Download presentation
Presentation is loading. Please wait.

2
THE RHYTHM IN LIFE THE SEASONS DO NOT PUSH ONE ANOTHER; NEITHER DO CLOUDS RACE THE WIND ACROSS THE SKY. ALL THINGS HAPPEN IN THEIR OWN GOOD TIME.

4
Chronic AF in patients with Mitral Valve Disease Its prevalence might reach up to 75%. An important marker of more advanced cardiovascular disease. The onset of AF is now considered a relative indication for mitral valve surgery. Persistence of postoperative AF is linked to increased mortality & morbidity Surgical correction of the valve rarely eliminates the arrhythmia.

5
Surgical treatment of atrial fibrillation – Left atrial isolation procedure – Corridor procedure – Cox- Maze procedure – The radial approach – Mini- Maze procedures

6
Since the Cox- maze III procedure showed that AF can be definitely eradicated, efforts were made to achieve alternative & particularly less complex methods using surgical catheter ablation techniques during cardiac surgery.

7
Rationale for RF ablation Based on the hypothesis that the pulmonary veins and surrounding areas frequently house focal triggers and re- entrant circuits critical to the genesis and perpetuation of AF, it was postulated that circumferential isolation of pulmonary veins eliminates or isolates the arrhythmogenic activity that perpetuates chronic AF within the pulmonary veins

8
An ideal lesion pattern should combine: Slight invasiveness Simplicity High reproducibility Saving of time With excellent success rate. Radiofrequency ablation techniques must guarantee lesion transmularity & continuity without cardiac tissue injury.

10
The purpose of this study is to assess the feasibility, safety, &efficacy of circumferential isolation of each pulmonary vein using endocardial radiofrequency pulses to restore stable sinus rhythm during mitral valve surgery. Also, to identify the clinical predictors to sinus rhythm restoration and left atrial mechanical contraction in this group of patients.

12
This is a prospective randomized controlled study. It had been conducted on sixty patients known to have rheumatic mitral valve disease and chronic atrial fibrillation, referred to the National Heart Institute, for mitral valve surgery between November 2001 and November 2004. They were divided into two groups according to being subjected to surgical ablation of chronic atrial fibrillation using radiofrequency energy in addition to the mitral valve surgery. This is a prospective randomized controlled study. It had been conducted on sixty patients known to have rheumatic mitral valve disease and chronic atrial fibrillation, referred to the National Heart Institute, for mitral valve surgery between November 2001 and November 2004. They were divided into two groups according to being subjected to surgical ablation of chronic atrial fibrillation using radiofrequency energy in addition to the mitral valve surgery.

13
Exclusion criteria: Patients with associated aortic valve disease are excluded from the study due to expected elongation of cross clamp time needed for double valve replacement. Exclusion criteria: Patients with associated aortic valve disease are excluded from the study due to expected elongation of cross clamp time needed for double valve replacement.

14
All patients were subjected to the following: Clinical assessment Electrocardiography Echocardiography Surgical procedure All patients were subjected to the following: Clinical assessment Electrocardiography Echocardiography Surgical procedure

