Download presentation
Presentation is loading. Please wait.

1
Epidemiology and diagnosis of acute pulmonary embolism Dr Sam Z Goldhaber Associate Professor of Medicine Harvard Medical School Staff Cardiologist Brigham and Women’s Hospital Boston, MA

4
Risk factors for PE Nurses’ Health Study 1)Obesity (RR = 3.0, with BMI >29) 2)Cigarette smoking (RR = 2.1, with > 35 cigs/d) 3)Hypertension (RR = 1.5) JAMA 1997; 277:642
Obesity (RR = 3.0, with BMI >29) 2)Cigarette smoking (RR = 2.1, with > 35 cigs/d) 3)Hypertension (RR = 1.5) JAMA 1997; 277:642")
5
Hypercoagulability work-up High yield (> 20%) 1)Factor V Leiden – Genetic mutation that causes resistance to activated protein C 2)Plasma homocysteine level – Rx with folate, B6, B12 3)Lupus anticoagulant screen – Requires intensive anticoagulation; Possible steroid/ASA responsiveness
 1)Factor V Leiden – Genetic mutation that causes resistance to activated protein C 2)Plasma homocysteine level – Rx with folate, B6, B12 3)Lupus anticoagulant screen – Requires intensive anticoagulation; Possible steroid/ASA responsiveness")
6
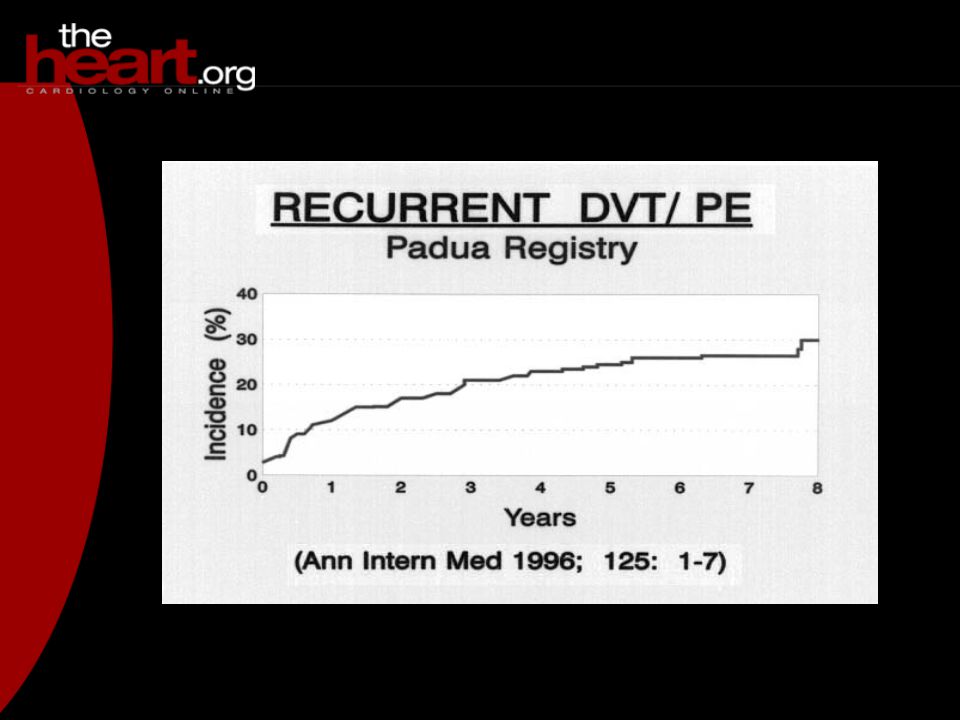
Leiden/recurrent VTE after discontinuing warfarin RR = 4.7 (p = 0.047) (PHS: Circulation 1995; 92:2800) RR = 2.4 (p < 0.01) (Padua: NEJM 1997; 336:399) No increased risk (Rintelen: Thromb Haemostas 996; 75:229)
 (PHS: Circulation 1995; 92:2800) RR = 2.4 (p < 0.01) (Padua: NEJM 1997; 336:399) No increased risk (Rintelen: Thromb Haemostas 996; 75:229)")
7
ACLA and VTE 412 Swedish patients 14% ACLA in men 17% ACLA in women 29% recurrence in ACLA positive vs 14% recurrence in ACLA negative 15% vs 6% 4-year mortality Am J Med 998; 104:332

8
Prothrombin gene mutation risk DVT/PE (Ann Intern Med 1998; 129:89) risk cerebral vein thrombosis (NEJM 1998; 338:1793)
 risk cerebral vein thrombosis (NEJM 1998; 338:1793)")
9
Hypercoagulability work-up Low yield 1)antithrombin III deficiency (spurious value on heparin) 2)protein C deficiency (spurious value on warfarin, BCP or when pregnant) 3)protein S deficiency (spurious value on warfarin, BCP or when pregnant)
antithrombin III deficiency (spurious value on heparin) 2)protein C deficiency (spurious value on warfarin, BCP or when pregnant) 3)protein S deficiency (spurious value on warfarin, BCP or when pregnant)")
10
Signs/Sx PE (n = 131) ObservationRate Dyspnea77% Chest pain55% Cyanosis18% Hemoptysis13% Syncope10% Arch Intern Med 1991; 151:933
 ObservationRate Dyspnea77% Chest pain55% Cyanosis18% Hemoptysis13% Syncope10% Arch Intern Med 1991; 151:933")
13
BLOOD ACTIVATION fibrinogenfibrin monomersfibrin clot thrombin F XIII F XIIIa plasmin FDP fibrinogen degradation products FIBRINOLYSIS D-Dimers (XDP) Figure 1: D-Dimer is exclusively from fibrin clot DD
 Figure 1: D-Dimer is exclusively from fibrin clot DD")
14
D-Dimer for PE diagnosis Overview of 9 trials (n = 908) ELISA assay; 38% have positive scans/PAgrams Sensitivity Specificity PPV NPV 97% 45% 50% 94% Thromb Haemostas 1994; 71:1-6
 ELISA assay; 38% have positive scans/PAgrams Sensitivity Specificity PPV NPV 97% 45% 50% 94% Thromb Haemostas 1994; 71:1-6")
15
High probability lung scans are insensitive for PE Scan interpretationSensitivity (%)Specificity (%) High 41 97 59% of patients with PE have non-high probability scans JAMA 1990; 263:2753-9
Specificity (%) High % of patients with PE have non-high probability scans JAMA 1990; 263:2753-9")
16
Normal (left) and abnormal (right) venous ultrasounds (C = compression)
 and abnormal (right) venous ultrasounds (C = compression)")
17
Venography for suspected PE Venography Pulmonary angiography PositiveNegative Positive2911 Negative1222 Total4133 Hull et al. Ann Intern Med 1983; 98:891

18
CT scan with contrast showing main bilateral pulmonary embolism

19
Echocardiogram suggesting a PE. Diastole on the left, systole on the right

20
PE diagnosis strategy High probability TREAT High D-dimer CONTINUE W/U Normal D-dimer STOP W/U If leg U/S normal PAgram (or CT) If Echo normal PAgram (or CT) Intermediate or low probability Normal STOP W/U Lung (or CT) scan
 If Echo normal PAgram (or CT) Intermediate or low probability Normal STOP W/U Lung (or CT) scan")
Similar presentations










 IPC/GCS or, UFH 5000 SQ q 12 hrs or, Enoxaparin 40mg SQ daily IPC/GCS or, UFH 5000.>")









 Zone Technical Application Specialist Siemens Healthcare.>")
