Download presentation
Presentation is loading. Please wait.

1
Health Care Reform? P-PACA vs Single Payer Oliver Fein, M.D. Professor of Clinical Medicine and Public Health Associate Dean Office of Affiliations Office of Global Health Education Weill Cornell Medical College Institution Name Update March 21, 2011

2
DISCLOSURES Dr. Oliver Fein has no relevant financial relationships with commercial interests Dr. Oliver Fein is immediate past President of Physicians for a National Health Program (PNHP), a non-profit educational and advocacy organization. He receives no financial compensation from PNHP.
, a non-profit educational and advocacy organization. He receives no financial compensation from PNHP..")
3
PRESENTATION OUTLINE 1.History of recent U.S. Health Reform 2.Challenges facing U.S. Health Care System 3.Comparison of Single Payer and 2010 Health Reform (P-PACA)
.")
4
HEALTH REFORM: OBAMA’S FATEFUL CHOICE He did not want to “start from scratch” He had two fundamental choices: 1) to build on the public sector (Medicare) or 2) to build on the private sector He chose to build on the private sector by mandating that everyone buy private health insurance or a public option
 to build on the public sector (Medicare) or 2) to build on the private sector He chose to build on the private sector by mandating that everyone buy private health insurance or a public option")
5
Progress(?) of US Health Reform Employer mandate Public option** Individual mandate* * “each eligible individual must enroll in an applicable health plan for the individual and must pay any premium required with respect to such enrollment.” (S.1775) ** “you can choose to enroll in the new public plan” Medicare ??
 of US Health Reform Employer mandate Public option** Individual mandate* * each eligible individual must enroll in an applicable health plan for the individual and must pay any premium required with respect to such enrollment. (S.1775) ** you can choose to enroll in the new public plan Medicare")
6
WHAT HAPPENED TO THE PUBLIC OPTION? The original “robust” Plan Open enrollment: “Medicare for everyone who wants it” Medicare rates, backed by the government 119 million members (Lewin) The House Plan Restricted enrollment (only the uninsured) 6 million members (<2% of the population) Negotiated rates, self sustaining The Senate Plan No public option
 The House Plan Restricted enrollment (only the uninsured) 6 million members (<2% of the population) Negotiated rates, self sustaining The Senate Plan No public option.")
7
THE PATIENT PROTECTION AND AFFORDABLE CARE ACT (P-PACA) March 23, 2010 Health insurance reform, not health care reform
 March 23, 2010 Health insurance reform, not health care reform")
8
P-PACA (a MANDATE MODEL) Everyone is required to have health insurance or pay a penalty. 1.Individual mandate: penalty =$695 for singles; $2,085 for families 2.Employer mandate (50 or more employees): penalty =$2,000/employee 3.Necessary for the survival of private HI. Private HI lost 3.2% (6.3 million) enrollees in 2009 and more than 15 million in the last decade.
: penalty =$2,000/employee 3.Necessary for the survival of private HI. Private HI lost 3.2% (6.3 million) enrollees in 2009 and more than 15 million in the last decade..")
9
Improved MEDICARE FOR ALL (a Single Payer Model) Build on the original Medicare 1.Improve Coverage: preventive services, oral surgery, long term care 2.Reduce or eliminate deductibles and co- payments 3.Expand drug coverage: eliminate the “donut hole” 4.Re-design physician reimbursement
 Build on the original Medicare 1.Improve Coverage: preventive services, oral surgery, long term care 2.Reduce or eliminate deductibles and co- payments 3.Expand drug coverage: eliminate the donut hole 4.Re-design physician reimbursement")
10
CHALLENGES FACING HEALTH CARE REFORM 1.Declining access 2.Escalating costs 3.Lack of comprehensive benefits 4.Restricted choice 5.Uneven Quality 6.Insufficient primary care 7.How to pay for reform

