessment Receive report
Review Antepartum and Intrapartum history Determine educational needs Consider religious and cultural factors Assess for language barriers

7
Post Partum Assessment BUBBLE-EE
Breast Uterus Bladder Bowel Lochia Episiotomy Extremities Emotion

8
Vital signs Temperature Pulse Blood pressure Respirations

9
Pain Assessment Determine source/location and pain level
Interventions- based on pain Document location, type, pain level and intervention Reassess in 30 min and document pain level

10
Breast Initial assessment Inspect for size, contour, and asymmetry
Note if nipples are flat, inverted or erect Ongoing assessments Check for cracks, redness, or fissures Engorgement Mastitis

13
Breast Care Lactating Mother
Supportive bra Clean areola & nipples with water Air dry Express colostrum apply to areola & nipple Change breast pads frequently

14
Breast Care Non-Lactating Mother
Avoid stimulation Wear support bra 24hrs Ice packs or cabbage leaves Mild analgesic for discomfort

15
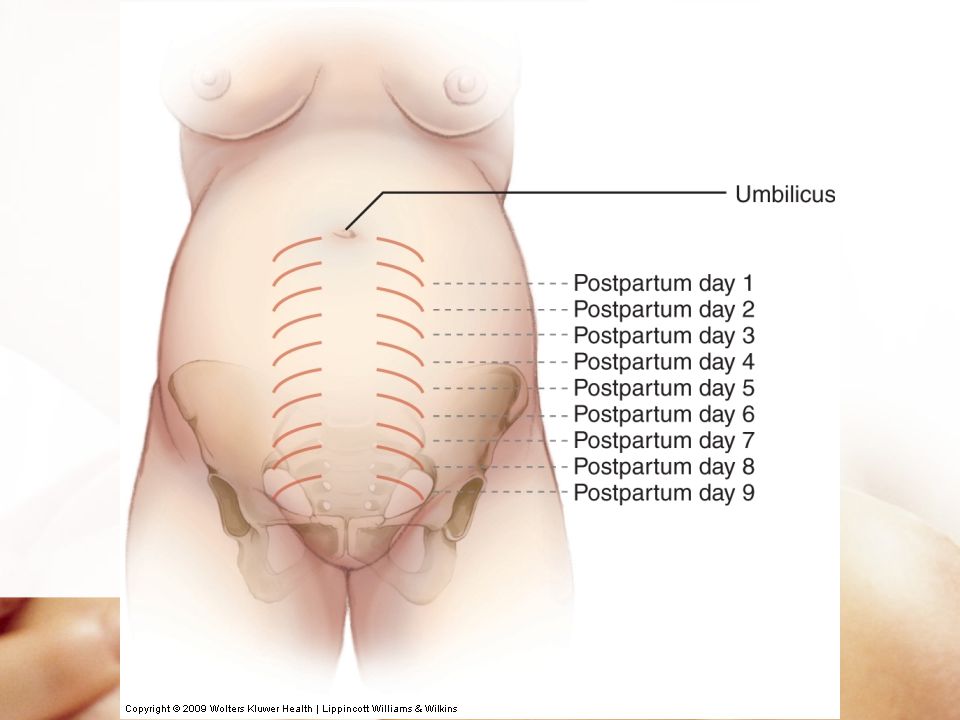
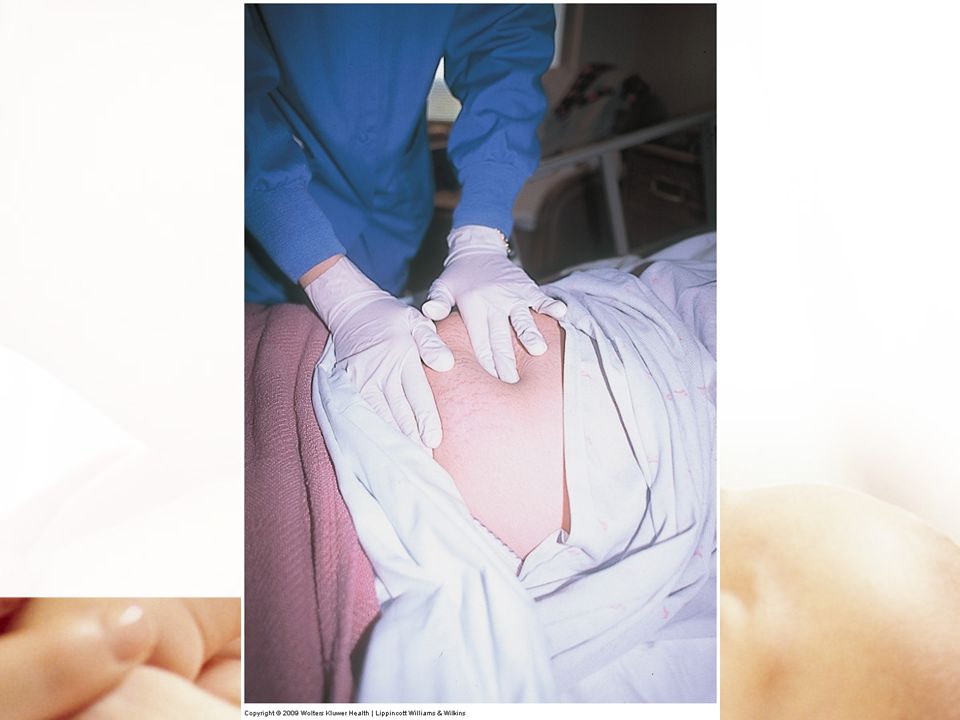
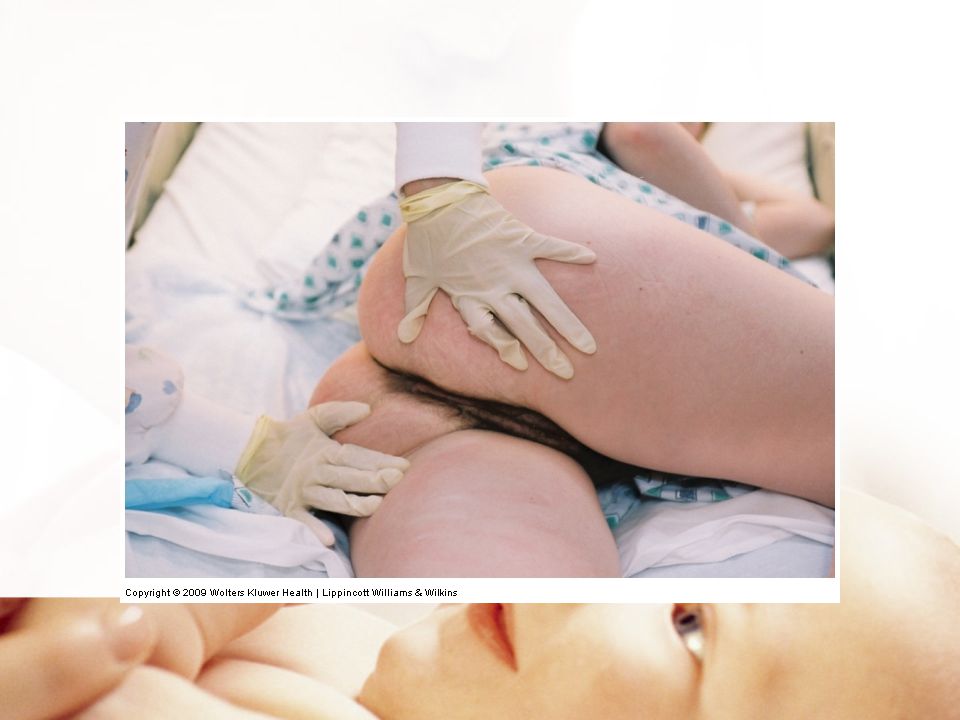
Assessment of Uterus After birth midline between umbilicus and the symphysis pubis Within 1h returns to the umbilicus Descends 1 cm/day Consistency- firm/boggy Height- measured in fingerbreadths Fundal massage procedure 22.1 p 753

