Download presentation
Presentation is loading. Please wait.

1
Update in Pain management HIMAA Conference Dr Tony Weaver Clinical Director of Surgical Services Director of Pain Management Clinic Barwon Health

2
Pain Services What we are-- Acute Pain Service – In patient- -run in conjunction with main Anaesthetic Dept. Pain Management Clinic ( Outpatients) – Chronic (Persistent) Non-Cancer pain – Cancer Pain ( with Oncologists & Palliative Care Physicians) Referral by GP’s, Hospital Medical Staff, Private Medical and Surgical Specialists
 – Chronic (Persistent) Non-Cancer pain – Cancer Pain ( with Oncologists & Palliative Care Physicians) Referral by GP’s, Hospital Medical Staff, Private Medical and Surgical Specialists.")
4
Pain is a Bio-Psycho-Social problem So, we must take a Multi- disciplinary Approach – Medical, Psychology, Physiotherapy. Review of diagnosis – M/disc Treatment plan formulated Then, Feed-back session with the patient

5
Pain Patho-physiology Types of Pain Descartes model ( anatomical model ) Physiological pain Clinical Pain( Injury + individual emotional & physiological response) Nociceptive Pain Neuropathic pain Sympathetically maintained pain
 Physiological pain Clinical Pain( Injury + individual emotional & physiological response) Nociceptive Pain Neuropathic pain Sympathetically maintained pain")
6
Pain Concepts Nociceptive Pain Nociceptive Pain - Acute Pain ( also persistent) – Stimulation of peripheral nociceptors, somatic and visceral, relayed to dorsal horn, modulated, and passed to perception centres. – Identifiable cause – Acute post injury, post surgery pain – Arthritic pain – Inflammatory pain – Mechanical pain

7
Pain concepts Neuropathic pain - Characteristics Neuropathic Pain- pain generated from within the nervous system – Spontaneous pain – Burning pain – Stabbing, shooting pain – Dysaesthesiae (ants crawling) – Multi-dermatomal Allodynia, Hyperalgaesia, Hyperpathia.
 – Multi-dermatomal Allodynia, Hyperalgaesia, Hyperpathia.")
8
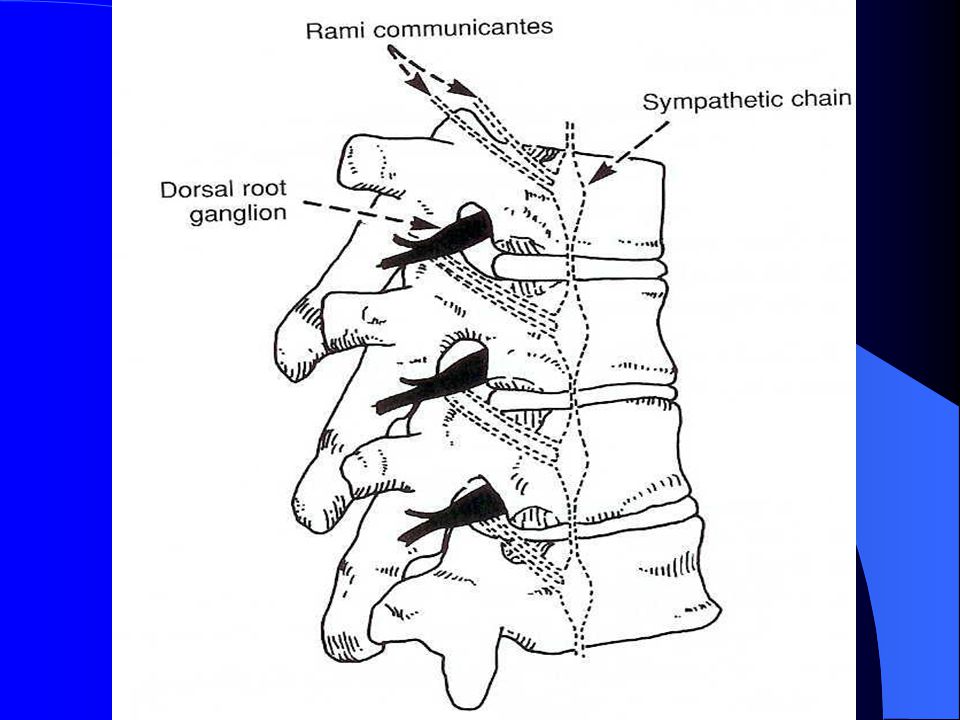
Pain Concepts Sympathetically maintained pain – Peripheral Sympathetic fibre growth – Dorsal root ganglion ingrowth with adrenergic fibres – Manifested by Vasomotor, Sudomotor, Trophic Motor & extra-pyramidal changes – Usually accompanied by Neuropathic pain features

