Download presentation
Presentation is loading. Please wait.

1
First Things First! Primary health care is the key to managing wait lists, chronic disease, and modernizing Medicare for the 21 st Century Michael M Rachlis MD MSc FRCPC Southey SK March 3, 2010 www.michaelrachlis.com

2
Outline Where are we now? How did we get here? We could fix almost all Medicare’s problems with innovation and quality – the Second Stage of Medicare Primary health care reform is the key to health reform

3
Where are we now? Southey

4
Medicare View #1: Globe and Mail We established Medicare when we were young, healthy, and altruistic. The economy was growing rapidly. It worked pretty well then. Now we are old, sick, and the economy is stagnant. Medicare doesn't work very well. Wait lists go from the North Pole to the US border. Health care costs are going through the roof. The public sector is too inefficient to make it work. We now have to ‘be cruel to be kind’. We should allow some privatization of finance and profitization of delivery to 'save' Medicare.

5
Medicare View #2: Toronto Star At the beginning, the federal government paid half the bills and everything worked pretty well. The Federal government gave up 50-50 cost sharing in 1977, and then hacked funding until 1997. Medicare was starved. This led to service erosion, privatization of finance, and increased use of for profit delivery. Now we need more public money, more enforcement of the Medicare legislation, and curbs on for profit delivery to save Medicare.

6
Medicare View #3: National Post Medicare was always a bad idea. Health care costs are out of control. But a government run health system is like the Beverly Hillbillies trying to run IBM. Despite huge costs, services are terrible. It’s not too late to do the right thing. Let’s privatize and profitize as fast as possible. Maybe a dumb, rich American will buy it.

7
What do Canadians want to hear? Medicare was the right road to take Resources aren’t the problem Medicare was designed for another time and was implemented as a compromise Canadians overwhelming support public sector solutions to Medicare's problems And, there are public sector solutions – Tommy Douglas’s 2 nd Stage of Medicare

8
Medicare was the right road

9
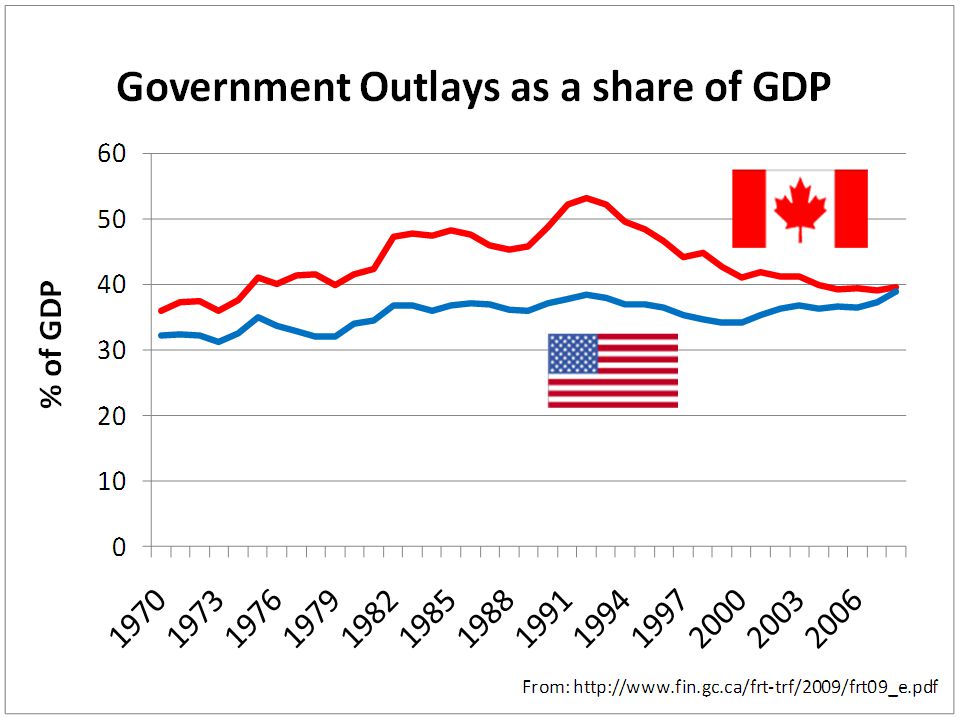
Canada vs. the US: No contest! All Canadians are covered but 47 million Americans are uninsured, and tens of millions more are under-insured Canada spends much less than the US Canadians get only slightly fewer services overall Canadian outcomes are as good or better Canadians live 3 years longer than Americans and our infant mortality rate is 20% lower. Single payer insurance boosts Canadian business – Health care costs are 1.5% of Canadian manufacturers’ payrolls vs. 9% in the US