15
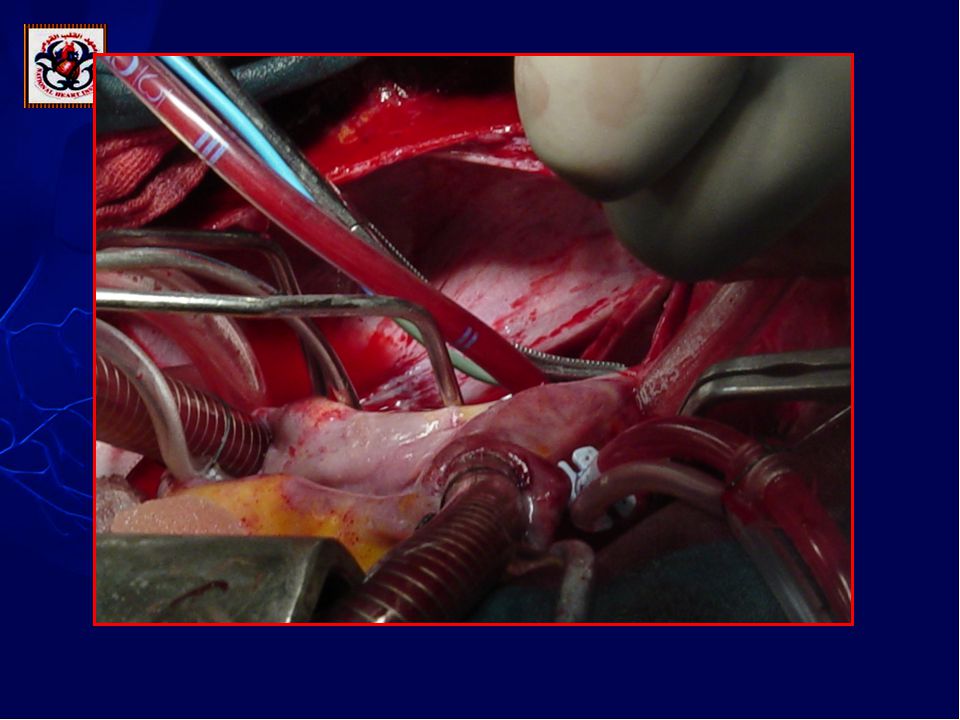
Surgical procedure : Tricuspid valve repair on a beating heart. Warm cardioplegia. Normothermia ( core temperature 36°C ). Mitral valve surgery. Lastly, RF endocardial ablation was performed under temperature control. Surgical procedure : Tricuspid valve repair on a beating heart. Warm cardioplegia. Normothermia ( core temperature 36°C ). Mitral valve surgery. Lastly, RF endocardial ablation was performed under temperature control.
. Mitral valve surgery. Lastly, RF endocardial ablation was performed under temperature control. Surgical procedure : Tricuspid valve repair on a beating heart. Warm cardioplegia. Normothermia ( core temperature 36°C ). Mitral valve surgery. Lastly, RF endocardial ablation was performed under temperature control..")
16
RF pulses were delivered under temperature control not exceeding 70 °C for a period of 2 min. aiming to produce continuous lesion lines to encircle each pulmonary vein without any interconnecting lines. The duration of ablation for each point was not less than 8-10 seconds.

17
Scheme of the procedure : circumferential isolation of each pulmonary vein

18
Antiarrhythmic medications : all patients were started on a loading dose of amiodarone in the early post-operative period, followed by a maintenance dose of 200 mg/day for 3 months. In case of postoperative AF prior to hospital discharge, electric cardioversion was attempted either alone or in combination with the administration of amiodarone. Antiarrhythmic medications : all patients were started on a loading dose of amiodarone in the early post-operative period, followed by a maintenance dose of 200 mg/day for 3 months. In case of postoperative AF prior to hospital discharge, electric cardioversion was attempted either alone or in combination with the administration of amiodarone. Postoperative management

19
Follow-up Follow - up was performed on post- operative days 1, 7, & 14 and after 1, 3 & 6 months. At each follow- up visit, clinical history, ECG, and echocardiogram were obtained. Follow - up was performed on post- operative days 1, 7, & 14 and after 1, 3 & 6 months. At each follow- up visit, clinical history, ECG, and echocardiogram were obtained.

20
Anticoagulation regimen The anticoagulation regimen was started on the second postoperative day by IV heparin administered to each patient in the two groups, with the activated partial thromboplastin time kept between 1.5 & 2 times that of the control time for 7-14 days until the targeted INR was reached.

