Download presentation
Presentation is loading. Please wait.

2
Prevention of a “Broken Heart”

3
February 16 2005 Mario L Maiese DO FACC FACOI Associate Professor UMDNJSOM South Jersey Heart Group www.sjhg.org Email @ maiese1@comcast.netmaiese1@comcast.net

7
Patients with one manifestation often have coexistent disease in other vascular beds Coronary Artery Disease Cerebrovascular Disease Peripheral Arterial Disease 6% 16%40% 11%3% 15% 9% 38% overlap ( 2 vascular beds) Hidden Overlap of Atherothrombotic Disease Ness J, Aronow WS. JAGS. 1999;47(10):1255-56. Ness J, Aronow WS. JAGS. 1999;47(10):1255-56.
: Ness J, Aronow WS. JAGS. 1999;47(10):")
8
Dyslipidemia: Identify high-risk patients and determine benefits of treatment. Strategy and recommendations for obtaining safe optimal aggressive treatment goals.

10
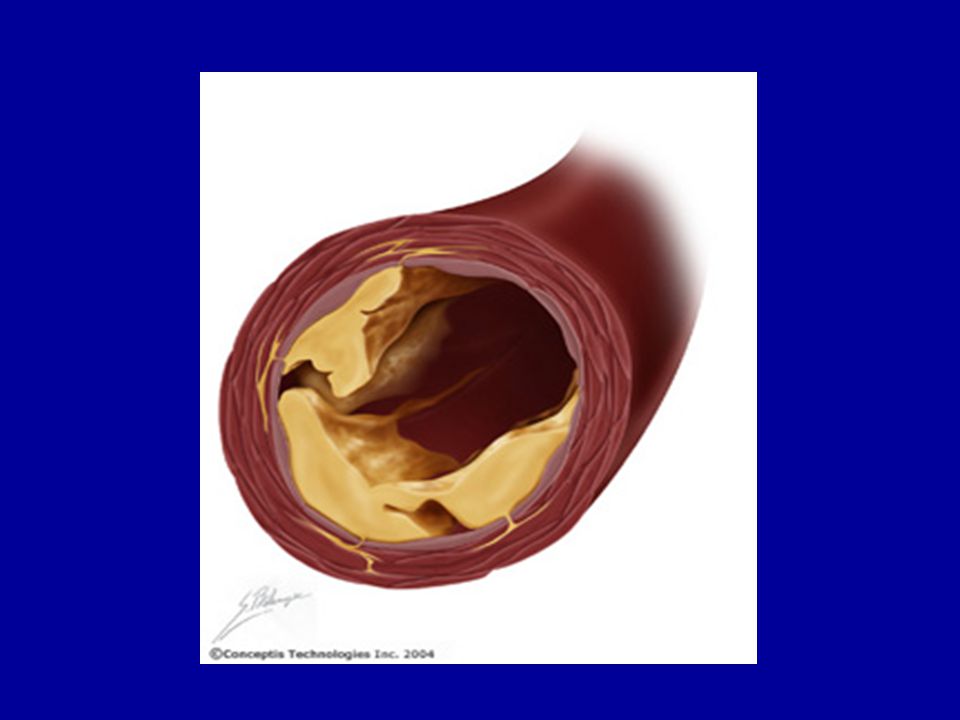
Normal Fatty Streak Fibrous Plaque Occlusive Atherosclerotic Plaque Occlusive Atherosclerotic Plaque Plaque Rupture/ Fissure & Thrombosis MI Stroke Critical Leg Ischemia Clinically Silent Coronary Death Coronary Death Increasing Age Effort Angina Claudication Unstable Angina Unstable Angina Atherothrombosis: A Progressive Process Courtesy of P Ganz.