20
Nursing care Boggy fundus- massage until firm
Medications- Pitocin, Methergine, Hemabate Teach new mom to massage her fundus

21
Afterpains Intermittent uterine contractions due to involution
Primiparous-mild Multipara- more pronounced Breastfeeding causes an increase in contractions due to release of oxytocin

22
Nursing Interventions
Patient in a prone position and place a small pillow to support her abdomen Ambulation Medicate with a mild analgesic

23
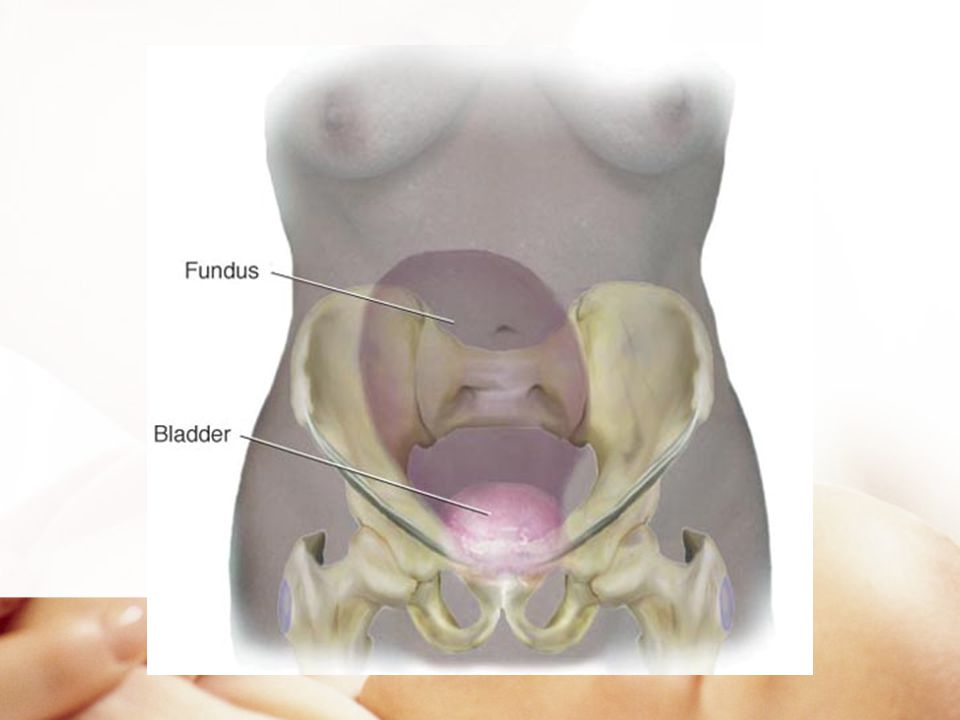
Bladder Monitor for bladder distention and displacement of uterus
Assess for voiding difficulty Monitor output Postpartum Diuresis