25
This study included 60 patients referred for elective mitral valve surgery +/- tricuspid valve repair. The patients included 19 men & 41 women, ranging in age from 18 to 65 years (average 35.5 ± 11.9 y). This study included 60 patients referred for elective mitral valve surgery +/- tricuspid valve repair. The patients included 19 men & 41 women, ranging in age from 18 to 65 years (average 35.5 ± 11.9 y).
. This study included 60 patients referred for elective mitral valve surgery +/- tricuspid valve repair. The patients included 19 men & 41 women, ranging in age from 18 to 65 years (average 35.5 ± 11.9 y)..")
26
Patients were subdivided into two groups : Group (A): thirty patients who were subjected to circumferential pulmonary vein isolation using RF ablation in addition to the mitral valve surgery (RF group). Group (B): another thirty patients were subjected to mitral valve surgery alone without any ablative procedures for the atrial fibrillation and served as the control group. Patients were subdivided into two groups : Group (A): thirty patients who were subjected to circumferential pulmonary vein isolation using RF ablation in addition to the mitral valve surgery (RF group). Group (B): another thirty patients were subjected to mitral valve surgery alone without any ablative procedures for the atrial fibrillation and served as the control group.
: another thirty patients were subjected to mitral valve surgery alone without any ablative procedures for the atrial fibrillation and served as the control group. Patients were subdivided into two groups : Group (A): thirty patients who were subjected to circumferential pulmonary vein isolation using RF ablation in addition to the mitral valve surgery (RF group). Group (B): another thirty patients were subjected to mitral valve surgery alone without any ablative procedures for the atrial fibrillation and served as the control group..")
27
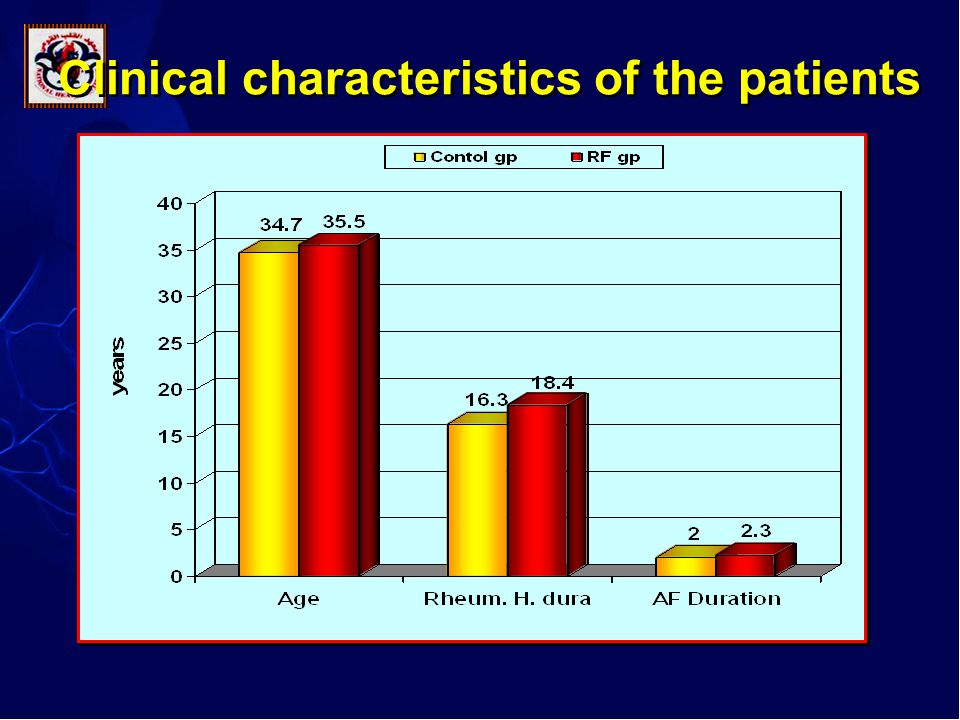