11
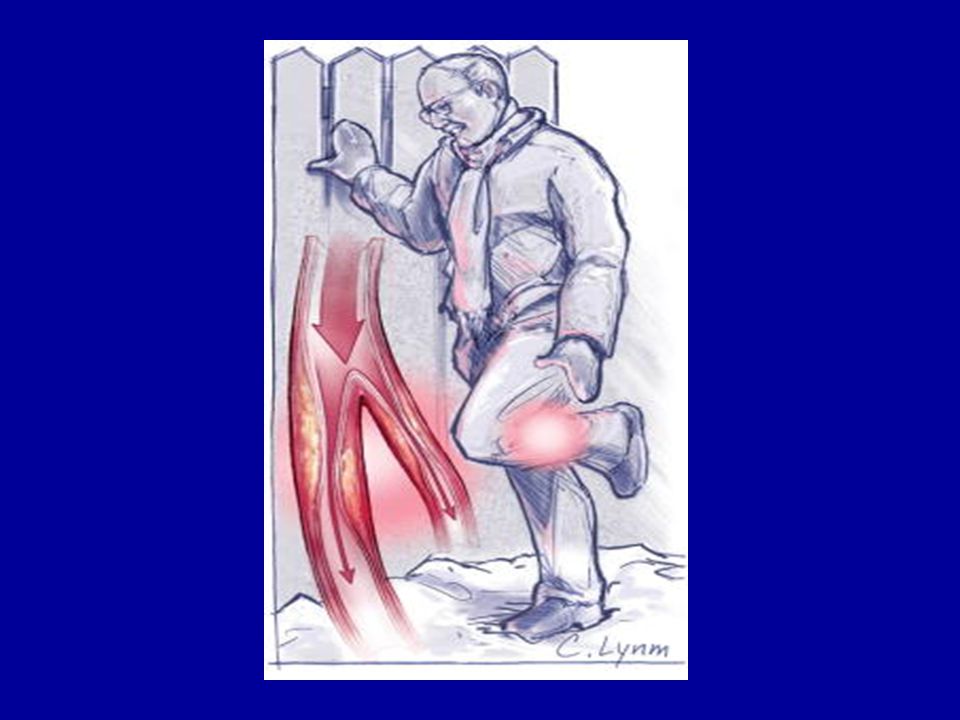
Thrombotic occlusion Final Result Normalblush

12
“To a man with a hammer every nail looks like it needs driving”. …Mark Twain

14
“If prevention is your goal focus on the donut, not the hole”.

15
Lesion growth

16
Mechanism of Plaque Disruption in Atherothrombosis

17
It is this "hidden disease" – the presence of vulnerable plaques throughout the coronary tree – that is the target of long-term treatment with high-dose statins, aspirin, ACE inhibitors.

18
ABCs of CVD Risk Management CVD=cardiovascular disease; ACE=angiotensin converting enzyme; ARB=angiotensin receptor blocker; BP=blood pressure; EF=ejection fraction; MI=myocardial infarction. Braunstein JB et al. Cardiol Rev. 2001;9:96-105. InterventionGoals A Antiplatelets/anticoagulants ACE inhibitors/ARBs Antianginals ( -blockers) Treat all high-risk patients with one or both of these (ASA, clopidogrel) Optimize BP especially if CVD, type 2 diabetes, or low EF present Relieve anginal symptoms, allow patient to exercise B BP control Aim for BP <130/85 mm Hg, or <130/80 mm Hg for type 2 diabetes Post MI or low EF
 Treat all high-risk patients with one or both of these (ASA, clopidogrel) Optimize BP especially if CVD, type 2 diabetes, or low EF present Relieve anginal symptoms, allow patient to exercise B BP control Aim for BP <130/85 mm Hg, or <130/80 mm Hg for type 2 diabetes Post MI or low EF.")
19
ABCs of CVD Risk Management Braunstein JB et al. Cardiol Rev. 2001;9:96-105. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497. * Circulation July 13 2004; 110: 227-239. InterventionGoals CCholesterol Management* LDL-C targets, ATP III guidelines – CHD, CHD risk equivalents: <100 mg/dL* – 2 RF: <130 mg/dL* – 0-1 RF: <160 mg/dL Cigarette-smoking cessation HDL-C: 40 mg/dL (men) 50 mg/dL (women) TG: <150 mg/dL Long-term smoking cessation
 50 mg/dL (women) TG: <150 mg/dL Long-term smoking cessation.")
20
ABCs of CVD Risk Management BMI=body mass index; HbA 1c =glycosylated hemoglobin; CAD=coronary artery disease. Braunstein JB et al. Cardiol Rev. 2001;9:96-105. *JAMA Nov 2004;2442-2490. InterventionGoals DDietary/weight counseling Diabetes management Achieve optimal BMI saturated fats; fruits, vegetables, fiber (South Beach)* Achieve HbA 1c <7% EExercise Education of patients and families Improve physical fitness (aim for 30 min/d on most days per week) Optimize awareness of CAD risk factors
* Achieve HbA 1c <7% EExercise Education of patients and families Improve physical fitness (aim for 30 min/d on most days per week) Optimize awareness of CAD risk factors.")
21
Cholesterol Management …per NCEP III Guidelines PRIMARY GOAL: LDL-C SECONDARY GOAL: Non HDL-C JAMA 2001; 285: 2486-2497.