24
Nursing care Encourage frequent voiding every 4-6 hours
Monitor intake and output for 24 hrs Early ambulation Void within 4-6 hrs after birth Catheterize if unable to void

25
Preventing Stress Incontinence
Vaginal delivery causes direct pelvic muscle trauma and disruption of fascial support contributing to the development of urinary stress incontinence. Prevention strategies: Loss weight, avoid bladder irritates, decrease fluid intake Kegal exercises Teaching Guidelines pg

26
Bowel Relaxin depresses bowel motility Progesterone ↓ muscle tone
Diminished intra-abdominal pressure Incontinence if sphincter lacerated (4th degree) Spontaneous BM 2nd to 3rd post partum day Normal bowel pattern 8-14 days
 Spontaneous BM 2nd to 3rd post partum day. Normal bowel pattern 8-14 days.")
27
Nursing Care Increase fiber in diet 6-8 glasses of water or juice
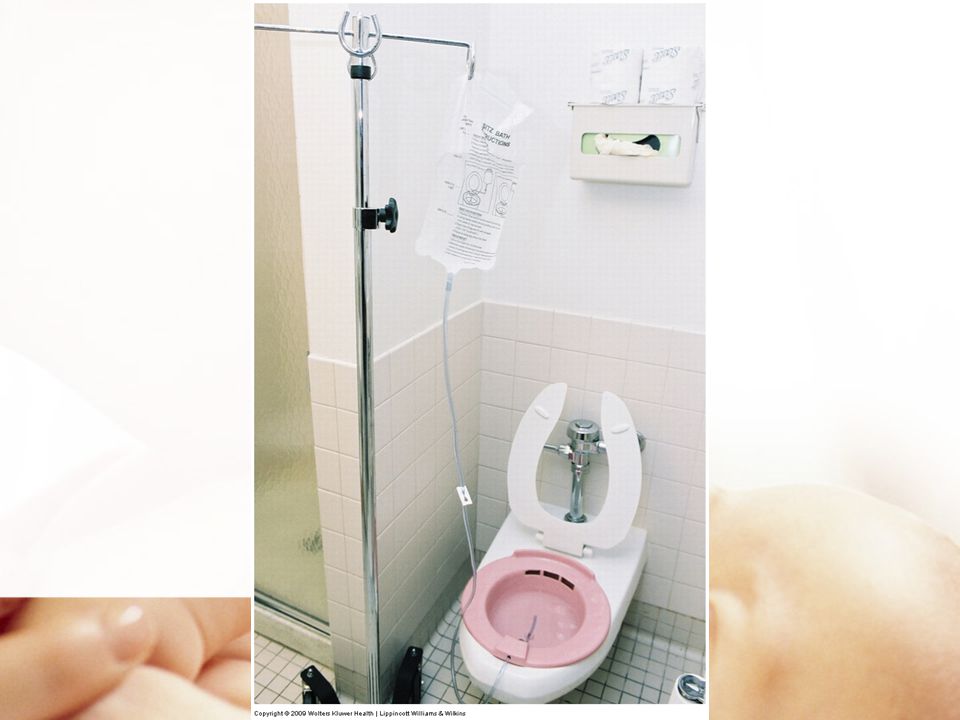
Stool softener- especially 4th degree Laxative Sitz bath for discomfort Medications for hemorrhoids

28
Lochia Rubra Serosa Alba Documentation

29
Lochia Assessment

30
Scant 1-2 in About 10 ml

31
Small 2-4 in About ml

32
Moderate 4-6in About mL

33
Heavy Saturated pad greater than 6 in About mL within 1 hr.

34
Nursing Care Educate on the stages of lochia
Increase in lochia, foul odor or return to Rubra lochia is not normal Change Peri pad frequently Peri care after each voids to decrease risk of infections