9
CRPS / RSD CRPS was called – Reflex Sympathetic Dystrophy – Causalgia ( kausis=burn, algos=pain) – Algodystrophy – Sudek’s atrophy – Peripheral acute trophoneurosis – Traumatic angiospasm – Post infarction sclerodactyly
 – Algodystrophy – Sudek’s atrophy – Peripheral acute trophoneurosis – Traumatic angiospasm – Post infarction sclerodactyly")
10
Pain Syndromes CRPS Type 1 and Type 2 ( post nerve injury) ( Old terminology RSD and Causalgia) Clinical presentation: – Neuropathic pain i.e. burning,shooting, multi dermatomal – Allodynia, Hyperalgaesia, Hyperpathia – Sudomotor, vasomotor, trophic tissue change, osteopaenia – Motor & extra-pyramidal changes

11
Target Treatment strategies Medical – Pharmacological – Interventional Psychology – Cognitive Behavioural Therapies Individual & Groups Physiotherapy – Always active exercises, restoration of function

12
Cognitive Behavioural Therapy Psychology, Physiotherapy, Medical Individual and Groups IMPACT and MG group work – Certainly Interventional – Re- engineering of Beliefs – Re-establishment of Self -Efficacy – Restoration of Function both Physically and Socially – Sustainable gains – 3 weeks full time + follow-up

13
Chronic, Persistent Pain. Cancer Pain Cancer Pain – ~ 95 % managed with chemo/ radio therapy and ‘conventional’ analgaesics including Opioids, nsaid’s, Steroids, Adjuvant agents, Tramadol,Lignocaine, Ketamine. Advanced management – includes specific nerve blocks e.g. splanchnic,(coeliac) paraverterbral. – Intraspinal: Epidural and Intrathecal drug Rx
 paraverterbral. – Intraspinal: Epidural and Intrathecal drug Rx.")
14
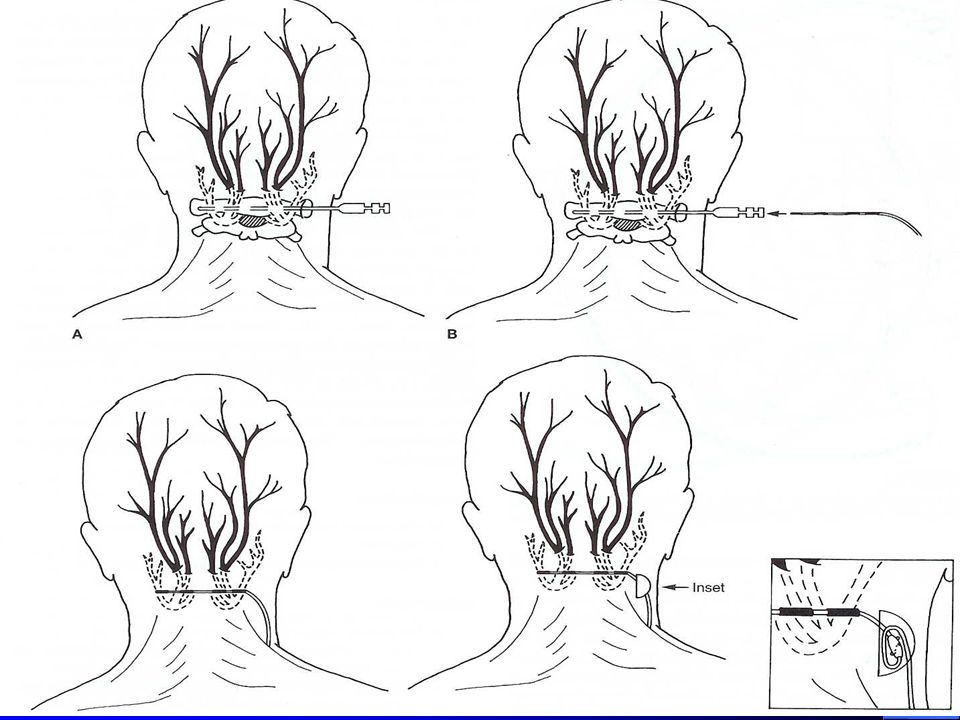
Interventional Therapies Specific nerve and plexus targets Peripheral & Cranial nerve blocks Radiofrequency lesioning – Continuous and Pulsed current – Somatic afferents from facet joints ( Medial Branch of Post.Primary Rami.) – Dorsal root ganglia, sympathetic ganglia. Cryotherapy