22
Non-HDL-C Provides a measure of all the cholesterol in atherogenic particles including LDL-C, Apo B, LP(a) and TG-rich particles in VLDL,VLDL remnants and intermediately dense lipoproteins. Introduced as the secondary target of therapy in patients with high TG (> 200mg/dL) per NCEP ATP III. JAMA 2001; 285: 2486-2497.
 per NCEP ATP III. JAMA 2001; 285:")
23
NCEP III Non HDL-C Goal Non-HDL-C = TC - HDL-C Goal Non-HDL-C is 30mg > LDL-C goal Must be remembered that LDL-C and non HDL-C goals are surrogates for the number 1 lipid risk factor which is Apo B (a marker of atherogenic lipoproteins).
.")
25
Modifications to NCEP III TLC was re-emphasized. Use of the Framingham CAD risk calculator was recommended. Circulation July 13 2004; 110: 227-239

26
Coronary Artery Disease Calculator

27
Modifications to NCEP III Risk CategoryLDL-C Goal High Risk: CHD,PAD, Carotid vasc. Dx, AAA or CHD risk equivalents (DM or 10-yr CHD risk > 20%) < 100mg/dL. Very High Risk: Above plus having multiple risk factors including DM, tobacco dependence, MetS,or severe or poorly controlled risk factors (eg HBP or recent MI, ACS or recurrent symptoms on Tx. Optional goal < 70mg/dL. Moderate Risk: Two or more risk factors (10- yr risk < 10%). < 130mg/dL. High Moderate Risk: Two or more risk factors (10-yr risk > 10%). Circulation July 13 2004; 110: 227-239. < 100mg/dL.
 < 100mg/dL. Very High Risk: Above plus having multiple risk factors including DM, tobacco dependence, MetS,or severe or poorly controlled risk factors (eg HBP or recent MI, ACS or recurrent symptoms on Tx. Optional goal < 70mg/dL. Moderate Risk: Two or more risk factors (10- yr risk < 10%). < 130mg/dL. High Moderate Risk: Two or more risk factors (10-yr risk > 10%). Circulation July ; 110: < 100mg/dL..")
29
HPS: Heart Protection Study. Lancet 2002; 360: 7-22 Simvastatin 40mg vs placebo 20,536 subjects, 5 years, 30% reduction LDL-C, significant reduction of CV events. Even with starting LDL-C < 100 PROSPER: Prospective Study of provastatin in the elderly at risk. Lancet 2002; 360:1623-30. Provastatin 40mg vs placebo 5,804 subjects, 3.2 years, 27% decrease in LDL-C, significant reduction of CV events. ALLHAT: Anti-hypertensive and lipid-lowering treatment to prevent heart attack trial. JAMA 2002; 288: 2998-3007. Provastatin vs usual care 10,355 subjects, No significant difference. ASCOT-LLA: Anglo- Scandinavian cardiac outcomes trial lipid lowering arm. Lancet 2003; 361: 1149-1158 Atorvastatin 10 mg vs placebo 10,305 hypertensive subjects, 29% decrease in LDL-C, terminated early because of a significant reduction in CV events. NCEP III Update Based on 5 Clinical Trials Trial Name Statin TherapySummary

