Download presentation
Presentation is loading. Please wait.

1
SLEEP DISORDERED BREATHING/ OBSTRUCTIVE SLEEP APNEA JHANSI NALAMATI MD

2
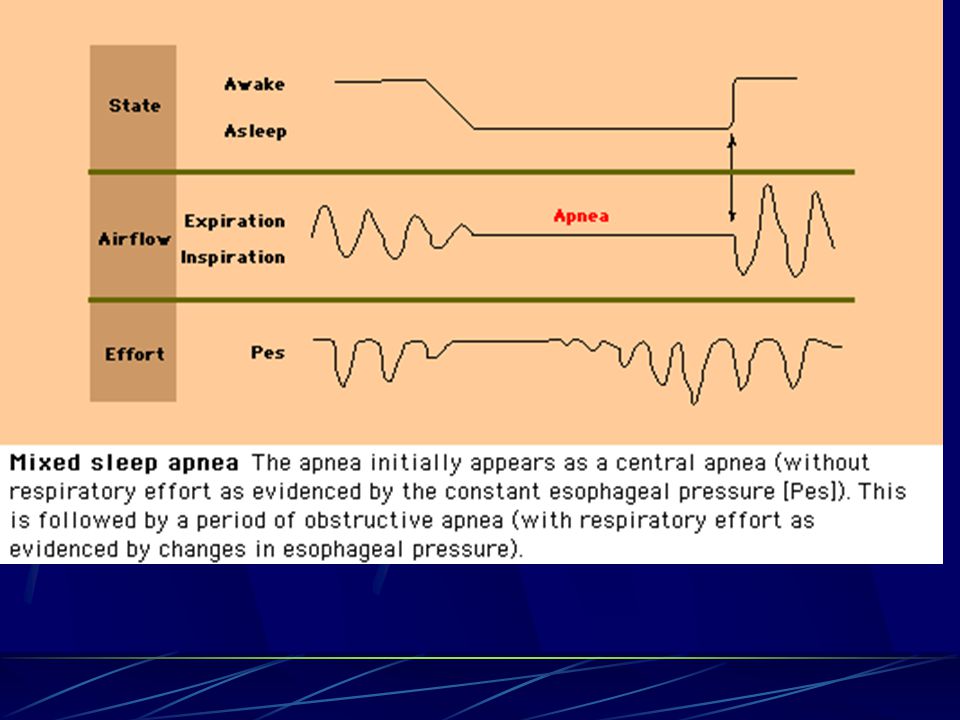
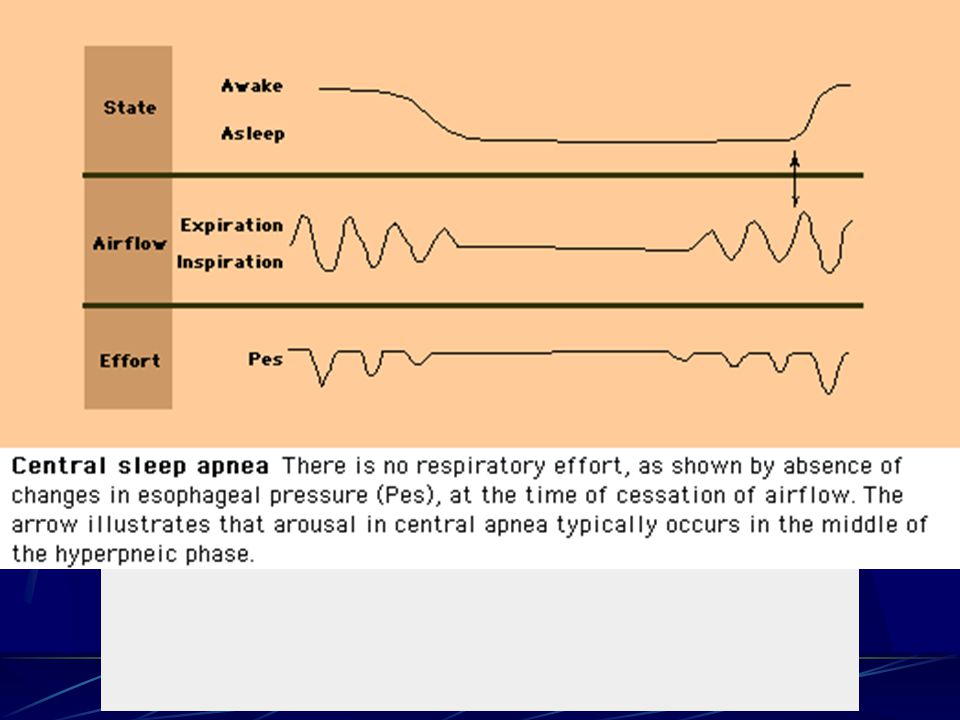
TYPES Obstructive Sleep Apnea Central Sleep Apnea Mixed Apnea Upper Airway Resistance Syndrome (UARS)
")
6
Historical background Apnea- literally means “without breath” Pickwickian papers fat boy “Joe” Osler and later Burwell applied the name “Pickwickian Syndrome” to patients with Obesity, Hypersomnolence and signs of Chronic hypoventilation