11
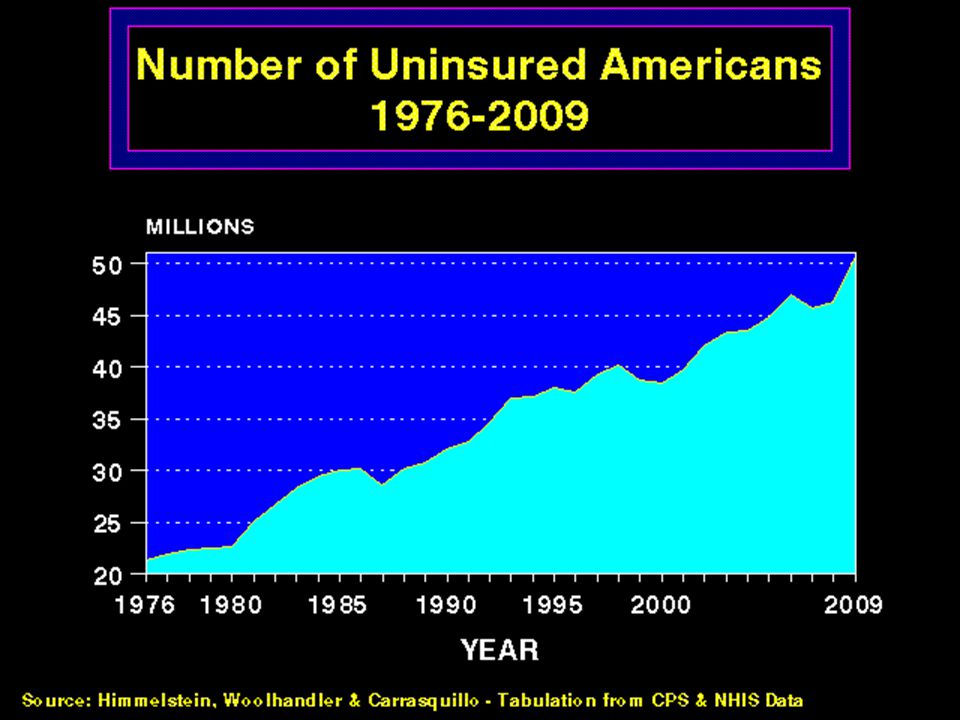
CHALLENGE #1 DECLINING ACCESS

13
The Epidemic of Underinsurance Source: Too Great a Burden, Families USA, December 2007 Number of people spending more than 10% of income on health care (Millions)
")
14
Improved MEDICARE FOR ALL Automatic enrollment Federal guarantee All residents of the United States “Everybody in, nobody out”

15
HEALTH INSURANCE REFORM (P-PACA) Mandates purchase of private HI (2014) Expands Medicaid eligibility to 133% FPL (2014) - single $14,403; family $19,378 Subsidizes premiums up to 400% FPL (2014) - single $43,320; family $88,200 Insurance market reforms: Guaranteed issue; no rescissions; no annual/life limits
 Mandates purchase of private HI (2014) Expands Medicaid eligibility to 133% FPL (2014) - single $14,403; family $19,378 Subsidizes premiums up to 400% FPL (2014) - single $43,320; family $88,200 Insurance market reforms: Guaranteed issue; no rescissions; no annual/life limits")
16
MEASURES of P-PACA EFFECT in 2011 How many more children with pre-existing conditions covered? How many young adults <26 years old opt for coverage under parents policies? How many seniors make annual wellness visits? How many seniors in the donut hole use the 50% brand name or 7% generic discounts? How many enroll in the state high risk pools? How many benefit from ban on annual/lifetime limits?

17
Millions Will Remain Uninsured (and Millions More Poorly Insured) Millions Note: The uninsured include about 5 million undocumented immigrants. Source: Congressional Budget Office.