15
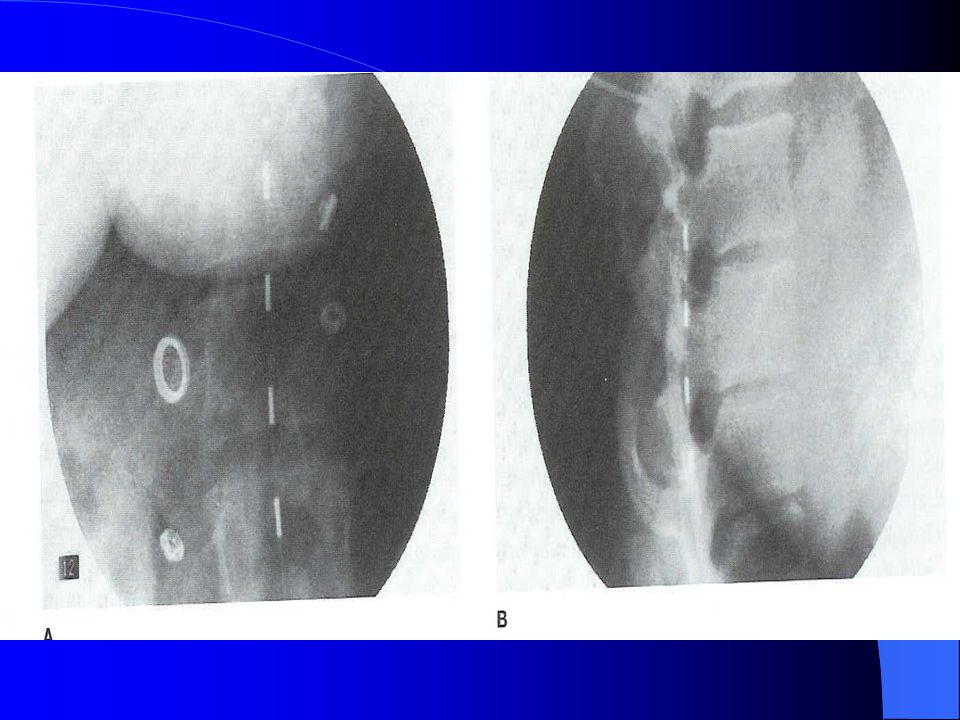
Interventional Therapies Chronic non-cancer Pain Epidurals: cervical, thoracic, lumbar, caudal Nerve root sleeve injections Sacro-iliac joints L.A. & Steroids Epidurolysis : lysis of fibrotic tissue in epidural space