7
Historical (contd.) Sleep apnea -Rediscovered by Gestaut and co- workers in 1965 by simultaneously recording sleep and breathing in a “Pickwickian” patient and described all 3 types of apnea. Postulated that sleepiness is due to repetitive arousals associated with resumption of breathing that terminated the apneic events.

8
Historical(contd.) First description of successful Tx of OSA by tracheostomy followed in 1969. First Tx with CPAP – in 1980’s soon after NIPPV was described by Charles Collins of Australia

9
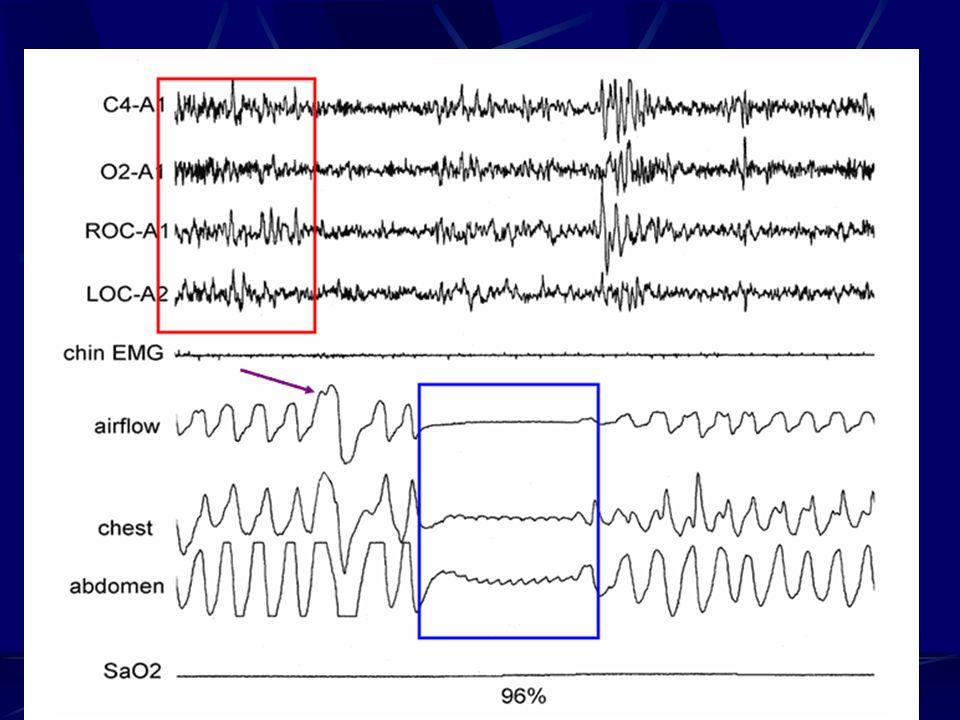
Definition of Apnea Apnea-Cessation of breathing(air flow) for 10 seconds Hypopnea- decreased in the airflow by 30-50%, and associated with an arousal and a drop in oxygen desaturation by 3- 4%
 for 10 seconds Hypopnea- decreased in the airflow by 30-50%, and associated with an arousal and a drop in oxygen desaturation by 3- 4%")
10
Prevalence 9% of men and 4% of women, in one study of state employees had AHI of 15 events/hr 12 million people in the US have OSA