18
CHALLENGE #2 ESCALATING COSTS

19
Insurance Premiums Workers’ Earnings Inflation 1999-2008 Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2000-2008. Bureau of Labor Statistics, Consumer Price Index

20
High Cost of Health Insurance Premiums: It’s Even Too Expensive for the Middle Class Today National Average for Employer-provided Insurance Single Coverage $5,049 per year Family Coverage $13,770 per year Note: Annual income at minimum wage = $13,624 Annual income of average Wal-Mart worker = $17,114 Source: Kaiser Family Foundation/HRET Survey of Employee Benefits, 2010

21
RISE IN PERSONAL BANKRUPTCIES 62% of personal bankruptcies are due to medical expenses and over 75% had health insurance at the outset of their bankrupting illness.* * Himmelstein, et.al. Am J Med, August, 2009

22
Improved MEDICARE FOR ALL Low Administrative Costs = Single Payer Administrative cost and profit - Medicare: 2-3 % - Private insurance: 16-30% $400 billion* redirected to cover the uninsured and to expand coverage for the underinsured * NEJM 2003:349;768-775 updated to 2010

23
Covering Everyone and Saving Money through Medicare for All Additional costs Covering the uninsured and poorly-insured +6.4% Elimination of cost-sharing and co-pays +5.1% Savings Reduced insurance administrative costs -5.3% Reduced hospital administrative costs -1.9% Reduced physician office costs -3.6% Bulk purchasing of drugs & equipment -2.8% Primary care emphasis & reduce fraud -2.2% Source: Health Care for All Californians Plan, Lewin Group, January 2005 134 107 241 -111 -21 -76 -59 -46 -313 $ B Total Costs +11.5% Total Savings -15.8% Net Savings - 4.3% - 73

25
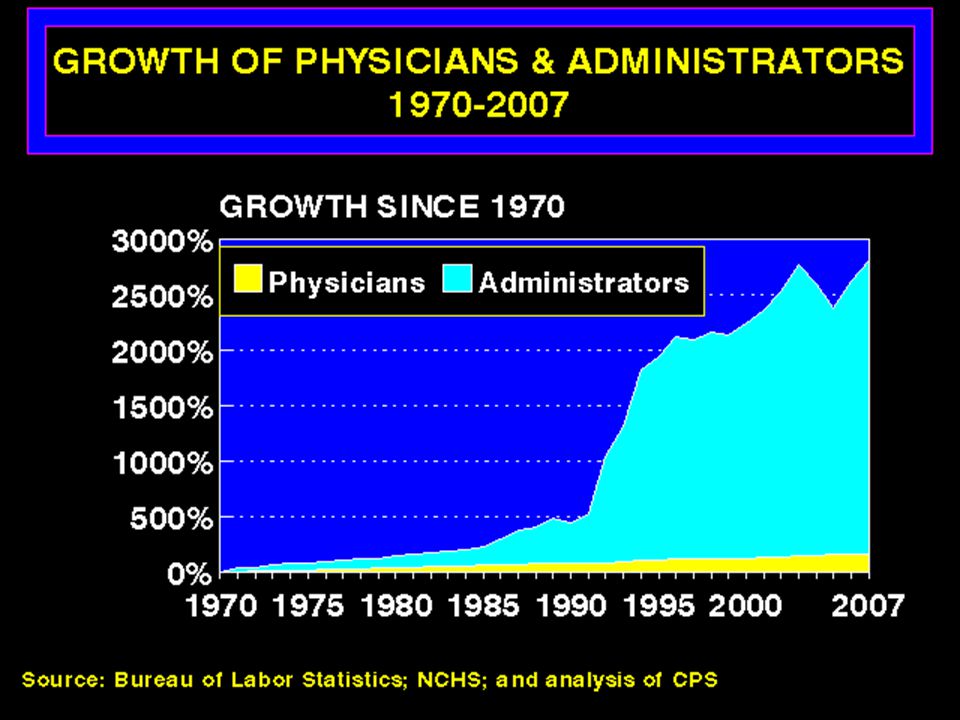
Private insurers’ High Overhead

26
SINGLE PAYER OFFERS REAL TOOLS TO CONTAIN COSTS Global budgeting of hospitals Capital investment planning Emphasis on primary care; coordination of care; alternative ways of paying for care Bulk purchasing of pharmaceuticals