p value Control group Group B Group B N=30 N=30 RF group Group A N=30 Clinical data NS 34.7+11.0 (18-55) 35.5+12.9 (18-65) Age (yrs) NS9(30%)21(70%) 10 (33.3%) 20(66.7%)GenderMaleFemale NS 2.0+0.80 (0.5-4)2.3±1(1-5) Duration of AF (years) NS 16.3+5.06 18.4+8.8 Duration of rheumatic history (years) Clinical characteristics of the patients
 (18-65) Age (yrs) NS9(30%)21(70%) 10 (33.3%) 20(66.7%)GenderMaleFemale NS (0.5-4)2.3±1(1-5) Duration of AF (years) NS Duration of rheumatic history (years) Clinical characteristics of the patients")
29
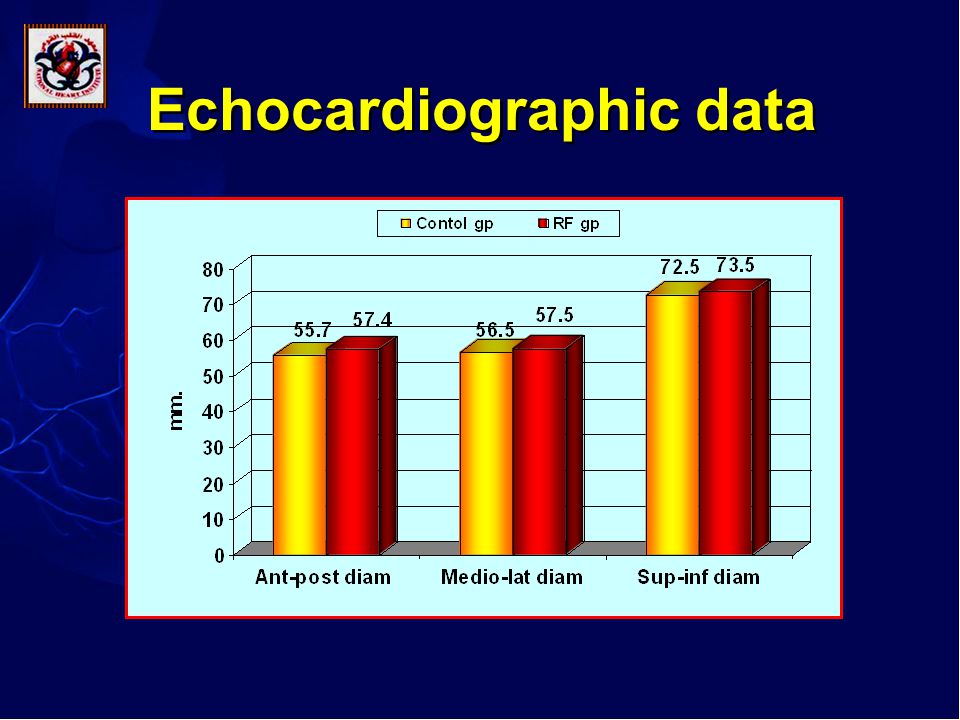
p value Group B (control group ) Group A (RF group) Echocardiographic data NS 55.9+0.5 57+0.45 LVEDD (mm) NS 38.6+0.6 40.5+0.5 LVESD(mm) NS 31+5 30+4 FS% NS 60+6 59+6 EF % NS 55.7+5.3 (46-67) 57.4+5.7 (48-68) LA. Antero-posterior diameter. (mm) NS 56.5+6.4 (45-75) 57.5+7.3 (45-75) LA. Medio-lateral diameter. (mm) NS 72.5+9.5 (58-92) 73.5+11.1 (58-97) LA. Superior-inferior diameter. (mm) Echocardiographic data
 NS (45-75) (45-75) LA. Medio-lateral diameter. (mm) NS (58-92) (58-97) LA. Superior-inferior diameter. (mm) Echocardiographic data.")
31
p value Group B (control group ) N=30 Group A (RF group) N=30 N=30 Postoperative Rhythm <0.001*20(66.7%)10(33.3%)02(6.7%)20(66.7%)8(26.6%) Immediately postoperative AFSRJR <0.001*20(66.7%)10(33.3%)04(13.3%)25(83.3%)1(3.3%) At hospital discharge AFSRJR <0.001*24(80%)6(20%)9(30%)21(70%) 3 month postoperative AFSR <0.001*27(90%)3(10%)12(40%)18(60%) 6 month postoperative AFSR Postoperative Cardiac Rhythm
 N=30 Group A (RF group) N=30 N=30 Postoperative Rhythm <0.001*20(66.7%)10(33.3%)02(6.7%)20(66.7%)8(26.6%) Immediately postoperative AFSRJR <0.001*20(66.7%)10(33.3%)04(13.3%)25(83.3%)1(3.3%) At hospital discharge AFSRJR <0.001*24(80%)6(20%)9(30%)21(70%) 3 month postoperative AFSR <0.001*27(90%)3(10%)12(40%)18(60%) 6 month postoperative AFSR Postoperative Cardiac Rhythm")
32
Immediately postoperative