35
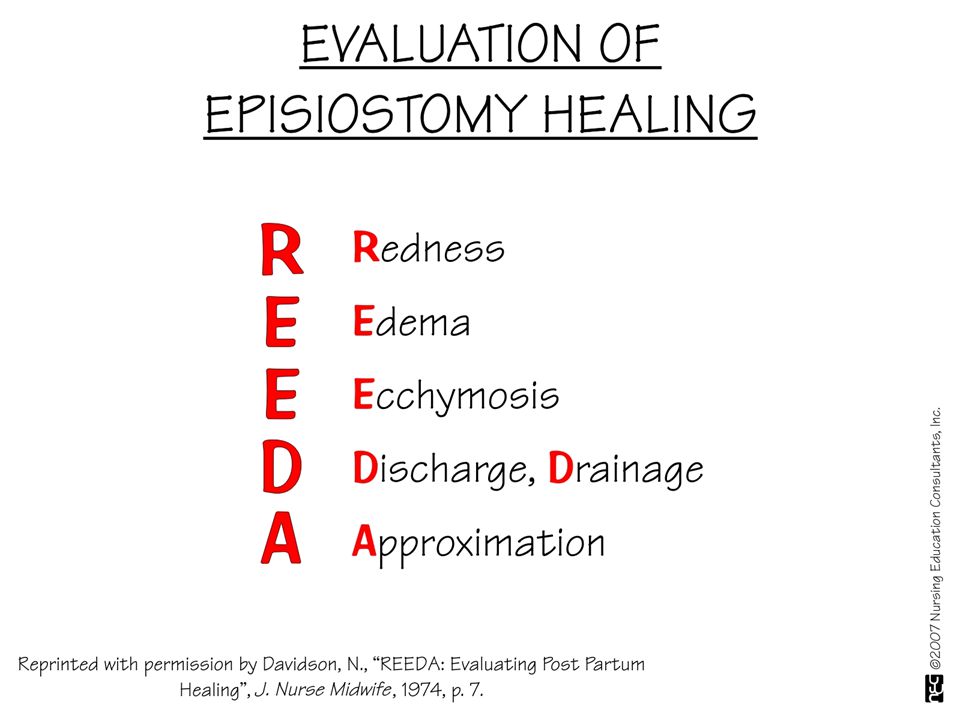
Episiotomy 1-2 inch incision in the muscular area between the vagina and the anus Assess REEDA Lacerations Episiotomy care

38
Nursing Care Peri care Ice packs Dry heat Topical medications
Sitz bath Teaching guidelines 16.1 p. 499

40
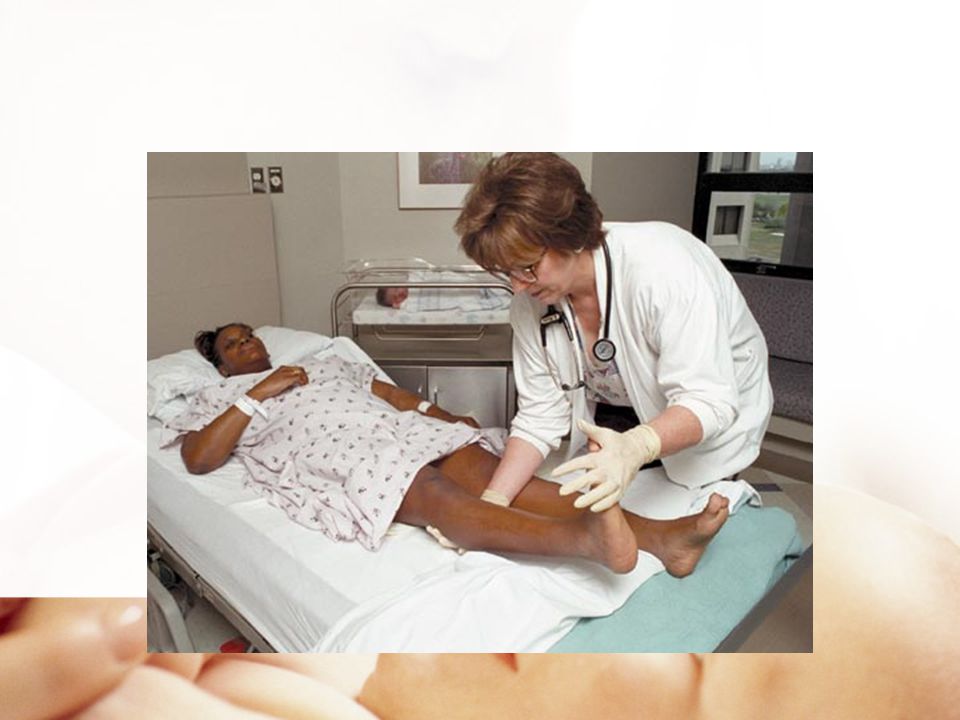
Extremities Increases the risk of thromboembolic disorders
Risk factors venous stasis, altered coagulation and vascular damage due to birth process increase risk of clot formation