11
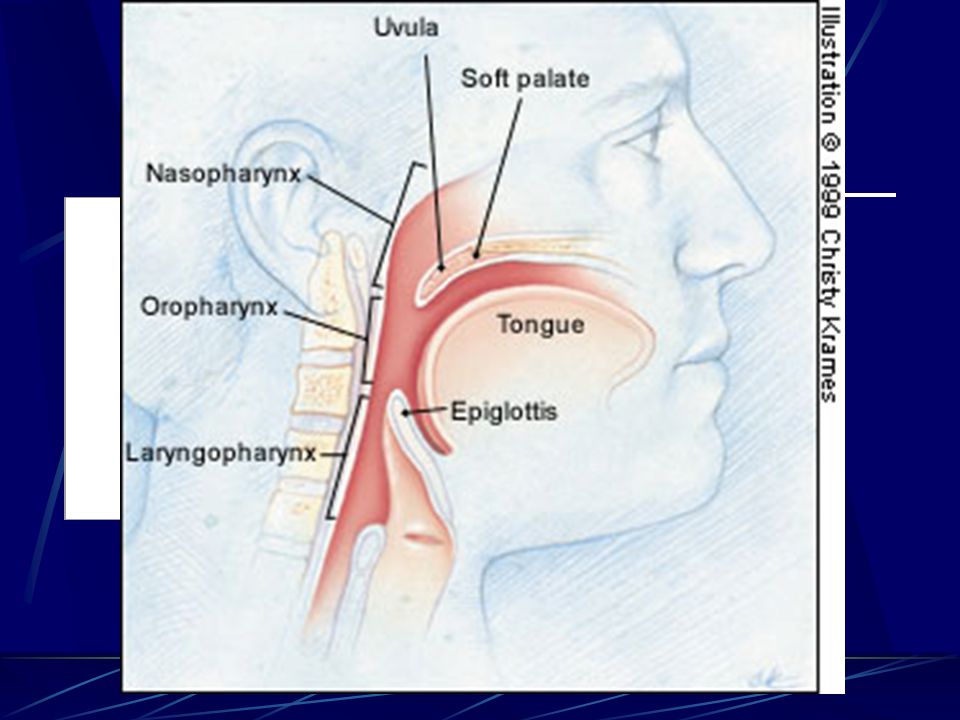
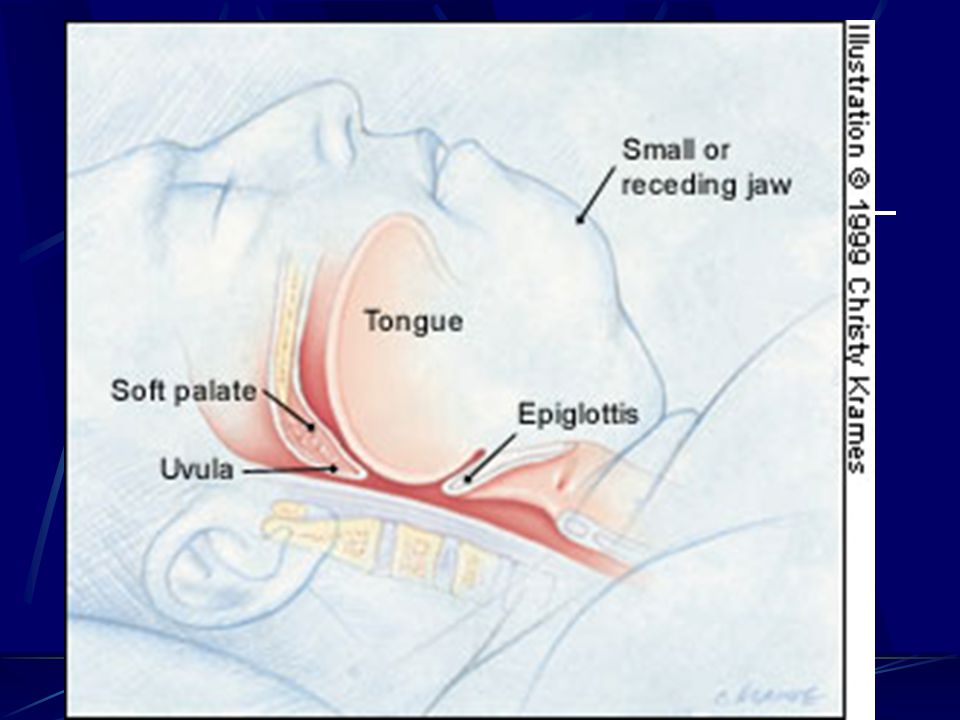
Pathophysiology Pharynx is abnormal in size or collapsibility. As an organ for speech and deglutition it must be able to change shape and close As a conduit for airflow it must resist collapse

