Download presentation
Presentation is loading. Please wait.

1
TRACHEOSTOMY AND OTHER PROCEDURES FOR AIRWAY MANAGEMENT
Dr. Sudeep K.C.

2
TRACHEOSTOMY: It is making an opening in anterior wall of trachea and converting it into stoma on the skin surface. FUNCTIONS OF TRACHEOSTOMY: Alternative pathway for breathing. Improves the alveolar ventilation. Protects the airway. Permits removal of tracheobronchial secretions. Intermittent positive pressure respiration. To administer anaesthesia.

3
INDICATIONS OF TRACHEOSTOMY
There are three main indication: Respiratory obstruction. Retained secretions. Respiratory insufficiency.

4
Respiratory obstruction-
Infections Trauma Neoplasms Foreign body larynx Oedema larynx due to steam , \ irritant fumes or gases, allergy Bilateral abductor paralysis Congenital anomalies

5
Retained secretions Inability to cough Painful cough
Aspiration of pharyngeal secreations.

6
Respiratory insufficiency
Chronic lung conditions Conditions listed in above both

7
FEELING BORING ????? WANNA LAUGH!!!!????? PLEASE TRY TO CONTROL

10
TYPES OF TRACHEOSTOMY 1)Emergency tracheostomy
2) Elective tracheostomy a) Therapeutic to relieve respiratory obstruction, remove tracheobronchial secretion or give assisted ventilation. b)prophylactic , to guard against anticipated respiratory obstruction or aspiration of blood or pahryngeal secretions .
 Elective tracheostomy. a) Therapeutic to relieve respiratory obstruction, remove tracheobronchial secretion or give assisted ventilation. b)prophylactic , to guard against anticipated respiratory obstruction or aspiration of blood or pahryngeal secretions .")
11
3)Permanent tracheostomy for bilateral abductor paralysis or laryngeal stenosis.
Permanent tracheostomy for bilateral abductor paralysis or laryngeal stenosis.")
12
Tracheostomy has also been divided into :
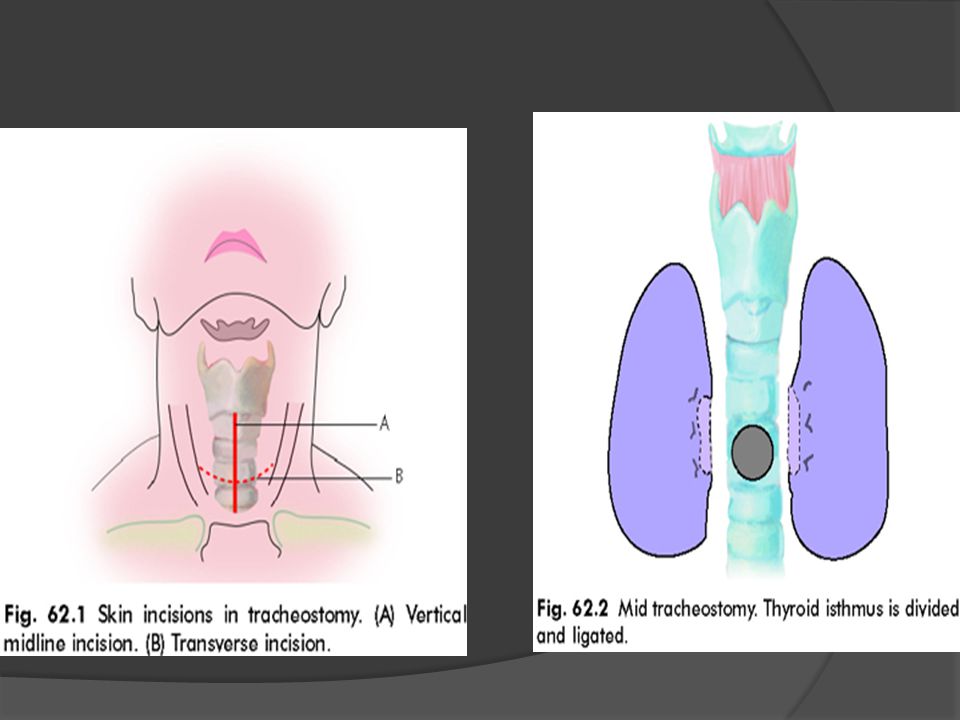
A) High tracheostomy : done above level of thyroid isthmus. Indication is ca larynx. B)Mid tracheostomy: it is the preferred one and done through II and III rings, division of isthmus. C) Low tracheostomy: done below level of isthmus . trachea is deep at this level and close to several large vessels.
 High tracheostomy : done above level of thyroid isthmus. Indication is ca larynx. B)Mid tracheostomy: it is the preferred one and done through II and III rings, division of isthmus. C) Low tracheostomy: done below level of isthmus . trachea is deep at this level and close to several large vessels.")
13
STEPS OF OPERATION A vertical incision is made in midline of neck , extending from cricoid cartilage to just above sternal notch. Transverse incision 5cm long given 2 fingers above notch in elective procedure. Tissues are dissected in the midline.Dilated veins are either ligated or displaced. Strap muscles are separated in midline and retracted laterally.