33
6 month postoperative Postoperative Cardiac Rhythm

34
Percentage of SR restoration in both RF and control groups

35
Surgical procedure p value Control group (group B) RF group (group A) <0.001 69.8± 5.9 86± 7.7 CPB (min.) <0.001 52.4± 6.25 64.2± 8.7 ACC (min.) 3028MVR 01 MV repair 01 MV redo 2123 Associated TV repair Cardiac tamponade mediastinitis Early complications
 RF group (group A) < ± ± 7.7 CPB (min.) < ± ± 8.7 ACC (min.) 3028MVR 01 MV repair 01 MV redo 2123 Associated TV repair Cardiac tamponade mediastinitis Early complications")
36
Echocardiographic data of the patients in RF group: preoperatively, immediately postoperative, & after 6 months 6months postoperative Immediate postoperative Preoperative Echocardiographic data 56.4 ± 0.28 57 ± 0.46 57+0.45 LVEDD ( mm) 38.4 ± 0.32 40.6 ± 0.49 40.5+0.5 LVESD (mm) 32 ± 3 28 ± 4 30+4 FS % 61 ± 5 56 ± 6 59+6 EF % 51.1 ± 7.2 50.4 ± 6.8 57.4+5.7 LA. Antero- posterior diameter. (mm) 50.5 ± 6.5 51.6 ± 5.5 57.5+7.3 LA. Medio-lateral diameter. (mm) 64.9 ± 9.4 65.9 ± 7.9 73.5+11.1 LA. Superior-inferior diameter.(mm)
 50.5 ± ± LA. Medio-lateral diameter. (mm) 64.9 ± ± LA. Superior-inferior diameter.(mm).")
37
Biatrial contraction was documented by the presence of A wave transmitral and tricuspid flow using transthoracic Doppler echocardiography in 83.6% of patients in SR in the RF group within six months of the operation.

38
Echocardiographic data of patients in control group: preoperatively, immediately postoperative, & after 6 months 6 months postoperative Immediate postoperative Preoperative Echocardiograph ic data 55.2 ± 0.36 56.1 ± 0.46 55.9 + 0.52 LVEDD ( mm) 37.4 ± 0.37 39.9 ± 0.49 38.6+0.6 LVESD (mm) 32 ± 3 29 ± 4 31 + 5 FS % 62 ± 5 57 ± 6 60 + 6 EF % 52.5 ± 4.8 50.1 ± 5.0 55.7+5.3 LA. Antero- posterior diameter. (mm) 50.4 ± 4.5 51.1 ± 4.5 56.5+6.4 LA. Medio-lateral diameter. (mm) 63.8 ± 5.3 65.5 ± 6.4 72.5+9.5 LA. Superior- inferior diameter.(mm)
 50.4 ± ± LA. Medio-lateral diameter. (mm) 63.8 ± ± LA. Superior- inferior diameter.(mm).")
39
Factors that might be influencing recurrence of atrial fibrillation Preoperative variables Age Duration of AF Type of MV disease Left atrial diameters Left ventricular EF Preoperative variables Age Duration of AF Type of MV disease Left atrial diameters Left ventricular EF Intraoperative variables Duration of CPB Duration ACC Diameter of dilated of pulmonary vein orifices. Intraoperative variables Duration of CPB Duration ACC Diameter of dilated of pulmonary vein orifices.