11
S Woolhandler Int J H Serv 2004;34:65-78.

12
Canadian health care outcomes on average are as good, or better than those in the US Guyatt et al 2007 published an overview of individual studies comparing US and Canadian health care. They concluded that overall Canadian care was as good or superior to US care. See: http://www.openmedicine.ca/article/view/8/1 http://www.openmedicine.ca/article/view/8/1

14
What do Canadians want to hear? Medicare was the right road to take Resources aren’t the problem Medicare was designed for another time and was implemented as a compromise Canadians overwhelming support public sector solutions to Medicare's problems And, there are public sector solutions – Tommy Douglas’s 2 nd Stage of Medicare

18
What do Canadians want to hear? Medicare was the right road to take Resources aren’t the problem. Medicare was designed for another time and was implemented as a compromise Canadians overwhelming support public sector solutions to Medicare's problems And, there are public sector solutions – the 2 nd Stage of Medicare

19
Canadian Medicare was designed for another time and was a compromise 1.Medicare was designed for acute illness and Canada’s acute care system compares well internationally 2.But now the main problems are chronic diseases and Canada does poorly with these and with waits and delays. 3.Political compromise has slowed the development of better delivery models since the 1960s and the implementation of the “quality agenda” more recently

20
Chronic disease: Big problems 60% of people with diabetes have gone more than a year without an eye exam. More than 50% of type 2 diabetics are not at recommended blood glucose targets. Less than 50% of type 2 diabetics are tested for A1c levels, blood pressure, cholesterol, or kidney function. Ontario Quality Improvement and Innovation Partnership 2009

21
21 Practices with Advanced Electronic Health Information Capacity Source: 2009 Commonwealth Fund International Health Policy Survey of Primary Care Physicians. %

22
22 % Practice Routinely Receives and Reviews Data on Patient Outcomes Source: 2009 Commonwealth Fund International Health Policy Survey of Primary Care Physicians

23
23 Time Spent Reporting or Meeting Regulations is a Major Problem Source: 2009 Commonwealth Fund International Health Policy Survey of Primary Care Physicians %

24
We could prevent most chronic diseases > 80% of ischemic heart disease, lung cancer, chronic lung disease, and diabetes cases could theoretically be prevented with what we know now This would free up over 6000 hospital beds across Canada

26
Canada Has Big Quality Problems -- mainly similar to those of other countries Misuse – 5-10% of deaths in developed countries are preventable hospital deaths Overuse – Medication and the elderly Under use – Chronic disease management and prevention – Cervical and breast cancer screening

27
Do one-fifth of older Canadian women need to take sedatives? Do we care what we’re paying for?

28
[Green et al Soc Sci Med 2003; 57:553-60]
![[Green et al Soc Sci Med 2003; 57:553-60]](http://images.slideplayer.com/20/5955027/slides/slide_28.jpg "[Green et al Soc Sci Med 2003; 57:553-60]")
29
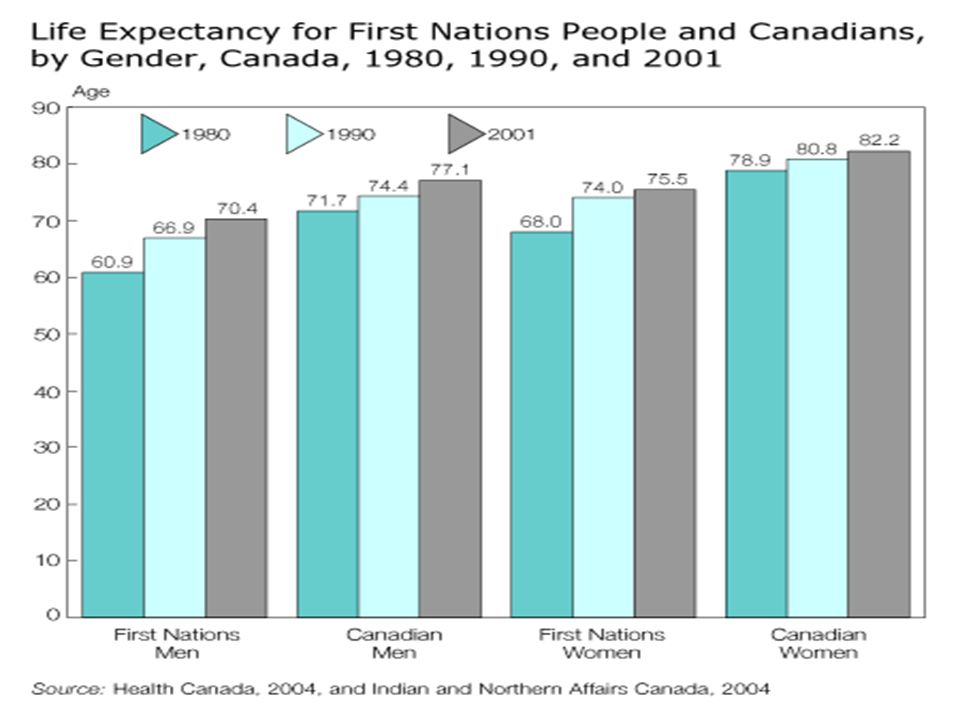
We don’t have equal access to health Men live 5 years less than women Women have more chronic, non-fatal conditions Aboriginal men live 7 years less than other men Poor men live 5 years less than rich men Infant mortality is 70% higher in poor neighbourhoods than rich neighbourhoods Northern Canadians have the shortest lives