12
Pathophysiology(contd.) Exact mechanism is not known During the day muscles in the region keep the airway open During sleep muscles relax to a point where the airway collapses to an extent that it gets obstructed Once breathing stops, individual awakens to breathe and arousal can last few seconds to a minute
 Exact mechanism is not known During the day muscles in the region keep the airway open During sleep muscles relax to a point where the airway collapses to an extent that it gets obstructed Once breathing stops, individual awakens to breathe and arousal can last few seconds to a minute")
15
Risk factors for OSA Obesity Age- middle aged men and post- menopausal women Older age- due to loss of muscle mass and tone ? Family Hx of OSA

16
Risk factors (contd.) Anatomic abnormalities- receding chin, ?Nasal congestion, ? DNS Enlarged Tonsils and adenoids esp.in children Enlarged and inflammed uvula, worsened by chronic smoking, GERD Acromegaly

17
Risk factors (contd.) Amyloidosis, post- polio syndrome, neuromuscular disorders Marfan’s syndrome, Down’s syndrome Use of alcohol and sedatives that relax the upper airway Increased neck circumference > 16 inches in women and 18 inches in men
 Amyloidosis, post- polio syndrome, neuromuscular disorders Marfan’s syndrome, Down’s syndrome Use of alcohol and sedatives that relax the upper airway Increased neck circumference > 16 inches in women and 18 inches in men")
22
Symptoms Most of the symptoms are from disruption of normal sleep architecture Excessive Daytime Sleepiness (EDS)- falling asleep even in stimulating environment, during a conversation, eating, business meeting H/O Snoring
- falling asleep even in stimulating environment, during a conversation, eating, business meeting H/O Snoring")
23
Symptoms (contd.) Non- restorative sleep Automobile Accidents Personality changes Decreased Memory Erectile Dysfunction Frequent Nocturnal Awakening
 Non- restorative sleep Automobile Accidents Personality changes Decreased Memory Erectile Dysfunction Frequent Nocturnal Awakening")
24
Symptoms(contd.) Drowsy Driver Syndrome Polyuria Early morning headache Dry mouth
 Drowsy Driver Syndrome Polyuria Early morning headache Dry mouth")
25
Signs Loud Snoring Witnessed apneas Obesity HTN Metabolic syndrome Increased Neck circumference Anatomic Abnormalities

26
SHHS Sleep heart health study- initiated by NIH in 1996 and initial data shows that treatment of SBD improved outcomes in control of HTN, CHF atherogenesis, glycemic control

27
Screening for OSA 2 of the three symptoms- EDS, loud Snoring, Witnessed Apneas High Score on ESS(Epworth Sleepiness Score)>12, or Stanford Sleepiness Score
>12, or Stanford Sleepiness Score")
28
Epworth Sleepiness Scale (ESS) Maxiumum score of 24 The scale is used to rate the 8 situations below that apply best to each individual 0-no chance of dozing 1- Slight chance of dozing 2- moderate chance of dozing 3- high chance of dozing
 Maxiumum score of 24 The scale is used to rate the 8 situations below that apply best to each individual 0-no chance of dozing 1- Slight chance of dozing 2- moderate chance of dozing 3- high chance of dozing")
29
ESS (contd.) Sitting and reading Watching television Sitting inactive in a public place ( theater, meeting) As a passenger in a car for about an hr. without break Lying down to rest in the afternoon when circumstances permit Sitting and talking to someone Sitting quietly after lunch In a car, while stopped for a few minutes in traffic