41
Assess for Thrombosis Homan’s sign Assess extremities
Monitor for signs of PE

43
Post Partum Assessment
Post Partum Assessment Video

44
Emotional Status Bonding is a vital component of the attachment process. It helps establish parent infant attachment and a healthy loving relationship. Bonding takes during the first 30 to 60 min. after birth

45
Emotional Status Bonding process helps to lay the foundation for nurturing care Touch- skin to skin Eye contact Breastfeeding Engrossment Factors that interrupt bonding

46
Engrossment Seven Behaviors Visual awareness Tactile awareness
Perception NB is perfect Focus is on NB Aware of NB’s distinct features Extreme Elation Increase sense of self esteem- proud

47
Tactile Awareness

48
Bonding Factors that may interfere with bonding process
Stress over finances Lack of support Cultural beliefs Interruption of process-sick child NICU

49
Transitioning to parenthood
Difficult and challenging Provide emotional support Accurate information Nursing goal create a supportive teaching environment

50
Assuming the mothering role
Rubin’s three phases Taking –in Taking –hold Letting-go

51
Taking in Phase

52
Fathers Development Process
Three stages Expectations Reality Transition to Mastery

53
Maternal Physiological Adaptations

54
Hematological System Decrease in blood volume Elevated WBC
Increased Fibrinogen

55
Hormonal Levels Estrogen and Progesterone decrease
Anterior pituitary → prolactin for lactation Expulsion of the placenta- placental lactogen, cortisol, growth hormone, and insulinase levels decrease “Honeymoon phase”- insulin needs decrease

56
Neurological System Maternal fatigue Transient neurological changes
Headaches Carpel tunnel improvement

57
Integumentary System Darken pigmentation gradually fades
Hair regrowth returns to normal in 6-12 months Striae( stretch marks) fade to silvery lines
 fade to silvery lines.")
58
Immune System Rubella Administer to nonimmune mothers
Safe for nursing mothers Avoid pregnancy for 1 month Flu-type symptoms may occur

59
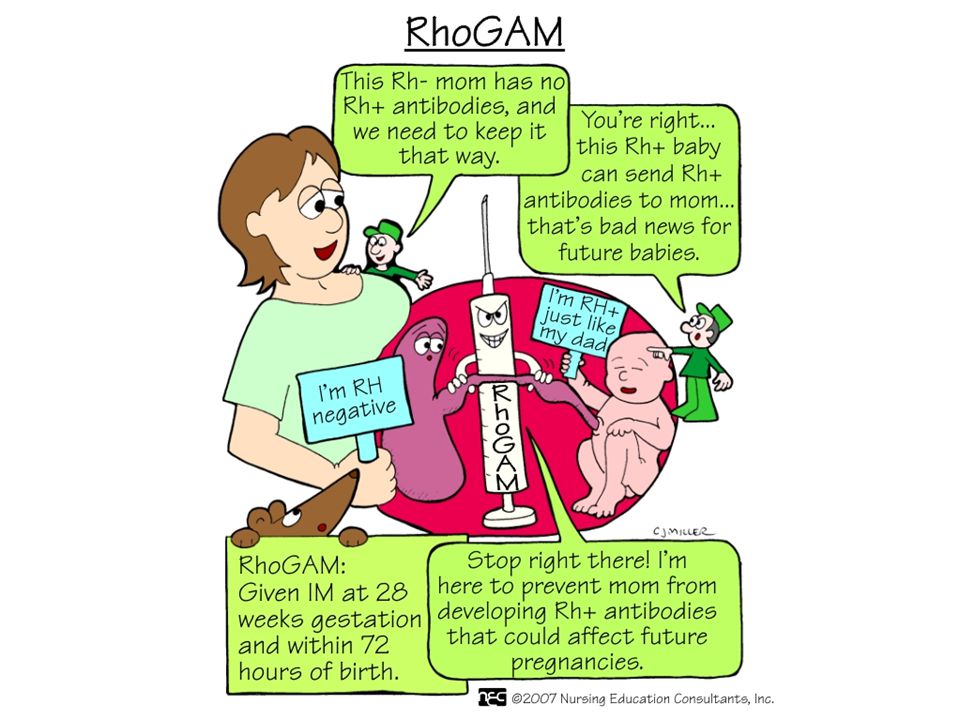
Immune System Rho (D) immune globulin
Mother Rh negative, infant Rh positive Negative coombs’ test 300 mcg of RhoGam within 72 hrs after delivery Card issued to mother

61
Reproductive System Involution of uterus Healing of placental site
Vaginal changes

62
Menstruation and Ovulation
Nonlactatating mother Menstruation returns in 7-9 wks, can take up to 3mo. First cycle may be anovulatory Lactating mother Delayed ovulation and menstruation