20
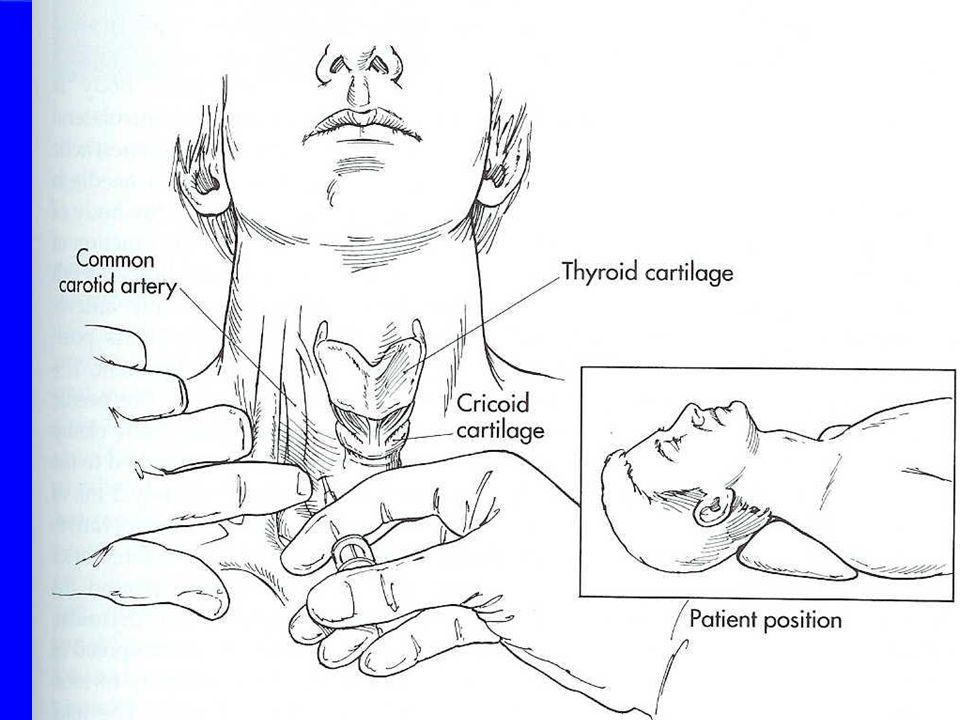
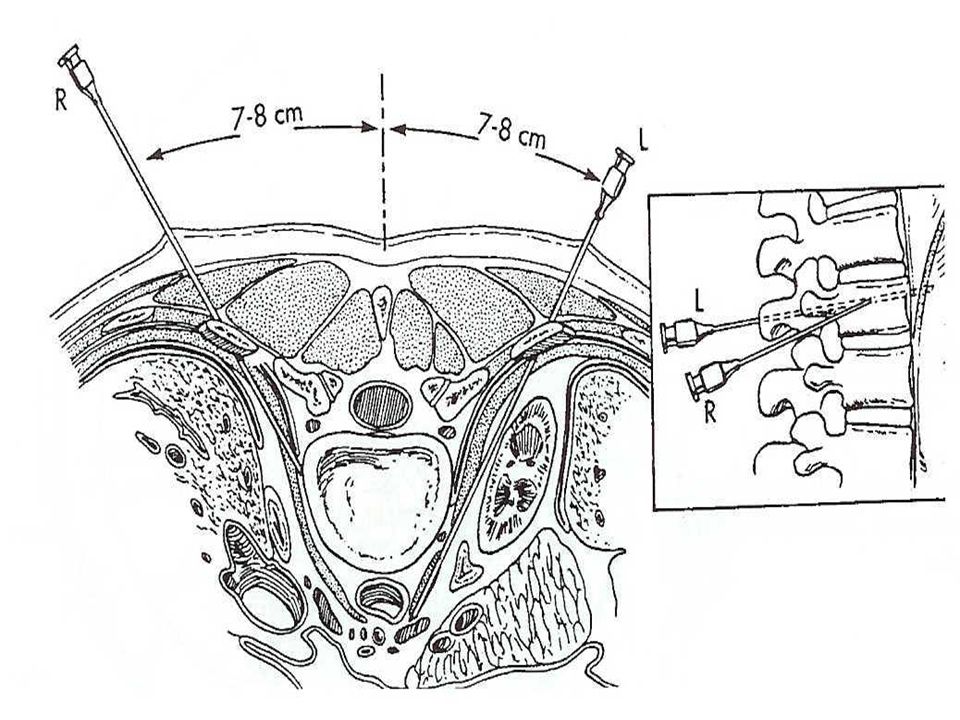
Interventional Therapies Specific nerve and plexus targets Sympathetic Nerve blocks – Stellate – Thoracic – Lumbar L.A – Coeliac Neurolytic – Splanchnic R.F. – Hypogastric – Ganglion impar