31
Disparities in health between different groups are responsible for 20% of health care costs Health Disparities Task Group of the Federal Provincial Territorial Advisory Committee on Population Health and Health Security. Health Disparities: Roles of the Health Sector. 2004. http://www.phac-aspc.gc.ca/ph- sp/disparities/pdf06/disparities_discussion_paper_ e.pdf http://www.phac-aspc.gc.ca/ph- sp/disparities/pdf06/disparities_discussion_paper_ e.pdf

32
Quality workplaces for providers Happier staff = healthier patients Happier staff = lower turnover Healthier patients = lower costs Lower turnover = lower costs

33
Swift Current Region Saskatchewan

34
The original vision for Medicare -- Swift Current, Saskatchewan 1945 Prepaid funding Services available on a universal basis, with little or no charge to users. Integrated health care delivery with acute care, primary care, home care, and public health. Group medical practice with doctors working in teams with other providers. Overall public health view of the system. Democratic community governance of health care delivery by local boards.

35
What happened to the vision? Despite the Swift Current Region’s success, Saskatchewan MDs didn’t want to bargain with anyone but the province Saskatchewan MD strike of 1962

36
What happened to the vision? The federal government only covered hospital and medical care leaving coverage incomplete Despite the 1972 Hastings’s Report recommendations for re-organizing the system around prevention, new models of care are slow to develop 1990s cutbacks harm a vulnerable system Waits and delays worsen There’s less national vision every day Notwithstanding, reforms are being implemented in some places and have made significant improvement in outcomes and efficiency

37
What do Canadians want to hear? Medicare was the right road to take Resources aren’t the problem. Medicare was designed for another time and was implemented as a compromise Canadians overwhelming support public sector solutions to Medicare's problems And, there are public sector solutions – Tommy Douglas’s 2 nd Stage of Medicare

39
What do Canadians want to hear? Medicare was the right road to take Resources aren’t the problem. Medicare was designed for another time and was implemented as a compromise Canadians overwhelming support public sector solutions to Medicare's problems And, there are public sector solutions – Tommy Douglas’s 2 nd Stage of Medicare

40
Medicare’s problems are due to the failure to re-tool an ineffective and inefficient delivery system 20 litres/100 km5 litres/100km

41
Good News! We could improve care for chronic disease The Sault Ste Marie Group Health Centre has had an electronic record since 1997 and uses it to continuously improve the care of over 5000 patients with diabetes.

42
Good News! We could access primary health care within 24 hrs “Even if we did nothing else, and we should implement other reforms, if every family physician implemented Advanced Access, every Canadian could have a family doctor.” Penticton British Columbia’s Dr. Jeff Harries to the CMA meeting, “ Taming the Queue”. Ottawa. March 31, 2006

43
Good News! We could have elective specialty consultations within one week – The Hamilton Family Medicine Mental Health Program increased access for mental health patients by 1100% while decreasing psychiatry outpatients’ clinic referrals by 70%. – The program staff includes 150 family doctors, 80 mental health counsellors, and 17 psychiatrists and provides care to 300,000 patients

44
Good News! We could have elective surgery within two months – In Toronto, Barrie, and other parts of Ontario arthritis patients are assessed within two weeks for joint replacements and have their surgery within two months