63
Musculoskeletal System
Relaxation of pelvic joints, ligaments, and soft tissue Muscle fatigue and general body aches from labor and delivery of newborn Rectus abdominis diastasis

64
Postpartal Surgical Patient
Tubal ligation Cesarean birth

65
Breast Feeding American Academy of Pediatrics (AAP) recommends infants be breastfed exclusively for first 6 months of life Breastfeeding should continue for at least 12 months If infants are weaned before 12 months, they should receive iron-fortified infant formula

66
Breast Feeding Optimal method of feeding infant
Breast milk- Bacteriologically safe, fresh, readily available Milk transition: Colostrum, Transitional milk & mature milk Breastfeeding benefits 18.2 p 583 Nursing Care Plan 18.1 pg 587

67
Contraindications to Breastfeeding
Maternal cancer therapy/ radioactive isotopes Active tuberculosis HIV Maternal herpes simplex lesion Galactosemia in infant Cytomegalovirus (CMV) Maternal substance abuse
 Maternal substance abuse.")
68
Breast Feeding Keys to successful breast-feeding
Initiate first feeding within first hr. No supplements Feed on demand, unrestricted at least 8-12 feeds in 24hrs Avoid artificial nipples Mother and newborn to stay together

69
Breastfeeding Cue signs Latch-on Assess for milk let down
Scoring tool table 18.6 p 509

70
Cue Signs Rooting

71
Latch on Open mouth gape Infant tip of nose, cheeks and chin touching breast

74
Hold nipple in infants mouth to latch & suck
THE LATCH SCORING TOOL Parameters 0 Point 1 Point 2 Point L Sleepy infant No latch achieved Hold nipple in infants mouth to latch & suck Stimulate to suck Latches on rhythmic sucking A: Audible swallow none Few with stimulation Spontaneous and Intermittent T Type of nipple Inverted Flat Protruding C Comfort of nipple Engorged cracked bleeding sever discomfort Filling, reddened, small blisters Mild to mod. discomfort Soft nontender H Positioning Nurse must hold infant to breast Minimal assistance then mother takes over No help needed

75
Breastfeeding Positions Cradle hold Foot ball Side lying

76
Cradle Hold

77
Foot Ball Hold

78
Foot Ball Hold

79
Side Lying

80
Breastfeeding A newborns stomach is the size of a small marble and can hold 5-7 cc’s. This is matches the amount of colostrum produced From 7-10 days it increases to the size of a golf ball and can hold 1.5 to 2 oz

81
Breastfeeding Newborns nurse on average 8-12 times/24hrs
Feed by cue signs about every 1-3 hours Should have no more than one 4 hr period Teaching Guidelines 18.4 pg.588

82
Milk Expression Manually Manual or handheld breast pump
Electric breast pump

83
Hand Express

85
Manual Pump

86
Electric Hand Held

87
Electric Pump

88
Electric Pump

89
Breast Milk Storage Room temperature- 4 hrs Refrigerator- 5-7 days
Deep freezer- 6-7 months

90
Ineffective Breastfeeding
Incorrect latch-on Inverted nipples Breast engorgement

91
Special Considerations
Sleepy baby- use gentle stimulate to bring to alert state Fussy baby- use calming techniques Slow weight gain- evaluate breastfeeding

92
Formula Feeding Formula preparation
Periodically check nipple integrity Bottle preparation Teaching Guidelines 18.5 p. 591

93
Discharge Teaching Fundus and Lochia Episiotomy care Incision care
Signs of PP infection- table 22.3 p 761 Elimination Nutrition Box 16.4 p 504

94
Discharge Teaching Exercise- 16.2 p 501 Activity Pain management
Sexual activity Contraception Blues Community resources

95
Postpartum Women at Risk Chapter 22

97
Postpartum Hemorrhage
Blood loss >500 ml of blood after a vaginal birth 1000 ml of blood after cesarean section Major hemorrhage >2,500 mL Transfusion of >5 units Any amount of bleeding that places mother in hemodynamic jeopardy Table 22.1 pg 748