26
Chronic - non-Cancer Pain Intraspinal Therapies Discovery of receptors in Spinal cord for – Opioids – Adrenergic alpha agonists – Alpha 2 agonists ( Clonidine) – Serotonergic – GABA
 – Serotonergic – GABA")
27
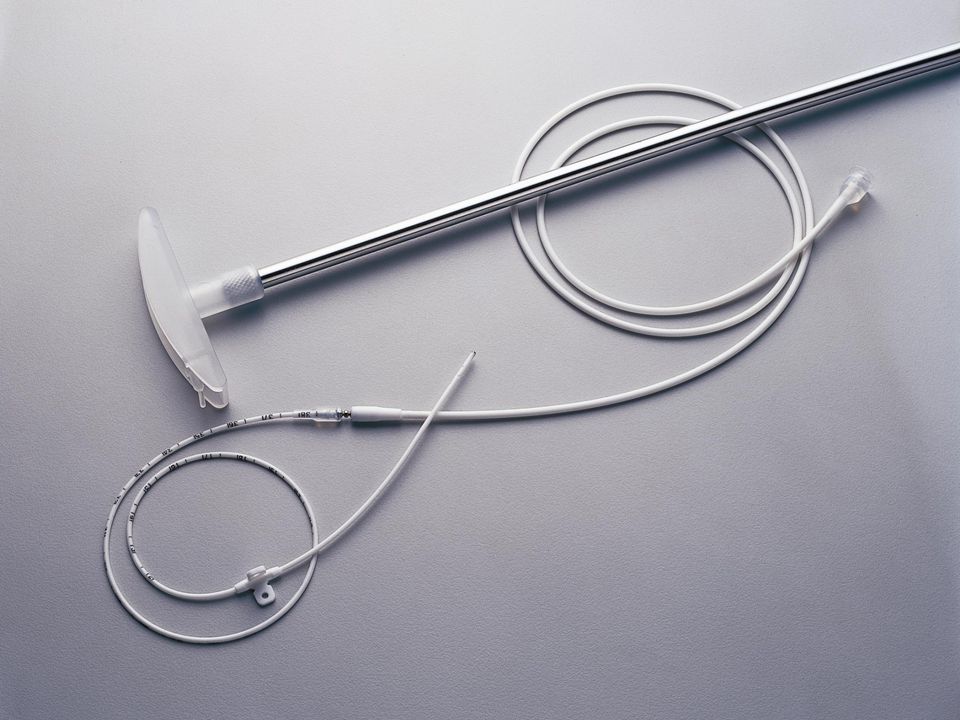
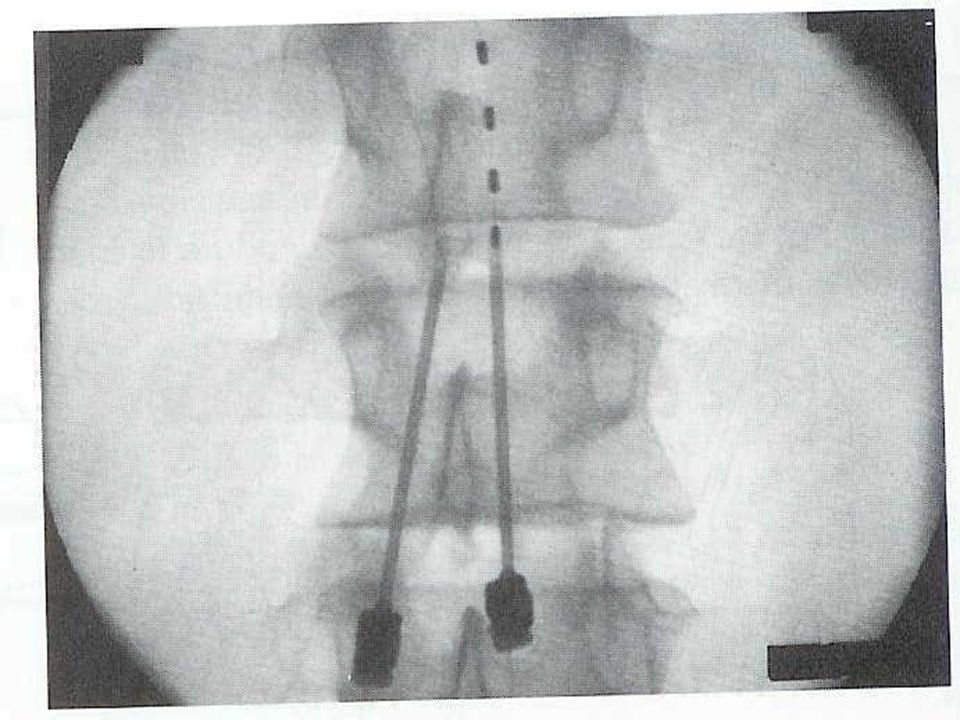
Chronic - non-Cancer Pain Intraspinal Therapies Portals – Epidural and Intrathecal catheters. Implanted Pumps & Intrathecal catheter Allows 10- 100 times decrease in dose c.f. systemic delivery with increased efficacy and marked decrease in side effects.

28
Spinal column Stimulation/ Intrathecal pumps SCS potentially good in CAREFULLY SELECTED patients for Neuropathic pain problems. ( Failed Back, CRPS Type 1 & 2,) Intrathecal pumps potentially useful for - nociceptive pain states lower body spasticity cancer pain with reasonable prognosis
 Intrathecal pumps potentially useful for - nociceptive pain states lower body spasticity cancer pain with reasonable prognosis.")
34
Chronic - non-Cancer Pain Intraspinal therapies Spinal Cord Stimulation – Relies on the “Gate theory” principle – continuous non-noxious stimuli via A beta fibres inhibit nociceptive traffic in dorsal horn & cord.

Similar presentations














 Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio)>")