45
Going for gold: Re-engineering services to immigrants in Toronto Access Alliance works with immigrant and refugee communities to identify women who are leaders and hires them as community health workers (CHWs) They are given 3 months of paid training and 3 year contracts The CHWs run educational workshops and facilitate well children and well women care CHWs have brought services to more than 12,000 women and their children 85% of CHWs get jobs in health or social services after their contracts are over 45
 They are given 3 months of paid training and 3 year contracts The CHWs run educational workshops and facilitate well children and well women care CHWs have brought services to more than 12,000 women and their children 85% of CHWs get jobs in health or social services after their contracts are over 45")
46
Going for Platinum: Population Health Planning in Saskatoon, Saskatchewan

48
“I am concerned about Medicare – not its fundamental principles -- but with the problems we knew would arise. Those of us who talked about Medicare back in the 1940’s, the 1950’s and the 1960’s kept reminding the public there were two phases to Medicare. The first was to remove the financial barrier between those who provide health care services and those who need them. We pointed out repeatedly that this phase was the easiest of the problems we would confront.” Tommy Douglas 1979 Catching Medicare’s second stage

49
“The phase number two would be the much more difficult one and that was to alter our delivery system to reduce costs and put and emphasis on preventative medicine…. Canadians can be proud of Medicare, but what we have to apply ourselves to now is that we have not yet grappled seriously with the second phase.” Tommy Douglas 1979

50
The Second Stage of Medicare is delivering health services differently to keep people well

51
Canada’s health policy is in evolution from a 19 th century passive insurance program for 18 th century professional practice to a public health program based upon high performing, patient- centred, team-based care

52
First things first! Primary health care reform is the key to health reform

53
Why is integrated primary health care so important? Canada has problems with access, chronic disease management and prevention, and population health Primary health care is the key for access, chronic disease management and prevention, and population health Primary health care = sustainability

54
A population health strategy focuses on factors that enhance the health and well-being of the overall population. It views health as an asset that is a resource for everyday living, not simply the absence of disease. Population health concerns itself with the living and working conditions that enable and support people in making healthy choices, and the services that promote and maintain health. From Strategies for Population Health 1994 FPT Advisory Committee on Population Health

55
Primary health care and population health Can the health system engage with communities? South Riverdale gets the lead out Regent Park’s Pathways to Education reduced its high school dropout rate from 56% to 14% Montreal PHC dealt with its Ice Storm Ottawa PHC dealt with influenza Saskatoon CC and the downtown Westside 55

56
What are the barriers to better primary health care linkages? Definitions do matter – They reflect different visions and values for Medicare and health care delivery. – Is health care largely a public good or is it largely a private commodity? Integration of physicians – Physician payment

57
“PHC is essential health care made universally accessible to the community by means acceptable to them, through their full participation and at a cost that the community and the country can afford....it is the first level of contact of individuals, the family and community within the national health system … and constitutes the first element of a continuing health care process...PHC addresses the main health problems in the community, providing promotive, preventive, curative, supportive and rehabilitative services accordingly.“ (World Health Organization 1978)
")
58
“Primary health care represents the first point of contact for individuals with the health care system, and is the key to efficient, timely, quality family and community care based on continuity and coordination, early detection and action, and better information on needs and outcomes.” First Ministers’ Accords; 2000, 2003, 2004

59
Declaration of Montevideo 2005 (http://www.paho.org/english/gov/cd/CD46-decl-e.pdf)http://www.paho.org/english/gov/cd/CD46-decl-e.pdf Approved by all countries in Pan American Health Organization PHC should be integrated into health systems – Not implemented as a separate program Commitment to social inclusion and equity Recommendations to strengthen community participation and oversight of PHC

60
What are the facilitators for primary health care reform? Engagement of the rest of the health care system including public health Engagement of communities

61
What are the facilitators for primary health care reform? Engagement with MDs – At all levels – Quality Improvement initiatives – Family physician divisions? Physician payment reform – Salary – Capitation – Blended systems

62
Trying to deliver health services without adequate primary health care is like pulling your goalie in the first period!

63
“Only through the practice of preventive medicine will we keep the costs from becoming so excessive that the public will decide that Medicare is not in the best interests of the people of the country.” Tommy Douglas

64
Summary: Canada’s health system out-performs the US but our health services are rife with problems because we forgot the 2 nd Stage of Medicare We could fix almost all Medicare’s problems with innovation– the 2 nd Stage of Medicare We need to implement the 2 nd Stage of Medicare or we risk losing the First Primary health care reform is the key to health reform and the 2 nd stage of Medicare

65
Courage my Friends, it is Not Too Late to Make a Better World! Tommy Douglas

Similar presentations