98
Postpartum Hemorrhage
5 T’s- factors associated with PPH Tone Tissue Trauma Thrombin Traction Table 22.2 pg. 751

99
Tone / Atony Altered muscle tone due to overdistention
Prolonged or rapid labor Infection Anesthesia

100
Tissue Retained placental fragments Uterine inversion Clots
Subinvolution

101
Trauma Cervical lacerations Vaginal lacerations
Hematomas of vulva, vagina or peritoneal areas

103
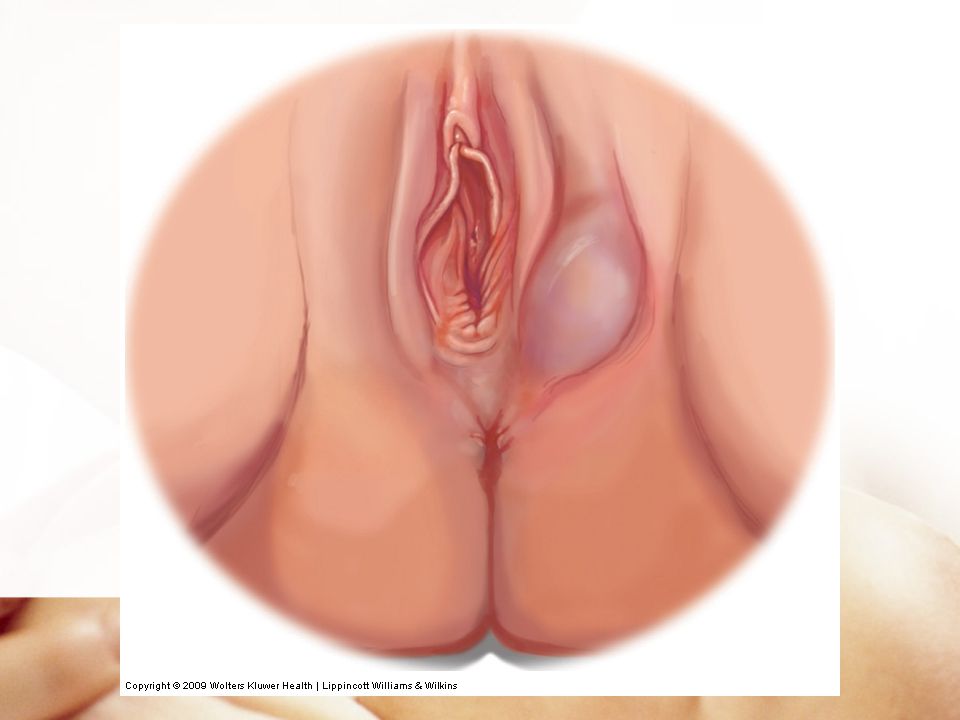
Trauma Hematoma Localized collection of blood in connective or soft tissue under the skin( caused by laceration to blood vessel) Risk factors Signs and symptoms Management

104
Thrombin Disorders of the clotting mechanism
This should be suspected when bleeding persists without an identifiable cause

105
Management of PPH Frequent VS q 15 min times 1 hr. Fundal massage
Administer medications Monitor blood loss for amount Maintain IV Type & cross match Empty bladder

106
Fundal Massaging Procedure 22.1 pg. 753

107
Uterotonic Drugs Oxytocin (Pitocin) Misoprostol (Cytotec)
Dinoprostone (Prostin E2) Methylergonovine maleate (Methergine) Prostaglandin (Hemabate) Drug Guide 22.1 pg.754
 Methylergonovine maleate (Methergine) Prostaglandin (Hemabate) Drug Guide 22.1 pg.754.")
108
Management of PPH Balloon Tamponade Catheter

109
Post Partum Hemorrhage
PPH Simulation PPH Noell

110
Thromboembolic Conditions
Thrombosis (blood Clot) can cause inflammation of the blood vessel (Thrombophlebitis) which can cause Thromboembolism (obstruction of blood vessel)
 can cause inflammation of the blood vessel (Thrombophlebitis) which can cause Thromboembolism (obstruction of blood vessel)")
111
Assessment Superficial
Tenderness and pain in extremity Warm and pinkish red color over thrombus area Palpable- feels bumpy and hard Increased pain when ambulating

112
Nursing Care NSAIDs for pain Bed rest elevate affected leg
Warm compresses Elastic stockings No anticoagulants required

113
Assessment For Deep Vein Thrombosis
Calf swelling Warmth Tenderness Pedal edema Diminished peripheral pulses Color blue Homan’s sign

114
Nursing Care Bed rest Elevate effected leg Continuous moist heat
TED hose both legs Analgesics PRN Anticoagulation therapy

115
Thrombosis Patient Education
Anticoagulation Teaching Guidelines 22.1 pg. 758 Eliminate risk factors Continue using Compression stockings Avoid constrictive clothing & prolonged standing Danger signs

116
Pulmonary Embolism Abrupt onset: chest pain, dyspnea, diaphoresis, syncope, anxiety ABC response

117
Postpartum Infections
Temp of or higher after the first 24 hrs. for 2 successive days of the first 10 PP days Temp of or greater within first 24 hrs.- sever pelvic sepsis Group A or B streptococcus