40
p value Atrial fibrillation Sinus rhythm Characteristic 1218 No of patients NS40±12.832±12.2Age NS 22 ± 11 15 ± 5 Duration of rheumatic process (yrs) <.0023±1.141.8±0.7 AF duration(yrs) Comparison of patients' clinical characteristics with and without AF in the RF group
 <.0023± ±0.7 AF duration(yrs) Comparison of patients clinical characteristics with and without AF in the RF group")
41
Characteristic Sinus rhythm Atrial fibrillation p value No of patients 1812 LSPV (mm) LSPV (mm)16.3±2.518.8±2.3<.017 LIPV (mm) 17.4±4.319.2±2.3<.011 RSPV(mm)15.5±3.319.3±4.1<.004 RIPV(mm)15.3±2.318.2±4.2<.043 CPB(min) 86.4± 8 85± 7.5 NS Patients' Intraoperative Findings in RF subgroups ( with and without AF )
 LSPV (mm)16.3± ±2.3<.017 LIPV (mm) 17.4± ±2.3<.011 RSPV(mm)15.5± ±4.1<.004 RIPV(mm)15.3± ±4.2<.043 CPB(min) 86.4± 8 85± 7.5 NS Patients Intraoperative Findings in RF subgroups ( with and without AF )")
43
Comparison of patients' echocardiographic data with and without AF in the RF group p value RF group Characteristic Atrial fibrillation Sinus rhythm 1218 No of patients <.00561±5.154.9±4.7 Preoperative LA diameter [antero-post.] mm [antero-post.] mm <0.00158.4±5.746.2±4 Postoperative LA diameter [antero-post.] mm [antero-post.] mm <0.0015%15% % change in LA diameter [anter-post.] [anter-post.] <.0162±7.754.5±5.2 Preoperative LA diameter [med.-lat.] mm [med.-lat.] mm <.00155.9±6.746.8±2.7 Postoperative LA diameter [med.-lat.] mm [med.-lat.] mm <.00280.1±10.568.6±8.7 Preoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm <.00171.4±10.96o.6±5.0 Postoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm
![Comparison of patients echocardiographic data with and without AF in the RF group p value RF group Characteristic Atrial fibrillation Sinus rhythm 1218 No of patients <.00561± ±4.7 Preoperative LA diameter [antero-post.] mm [antero-post.] mm < ± ±4 Postoperative LA diameter [antero-post.] mm [antero-post.] mm <0.0015%15% % change in LA diameter [anter-post.] [anter-post.] <.0162± ±5.2 Preoperative LA diameter [med.-lat.] mm [med.-lat.] mm < ± ±2.7 Postoperative LA diameter [med.-lat.] mm [med.-lat.] mm < ± ±8.7 Preoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm < ±10.96o.6±5.0 Postoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm](http://images.slideplayer.com/20/5981026/slides/slide_43.jpg "Comparison of patients echocardiographic data with and without AF in the RF group p value RF group Characteristic Atrial fibrillation Sinus rhythm 1218 No of patients <.00561± ±4.7 Preoperative LA diameter [antero-post.] mm [antero-post.] mm < ± ±4 Postoperative LA diameter [antero-post.] mm [antero-post.] mm <0.0015%15% % change in LA diameter [anter-post.] [anter-post.] <.0162± ±5.2 Preoperative LA diameter [med.-lat.] mm [med.-lat.] mm < ± ±2.7 Postoperative LA diameter [med.-lat.] mm [med.-lat.] mm < ± ±8.7 Preoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm < ±10.96o.6±5.0 Postoperative LA diameter [sup.-inf.] mm [sup.-inf.] mm")
44
Echocardiographic Findings (pre & postoperative) in the RF subgroups (with and without AF )
 in the RF subgroups (with and without AF )")
45
Percentage of SR restoration of patients in RF group according to their left atrial antero-posterior diameters RF Group Postoperative Rhythm Group (3) ≥ 60mm (n=10 ) Group (2) 55-59mm (n=8) Group (1) ≤54mm (n= 12) 9(90%)1(10%)7(87.5%)1(12.5%)12(100%)(0%) Immediately postoperative SRAF 8(80%)2(20%)7(87.5%)1(12.5%)11(91.6%)1(8.3%) At hospital discharge SRAF 4(40%)6(60%)6(75%)2(25%)11(91.6%)1(8.3%) 3 month postoperative SRAF 3(30%)7(70%)4(50%)4(50%)11(91.6%)1(8.3%) 6 month postoperative SRAF
 ≥ 60mm (n=10 ) Group (2) 55-59mm (n=8) Group (1) ≤54mm (n= 12) 9(90%)1(10%)7(87.5%)1(12.5%)12(100%)(0%) Immediately postoperative SRAF 8(80%)2(20%)7(87.5%)1(12.5%)11(91.6%)1(8.3%) At hospital discharge SRAF 4(40%)6(60%)6(75%)2(25%)11(91.6%)1(8.3%) 3 month postoperative SRAF 3(30%)7(70%)4(50%)4(50%)11(91.6%)1(8.3%) 6 month postoperative SRAF")
46
Percentage of SR restoration of patients in control group according to their left atrial antero- posterior diameters Group (3) ≥ 60mm (n=7) Group (2) 55-59mm(n=8) Group (1) ≤54mm (n= 15) Postoperative Rhythm 0(0%)7(100%)1(12.5%)7(87.5%)9(60%)6(40%) Immediately postoperative SR SR AF AF 1(14.3%)6(85.7%)2(25%)6(75%)7(46.6%)8(53.3%) Immediately postoperative SR SR AF AF 0(0%)7(100%)0(0%)8(100%)6(40%)9(60%) 3 month postoperative SR SR AF AF 0(0%)7(100%)0(0%)8(100%)3(20%)12(80%) 6 month postoperative SR SR AF AF
 ≥ 60mm (n=7) Group (2) 55-59mm(n=8) Group (1) ≤54mm (n= 15) Postoperative Rhythm 0(0%)7(100%)1(12.5%)7(87.5%)9(60%)6(40%) Immediately postoperative SR SR AF AF 1(14.3%)6(85.7%)2(25%)6(75%)7(46.6%)8(53.3%) Immediately postoperative SR SR AF AF 0(0%)7(100%)0(0%)8(100%)6(40%)9(60%) 3 month postoperative SR SR AF AF 0(0%)7(100%)0(0%)8(100%)3(20%)12(80%) 6 month postoperative SR SR AF AF")
47
Percentage of SR restoration in RF group according to the left atrial diameters