27
HEALTH INSURANCE REFORM (P-PACA) Reduces private health insurance premiums by mandating penalties for uninsurance (forcing low risks into risk pool) 1. Individual mandate (2014) 2.5% of income or $695 (singles) to $2,085 (family)-(2016) 2. Employer mandate (if 50 or more employees) $2,000/employee 3. ACOs: reduce overuse/misuse by bundling payments?
 2.5% of income or $695 (singles) to $2,085 (family)-(2016) 2. Employer mandate (if 50 or more employees) $2,000/employee 3. ACOs: reduce overuse/misuse by bundling payments .")
28
HEALTH INSURANCE REFORM (P-PACA) Leaves many of the undesirable features of employment-based insurance unchanged Employers can change coverage and plans Insurers can change provider networks Employees must accept the employer plan
 Leaves many of the undesirable features of employment-based insurance unchanged Employers can change coverage and plans Insurers can change provider networks Employees must accept the employer plan")
29
HEALTH INSURANCE REFORM (P-PACA) Offers unproven tools to contain costs Health Information Technology (HIT) Chronic Disease Management Payment reforms (e.g., ACOs, bundled payments)
 Offers unproven tools to contain costs Health Information Technology (HIT) Chronic Disease Management Payment reforms (e.g., ACOs, bundled payments)")
30
…and Costs Will Keep On Rising National Health Expenditures (trillions) Notes: * Modified current projection estimates national health spending when corrected to reflect underutilization of services by previously uninsured. Source: D. M. Cutler, K. Davis, and K. Stremikis, Why Health Reform Will Bend the Cost Curve, Center for American Progress and The Commonwealth Fund, December 2009. Estimated Financial Effects of PPACA as Amended, Richard Foster, CMS Actuary, April 2010 $4.67 $4.5 6.4% annual growth 6.6% annual growth 6.0% annual growth $4.7 National Health Expenditures as Percent of GDP 17.8 17.9 18.0 18.2 18.8 19.3 19.8 20.2 20.5 21.0

31
CHALLENGE #3 BASIC vs. COMPREHENSIVE BENEFITS Service Coverage: Doctors, NPs, Hospitals, Drugs; Dental, Mental Health, Home care/nursing home Financial Coverage: Copays and deductibles

32
Improved MEDICARE FOR ALL Comprehensive coverage - Preventive services - Hospital care - Physician services - Dental services - Mental health services - Medication expenses - Reproductive health services -Home Care/nursing home care “All medically necessary services” Any exclusions? How decided?

33
Improved MEDICARE FOR ALL Eliminates Co-Pays or Deductibles Reduce use of needed and unneeded services equally Results in under use of primary care services Not as effective in reducing over use of technology intensive services, as - Eliminating self-referral to MD owned facilities - Reducing defensive medicine

34
HEALTH INSURANCE REFORM (P-PACA) No Standard Benefit Package mandated, just coverage of annual checkups Reduces or eliminates co-pays and deductibles, but only on preventive services No regulation of the magnitude of premiums, deductibles and co-pays – just the stipulation that benefits have an actuarial value of 60% or higher Stipulation of a medical lost ratio (MLR) of 80- 85%
 No Standard Benefit Package mandated, just coverage of annual checkups Reduces or eliminates co-pays and deductibles, but only on preventive services No regulation of the magnitude of premiums, deductibles and co-pays – just the stipulation that benefits have an actuarial value of 60% or higher Stipulation of a medical lost ratio (MLR) of %")
35
CHALLENGE #4 RESTRICTED CHOICE 42% of employees have no choice Private health insurance limits choice to the network of doctors and hospitals with whom they have negotiated contracts You pay more to go out of network

36
Improved MEDICARE FOR ALL Expands Choice for Everyone No limit to a network of providers Free choice of doctor and hospital Delinks health insurance from employment

37
HEALTH INSURANCE REFORM (P-PACA) Creation of HI Exchanges Expands Choice for Some Limited to the individual and small group market Market-place of private HI plans No public option State-based with federal backup No state single payer until 2017
 Creation of HI Exchanges Expands Choice for Some Limited to the individual and small group market Market-place of private HI plans No public option State-based with federal backup No state single payer until 2017")
38
VERMONT MOVES TOWARDS SINGLE PAYER Elected Peter Schumlin governor Commissioned William Hsiao, Ph.D., Harvard economist to propose 3 options - Option 1: Government-run single payer - Option 2: HI exchange with public option - Option 3: Public-private hybrid single payer Standard benefit package Uniform prices Administered by a public benefit corporation