118
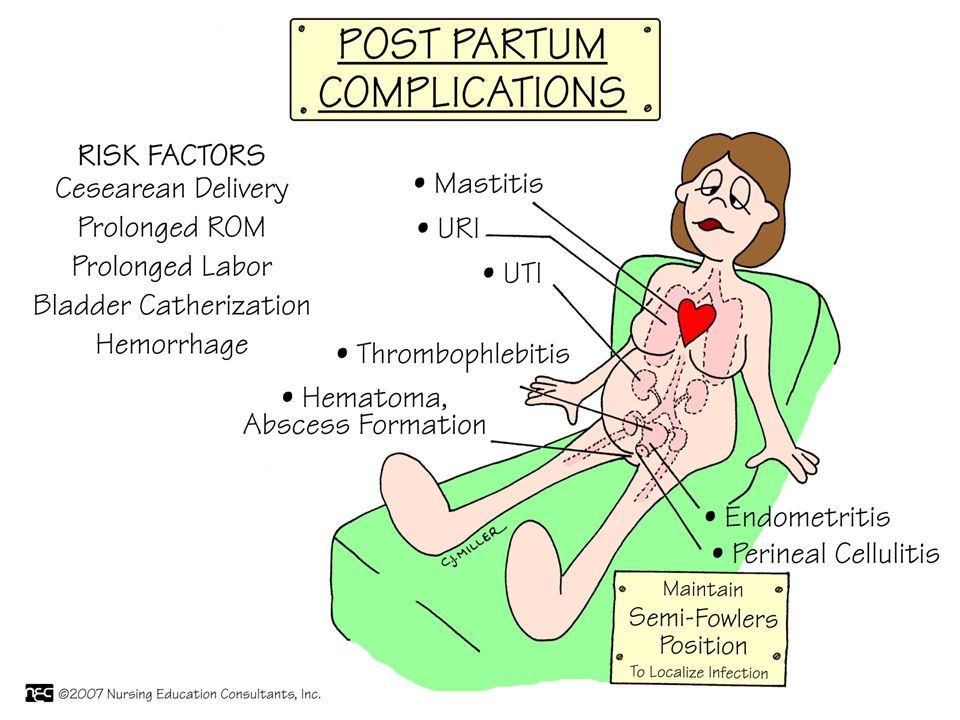
Postpartum Infections
Endometritis Wound infection UTI Mastitis Septic Pelvic Thrombophlebitis Box 22.1 Risk Factors Table pg. 761 signs & symptoms

119
Metritis Involves the endometrium, decidua and adjacent myometrium of the uterus Lower abdominal tenderness or pain Temperature Foul-smelling lochia

120
Nursing Care Administer broad spectrum antibiotic Provide analgesia
Provide emotional support

121
Wound Infection Sites- Cesarean incision, episiotomy and genital tract laceration Drainage Edema Tenderness Separation of wound edges

122
Nursing Care Aseptic wound management Frequent perineal pad changes
Good hand washing Administer antibiotics Analgesics Perineal- Peri care Incision- wound care

123
Urinary Tract Infection
Burning and pain on urination Lower abdominal pain Low grade fever Flank pain Proteinuria, hematuria, bacteriuria, nitrates and WBC

124
Nursing Care Frequent emptying of bladder Increase fluid intake
Antibiotics Analgesics Peri care

125
Mastitis Infection of the breast (one sided)
Seen first 2 weeks after delivery Most common organism staphylococcus aureus Infected nipple fissure - to ductal system involvement- edema obstructs milk flow in a lobe- mastitis

126
Mastitis Symptoms Flu like symptoms
Tender, hot, red area on one breast Breast distention with milk

127
Nursing Management Empty the breast by increasing the frequency of nursing or pumping Control infection- Antibiotics Analgesics Warm/ice compresses Assess infants mouth for thrush

128
Postpartum Infection Education
Continue antibiotics Monitor temperature and notify provider if temp greater then 100.4 Watch for signs and symptoms of a recurrence Practice good hand washing Teaching Guidelines 22.2 pg. 765

129
Postpartum Affective Disorders
Plummeting levels of estrogen and progesterone after delivery contribute to the mood disorders Disorders based on their severity: Postpartum blues Postpartum depression Postpartum psychosis

130
Postpartum Blues Transient periods of depression during the first 1 to 2 weeks postpartum Tearfulness Sad feeling Confusion Insomnia Feel overwhelmed

131
Nursing Care Remind mom that the “Blues” are normal Encourage rest
Utilize relaxation techniques Share her feelings with her partner If symptoms do not resolve and progress to depression medical treatment needs to be sought

132
Postpartum Depression
Gradual onset and is evident within first 6 wks. Cause combination of body, mind, and lifestyle Symptoms- sleep disturbances, guilt, fatigue, feelings of hopelessness Box 22.2 pg. 771 Screening tools

133
Postpartum Depression
Management same as that for major depression Antidepressants Antianxiety Psychotherapy Marriage counseling if that is part of the causes Provide support for the father as well

134
Postpartum Psychosis Emergency psychiatric condition which could put the women at risk for suicide & infanticide Detect within 3 wks. of giving birth Symptoms: delusions, hallucinations, agitation, inability to sleep, bizarre irrational behavior

135
Postpartum Psychosis Management
Usually hospitalized for several months Psychotropic drugs Individual psychotherapy Support group therapy

Similar presentations




















 Contractions: oxytocin; decrease bleeding After pains: associated with multiparas,>")