15
Throid isthmus is displaced upward or divided between clamps, and suture –ligated.
A few drops of 4% lignocaine are injected into trachea to supress cough when trachea is incised. Trachea is fixed with hook and opened with vertical incision in region of 3rd and 4th or 3rd and 2nd rings. .

16
This is then converted into circular opening
This is then converted into circular opening.ist tracheal ring shouldn’t be divided. Tracheostomy tube of appropriate size is inserted. Skin incision shouldn’t be sutured or packed tightly otherwise lead to subcutaneous emphysema. Gauze dressing is placed between the skin and flange of tube around stoma.

17
POST OPERATIVE CARE: 1)Constant supervision for bleeding, displacement, blocking of tube and removal of secretions is essential. 2)Suction depending on amount of secretion every half an hr. 3)Prevention of crusting and tracheitis. 4)Care of tracheostomy tube.
Suction depending on amount of secretion every half an hr. 3)Prevention of crusting and tracheitis. 4)Care of tracheostomy tube.")
18
DECANNULATION Tracheostomy tube should be kept longer than necessary . Prolonged use leads to infections, tracheal ulceration, granulations , stenosis . To decannulate , tube is plugged and patient closely observed if patient can tolerate it for 24 hr tube can be safely removed. After tube removal , wound is taped and patient again closely observed. Healing of wound will take place within few days or weeks.

19
COMPLICATIONS: A) Immediate(at the time of operation) Haemorrhage.
Apnoea. Pneumothorax. Injury to recurrent laryngeal nerves. Aspiration of blood. Injury to oesophagus.

20
B) Intermediate(during first few hrs or days.)
Bleeding, reactionary or secondary. Displacement of tube. Blocking of tube. Subcutaneous emphysema. Tracheitis and tracheobronchitis with crusting in trachea. Atelectasis and lung abscess. Local wound infection and granulations.

21
C) Late (with prolonged use of tube for weeks and months)
Haemorrhage, due to erosion of major vessel. Laryngeal stenosis, due to perichondritis of cricoid cartilage. Tracheal stenosis, due to tracheal ulceration and infection. Tracheo-oesophageal fistula Problems of decannulation Persistent tracheocutaneous fistula. Problem of tracheostomy scar like keloid. Corrosion of tracheostomy tube and aspiration of its fragment into tracheobronchial tree.

22
PROCEDURES FOR IMMEDIATE AIRWAY MANAGEMENT:
1) Jaw thrust 2)Oropharyngeal airway. 3)Nasopharyngeal airway (trumpet) 4)Laryngeal mask airway. 5)Transtracheal jet ventilation
 Jaw thrust. 2)Oropharyngeal airway. 3)Nasopharyngeal airway (trumpet) 4)Laryngeal mask airway. 5)Transtracheal jet ventilation.")
23
6)Endotracheal intubation.
7)Cricothyrotomy or laryngotomy. 8)Emergency tracheostomy.
Cricothyrotomy or laryngotomy. 8)Emergency tracheostomy.")
24
ITS MOVIE TIME …

Similar presentations







 – Oral-tracheal – Naso-tracheal Tracheostomy (trach) 1.>")








 Amended 2012.>")