52
Data in this study are encouraging for using this new approach in eliminating AF associated with mitral valve disease. Simple "circumferential isolation of each pulmonary vein" ablation lines met the essential requirements to eliminate AF; is simple, easy, and quick to perform; effectively eliminated AF Data in this study are encouraging for using this new approach in eliminating AF associated with mitral valve disease. Simple "circumferential isolation of each pulmonary vein" ablation lines met the essential requirements to eliminate AF; is simple, easy, and quick to perform; effectively eliminated AF

53
It helped in restoration and maintenance of a normal sinus rhythm in a considerable percentage of patients with long standing AF secondary to mitral valve disease at an average follow-up period of six months. Atrial transport function was restored in 83.6% of the patients in SR. It helped in restoration and maintenance of a normal sinus rhythm in a considerable percentage of patients with long standing AF secondary to mitral valve disease at an average follow-up period of six months. Atrial transport function was restored in 83.6% of the patients in SR.

54
It is effective and does not require either new technical resources or additional training of surgical teams. The preoperative left atrial diameter and preoperative AF duration are important determinant that might be influencing the sinus conversion rate. It is effective and does not require either new technical resources or additional training of surgical teams. The preoperative left atrial diameter and preoperative AF duration are important determinant that might be influencing the sinus conversion rate.

Similar presentations
















>")








 Trial Presented at The American College of Cardiology Scientific Session 2006 Presented by Dr. Carlo.>")



 Persistent Sustained > 7 days, or lasting < 7 days but requires pharmacologic.>")