39
HEALTH INSURANCE REFORM (P-PACA) Restricts Choice when it comes to abortion Allows states to prohibit abortion coverage in state-run exchanges If states allow abortion coverage, requires enrollees or employers to send two checks Insurers must keep abortion coverage money separate from federal subsidies
 Restricts Choice when it comes to abortion Allows states to prohibit abortion coverage in state-run exchanges If states allow abortion coverage, requires enrollees or employers to send two checks Insurers must keep abortion coverage money separate from federal subsidies")
40
PROGRESS ON EXCHANGES 33 states have passed legislation or taken executive action to implement an exchange 28 states filed challenges to P-PACA 27 of the 28 have requested federal $ to establish exchanges

41
CHALLENGE #5: UNEVEN QUALITY In 2008, U.S. was last among 19 industrialized nations in mortality amenable to health care. In 2006, we were 15th. * Commonwealth Fund (2009)
.")
42
Improved MEDICARE FOR ALL National data on health care quality vs. proprietary data held by private HI National standards and public reporting HIT for the nation with patient protections – every patient their own medical record on a “credit” card

43
HEALTH INSURANCE REFORM (P-PACA) Comparative Effectiveness Research Innovation Center in CMS to test new payment and service delivery models (2011) Value based purchasing – hospital payments based on quality reporting measures (2013) Readmission penalties (2013) Reduce hospital payments for hospital-acquired conditions (2015)
 Comparative Effectiveness Research Innovation Center in CMS to test new payment and service delivery models (2011) Value based purchasing – hospital payments based on quality reporting measures (2013) Readmission penalties (2013) Reduce hospital payments for hospital-acquired conditions (2015)")
44
CHALLENGE #6: LACK OF PRIMARY CARE Average medical school debt = $160,000 Primary care is under-reimbursed Medical school graduates going into specialties

45
Improved MEDICARE FOR ALL Debt forgiveness for primary care Malpractice payment for primary care providers (MDs, NPs and PAs) Patient-Centered Medical Homes (team based care, open access, coordination of care; phone/internet medicine)
 Patient-Centered Medical Homes (team based care, open access, coordination of care; phone/internet medicine)")
46
HEALTH INSURANCE REFORM (P-PACA) 10% Primary Care Bonus Payments (2011- 2017) – estimate = $4,000/provider/year Increase Medicaid payment to Medicare rates for primary care (2013) Independent Payment Advisory Board (2014)
 10% Primary Care Bonus Payments ( ) – estimate = $4,000/provider/year Increase Medicaid payment to Medicare rates for primary care (2013) Independent Payment Advisory Board (2014)")
47
CHALLENGE #7 HOW TO PAY FOR REFORM

48
Improved MEDICARE FOR ALL Public funding - Payroll tax - Corporate taxes - Income taxes - Tax on unearned income (stocks, bonds, etc.) No premiums: regressive No increase in overall health care spending, because of administrative savings
 No premiums: regressive No increase in overall health care spending, because of administrative savings")
49
Improved MEDICARE FOR ALL Non-profit/private delivery system under local control - Doctors not salaried by government - Hospitals not owned by government - This is not “socialized medicine” A publicly funded-privately delivered partnership