30
JAMA 2001; 285: 2486-2497.

32
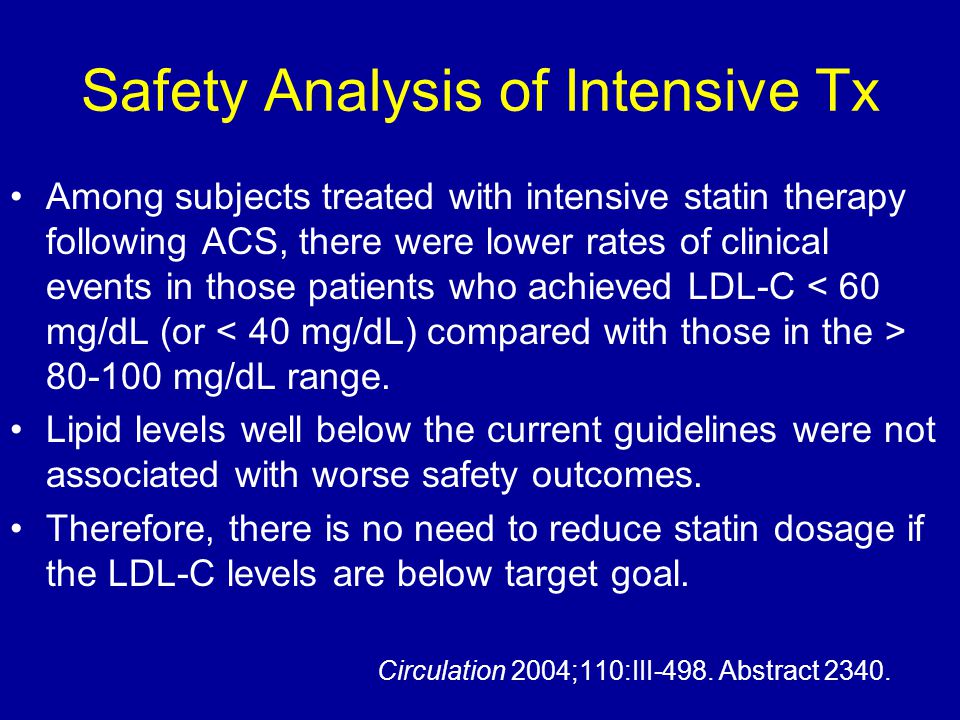
Safety Analysis of Intensive Tx Among subjects treated with intensive statin therapy following ACS, there were lower rates of clinical events in those patients who achieved LDL-C 80-100 mg/dL range. Lipid levels well below the current guidelines were not associated with worse safety outcomes. Therefore, there is no need to reduce statin dosage if the LDL-C levels are below target goal. Circulation 2004;110:III-498. Abstract 2340.

33
“Very High Risk” Patients The updated NCEP III definition of “high risk” requires established CVD plus: Multiple risk factors (especially diabetes). Severe and poorly controlled risk factors (especially continued cigarette smoking). Multiple risk factors for MetS (especially high TG >200 plus non HDL-C > 130mg/dL with low HDL-C [< 40mg/dL]). Patients with ACS.
. Multiple risk factors for MetS (especially high TG >200 plus non HDL-C > 130mg/dL with low HDL-C [< 40mg/dL]). Patients with ACS..")
34
The Forgotten Cardiac Risk Factor: Noncompliance With Lipid- Lowering Therapy Before NCEP ATP III Update. Will be even more difficult reaching LDL-C goals post update.

36
The CARDS data strongly demonstrateas the safety and benefits of statin therapy in T2DM regardless of baseline LDL-C. Conclusion:

39
Comparative Efficacy of Available Statins Available Statins % LDL-C reduction Rosuvastatin 5mg Atorvastatin 10mg 33-39% Simvastatin 20mg Lovastatin 40mg Pravastatin 40mg Fluvastatin 80mg Roberts WC. Am J Cardiol. 1997; 80: 106-107. Stein E et al. J Cardiovasc Pharmacol Therapeut. 1997; 2: 7-16.

40
Even with optimal statin treatment: ----30- 40% reduction in CV events with statins. “There is 50% to 60% risk we’re not addressing”.

41
Preliminary data suggests that combination therapy is much more efficacious in ↓ CV events (> 75%) - not surprising given that the lipid lowering effect is much greater.
 - not surprising given that the lipid lowering effect is much greater.")
42
Be aggressive with combination therapies. In insulin resistant patients with abnormalities of the TG/HDL-C axis statin/Zetia/TriCor would solve the overwhelming majority of lipoprotein abnormalities seen in most patients (getting to LDL-C and non-HDL- C goals (apoB surrogate markers).
..")
45
Efficacy of HDL-C Increasing Compounds Fibrates reduce major coronary events and increase HDL-C without significant toxicity. Niacin has a more potent effect on HDL-C levels, but data on CV event reduction are limited. HDL-C will probably be the “next target” over the next 10 years. J Am Coll Cardiol January 18 2005; 45: 185-197.

46
AFREGS: Armed Forces Regression Study A combination of 3 drugs aimed at increasing HDL-C (niacin, fibrates and cholestyramine): Improves cholesterol profiles. Helps halt angiographic progression of coronary stenosis. May help prevent CV events. Ann Intern Med January 18 2005; 142: 95-104.

49
Adverse Effects of Statins Myalgias (muscle pains), which is seen in 2% to 4% of patients. Myopathy (10x NL CPK) including rhabdomyolysis (> 10,000 CPK) is very rare: Incidence =0.5-1 in 10,000 patients. Increased values in liver function tests (LFTs) in ~ 1% of patients, significant elevations > than 3x NL up to 2% or 2.5% with the highest doses of statins.
 including rhabdomyolysis (> 10,000 CPK) is very rare: Incidence =0.5-1 in 10,000 patients. Increased values in liver function tests (LFTs) in ~ 1% of patients, significant elevations > than 3x NL up to 2% or 2.5% with the highest doses of statins..")
50
Adverse Effects of Therapy Risk usually increases with dose escalation. Risk is higher in women, older age (> 60), dehydration or those with underlying renal or liver disease. Risk increases with combination therapy. Risk is not directly proportional to cholesterol- lowering efficacy.
, dehydration or those with underlying renal or liver disease. Risk increases with combination therapy. Risk is not directly proportional to cholesterol- lowering efficacy..")
51
Management Listen to the patient first (muscle pain weakness or stiffness). Negative placebo situation Balance Positive placebo effect Temporarily stop, reduce the dose or switch (every other day dosing is frequently as effective with reduced side effcts).
..")
52
Take Home Points In nearly all cases increased LFTs and myopathy are reversed after discontinuation of the statin or fibrate. Fenofibrate (Tricor) is safe in combination with all statins (though more expensive). Gemfibrozil (Lopid) in combo increases statin levels and possibly CPK levels and muscle symptoms with all statins except fluvastatin and minimally with pravastatin. Niacin in combination with statins appears to have a much lower risk of myopathy.
 is safe in combination with all statins (though more expensive). Gemfibrozil (Lopid) in combo increases statin levels and possibly CPK levels and muscle symptoms with all statins except fluvastatin and minimally with pravastatin. Niacin in combination with statins appears to have a much lower risk of myopathy..")
53
Clinical concerns (side effects, cost and tolerability) must always be balanced in each individual case with benefit.
 must always be balanced in each individual case with benefit.")
55
Assess and Identify Risk

57
“Are you done with that?”

58
STELLAR trial, Rosuvastatin (Crestor) blew away all the other statins in its ability to reduce the atherogenic lipoproteins so prevalent in metabolic syndrome patients. (Am J Cardiol 2005;95:360–366)
.")
60
Clinical Application of hs-CRP for Cardiovascular Risk Prediction 1 mg/L 3 mg/L 10 mg/L LowRisk Moderate Risk Risk HighRisk Acute Phase Response Ignore Value, Repeat Test in 2 weeks >100 mg/L Adapted from Pearson TA, et al. AHA-CDC Scientific Statement. Circulation. 2003;107:499-511. hs-CRP (Cardio) Level hs-CRP (Cardio) Level Risk Category Risk Category
 Level hs-CRP (Cardio) Level Risk Category Risk Category.")
61
PROVE-IT proves it for inflammation Table 1. Age-adjusted Event Rates According to LDL and CRP Level Achieved with Statin Therapy. Individually Together LDL-C > 704.0LDL-C >70, CRP >24.6 LDL-C < 702.7LDL-C 23.1 CRP > 23.9LDL-C >70, CRP < 23.2 CRP < 22.8LDL-C < 70, CRP < 22.4 N Engl J Med January 6 2005; 352: 20-28.

63
TLC

65
The Problem: “Will power only lasts 3 weeks and in addition it is alcohol soluble.” ….Don’t have a pill for diet & exercise.