50
HEALTH INSURANCE REFORM (P-PACA) 1.Increased taxes - Excise tax on “Cadillac” health insurance plans (2018) - Medicare payroll tax increase from 1.45% to 2.35% if income greater than $200-250K - 3.8% tax on investment income 2. Savings from Medicare - Advantage: ($132 bill over 10 yrs) - Cut DSH payments ($36 million) - Cut Medicare payments to hospitals ($136 bill over 10 yrs) - Cut payments for home care/nursing homes ($60 bill) 3. Revenue from cracking down on fraud and abuse
 - Cut DSH payments ($36 million) - Cut Medicare payments to hospitals ($136 bill over 10 yrs) - Cut payments for home care/nursing homes ($60 bill) 3. Revenue from cracking down on fraud and abuse.")
51
HEALTH REFORM (P-PACA) 1.Expanded coverage, but not universal 2.Cost control by market means 3.No definition of benefits 4.Choice thru State-based exchanges, but no public option 5.Limits on abortion 6.Primary care/ACO pilots 7.Funding: Excise tax on high cost private HI and Medicare cutbacks
 1.Expanded coverage, but not universal 2.Cost control by market means 3.No definition of benefits 4.Choice thru State-based exchanges, but no public option 5.Limits on abortion 6.Primary care/ACO pilots 7.Funding: Excise tax on high cost private HI and Medicare cutbacks")
52
Single Payer MEDICARE FOR ALL THE PHYSICIANS’ PROPOSAL (JAMA, August 13, 2003 p. 798-805) 1.Universal coverage/automatic enrollment 2.Low administrative costs=single payer 3.Comprehensive coverage without co-pays and deductibles 4.Maximum choice of Doctor, NP, Hospital 5.Improved quality through nationwide HIT 6.Expanded primary care 7.Publicly-funded/privately delivered MEDICARE 2.0
 1.Universal coverage/automatic enrollment 2.Low administrative costs=single payer 3.Comprehensive coverage without co-pays and deductibles 4.Maximum choice of Doctor, NP, Hospital 5.Improved quality through nationwide HIT 6.Expanded primary care 7.Publicly-funded/privately delivered MEDICARE 2.0.")
53
Conyers HR 676 Expanded and improved MEDICARE-FOR-ALL “Single Payer NH Care” (86 Co-sponsors in House of Rep) Automatic enrollment Comprehensive benefits Free choice of doctor and hospital Doctors and hospitals remain independent Financed through progressive taxes Costs contained through capital planning, budgeting, quality reviews, primary care emphasis
 Automatic enrollment Comprehensive benefits Free choice of doctor and hospital Doctors and hospitals remain independent Financed through progressive taxes Costs contained through capital planning, budgeting, quality reviews, primary care emphasis")
54
Sanders (& McDermott): American Health Security Act S 703 (HR 1200) 1.Automatic enrollment 2.Comprehensive benefits 3.Operated by States using Federal standards 4.Free choice of doctor and hospital 5.Doctors and hospitals remain independent 6.Public agency processes and pays bills 7.Financed through payroll taxes
: American Health Security Act S 703 (HR 1200) 1.Automatic enrollment 2.Comprehensive benefits 3.Operated by States using Federal standards 4.Free choice of doctor and hospital 5.Doctors and hospitals remain independent 6.Public agency processes and pays bills 7.Financed through payroll taxes")
55
IN CONCLUSION A system based on private insurance plans - will not lead to universal coverage - will not create affordable insurance A Medicare for All System - can lead to universal comprehensive coverage, without costing more - has the greatest potential to increase choice, improve quality and expand primary care - can be financed fairly

56
We Can’t Wait Another 16 Years! We Need Real Health Care Reform Before the Premium Takes All our Income! Source: American Family Physician, November 14, 2005 Today

57
CONTACTS AND REFERENCES PNHP National: www.pnhp.org PNHP-NY Metro: www.pnhpnymetro.org Bodenheimer TS, Grumbach K, Understanding Health Policy: A Clinical Approach. McGraw-Hill, 2005 Fein O, Birn AE. (editors), Comparative Health Systems. Am Jour Public Health 2003; 93: 1-176 O’Brien ME, Livingston M (editors), 10 Excellent Reasons for National Health Care. New Press, 2008 Potter W, Deadly Spin: An Insurance Company Insider Speaks Out on How Corporate PR Is Killing Health Care and Deceiving Americans. Bloomsbury Press, 2010
, Comparative Health Systems. Am Jour Public Health 2003; 93: O’Brien ME, Livingston M (editors), 10 Excellent Reasons for National Health Care. New Press, 2008 Potter W, Deadly Spin: An Insurance Company Insider Speaks Out on How Corporate PR Is Killing Health Care and Deceiving Americans. Bloomsbury Press,")
Similar presentations








 Prepared by Randy Block Co-Chair, Gray Panthers of Metro Detroit.>")



 implements broad, historic changes to U.S. health care Expanded access to health insurance and care.>")




>")