66
Medical Treatment (Based on the Guidelines) is determined by risk LDL-C goals: Usually statins first Non- HDL-C goals: Will usually necessitate combination tx [fenofibrate &/or ezetimibe – preferred]
![Medical Treatment (Based on the Guidelines) is determined by risk LDL-C goals: Usually statins first Non- HDL-C goals: Will usually necessitate combination tx [fenofibrate &/or ezetimibe – preferred]](http://images.slideplayer.com/20/5981787/slides/slide_66.jpg "Medical Treatment (Based on the Guidelines) is determined by risk LDL-C goals: Usually statins first Non- HDL-C goals: Will usually necessitate combination tx [fenofibrate &/or ezetimibe – preferred]")
67
STATINS

68
COMBINATION THERAPY

69
GEMS NCEP states that when Non HDL-C is not achieved on lifestyle and a statin, that is when the benefit outweighs any risk of adding a fibrate or niacin of the statin. Combinations of statins, ezetimibe and fibrates (fenofibrate) seems to be the best.
 seems to be the best..")
70
CONCLUSIONS

71
“Preventing a Broken Heart” …The time is now!

72
Sample Case 1 Male, age 62. Original Lipid Panel as of 9/2004: TC = 210, HDL-C = 25, LDL-C = 124. TG = 307 Non HDL-C = 210 - 25 = 185 Lipid Panel as of 1/2005: on TriCor 145 mg and Lipitor 20mg TC = 148, HDL-C = 23, LDL-C = 67, TG = 291 Non HDL-C = 125 Access Risk: “Setting” CHD Risk calculation Goals of therapy: (Based on NCEP ATP III updated) LDL-C Non-HDL-C Treatment: TLC Meds
 LDL-C Non-HDL-C Treatment: TLC Meds.")
73
No preventive cardiologist or lipidologist can make accurate assessments of RISK without clinical details, including history and physical examination. Docs too often loose tract of the essential fact that every bit of advice we offer patients will depend on the risk of that patient.

74
Sample Case 2 Friend of mine: (1995), TC 272, TG 39, HDL-C 93, LDL-C 171. Female now age 45 with - FH no other risk factors, quite fit. Chest CT for Calcium = 0. Now: TC 335, TG 172, LDL-C 202, HDL-C 116. Non HDL-C = 335 - 116 = 219 EBT Calcium score still is 0. Hs-CRP 0.9, LP(a) 70. What is the plan? What does NCEP III recommend?
 70. What is the plan. What does NCEP III recommend .")
75
Sample Case 3. TC = 364 Triglycerides = 219 HDL-C = 39 VLDL -C (calculated) = 44 LDL-C = 281 Non HDL-C = 364 - 39 = 325 What do you want to know?
 = 44 LDL-C = 281 Non HDL-C = = 325 What do you want to know .")
76
Tx Plan for Case 3 1) TLC: Mediterranean or South Beach diet and > 30 - 60 minutes aerobics daily. Take a treadmill exercise test before starting serious exercise. 2) Crestor 20 mg daily along with Zetia 10 mg daily. 3) Wait two weeks, recheck lipids and if Non HDL-C still abnormal start TriCor 160 mg daily. 3) Daily ASA (81mg). 4) Daily omega-3 FA supplement (Coromega, etc): Also have option to push omega-3 FA to higher doses (3-6 gm) to help with the TG, will also increase HDL-C. 5) Must have a BP < 130/85 If up use an ACEI or ARB. 6) If obese and will not exercise, start metformin and titrate to 2 gms daily.
 Crestor 20 mg daily along with Zetia 10 mg daily. 3) Wait two weeks, recheck lipids and if Non HDL-C still abnormal start TriCor 160 mg daily. 3) Daily ASA (81mg). 4) Daily omega-3 FA supplement (Coromega, etc): Also have option to push omega-3 FA to higher doses (3-6 gm) to help with the TG, will also increase HDL-C. 5) Must have a BP < 130/85 If up use an ACEI or ARB. 6) If obese and will not exercise, start metformin and titrate to 2 gms daily..")
77
Cure all Med

79
Survival of the Fittest More than 150 years after Darwin’s published theory of evolution… Evidence continues to mount. There is a direct relationship of survival to physical fitness. Myers J et al. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 2002; 346: 793-801.

80
Exercise

81
Photo Album by Mario L Maiese

96
Relationship Between LDL-C and HDL-C Levels & Coronary Risk

Similar presentations
































>")









” 2004 Focus = multiple risk factor assessment.>")


 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")

![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")