30
ESS ( contd.) 1-6 : getting enough sleep 7-9 about average and probably not suffering from Excessive daytime Sleepiness (EDS) 10 or greater- need further evaluation to determine the cause of EDS or if you have underlying sleep disorder
 1-6 : getting enough sleep 7-9 about average and probably not suffering from Excessive daytime Sleepiness (EDS) 10 or greater- need further evaluation to determine the cause of EDS or if you have underlying sleep disorder")
31
Types of Sleep Study Full night Polysomnography ( PSG) PSG with CPAP titration Split- Night Polysomnography Multiple Sleep latency test ( MST) Maintainance of wakefulness Test ( MWT)
 PSG with CPAP titration Split- Night Polysomnography Multiple Sleep latency test ( MST) Maintainance of wakefulness Test ( MWT)")
32
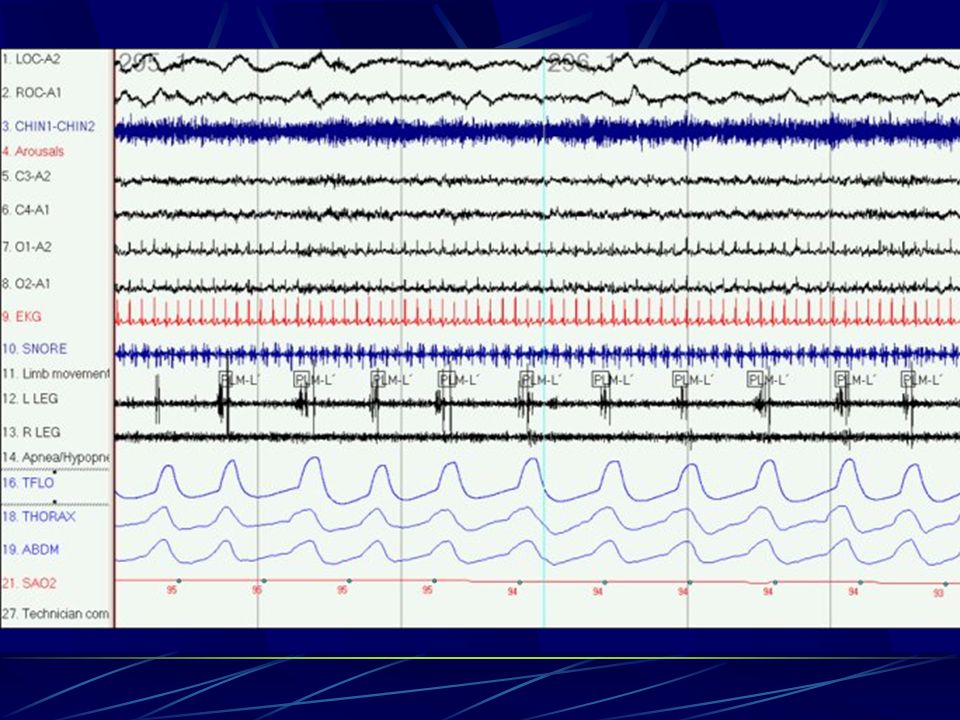
Diagnosis Nocturnal Polysomnography-in lab study, where EEG, EMG, HR, body position, leg movements, Oximetry, Snoring, abdominal and chest wall movements are recorded Home studies are limited as EEG is not recorded, or in some limited studies only Nocturnal Pulse oximetry is done

35
Definition of OSA Normal- AHI < 5 Mild OSA- AHI 5-20 Moderate OSA- AHI 20-40 Severe OSA- AHI 40-60 RDI( respiratory disturbance Index)- AHI+ RERA( Respiratory Effort Related Arousals)
- AHI+ RERA( Respiratory Effort Related Arousals)")
36
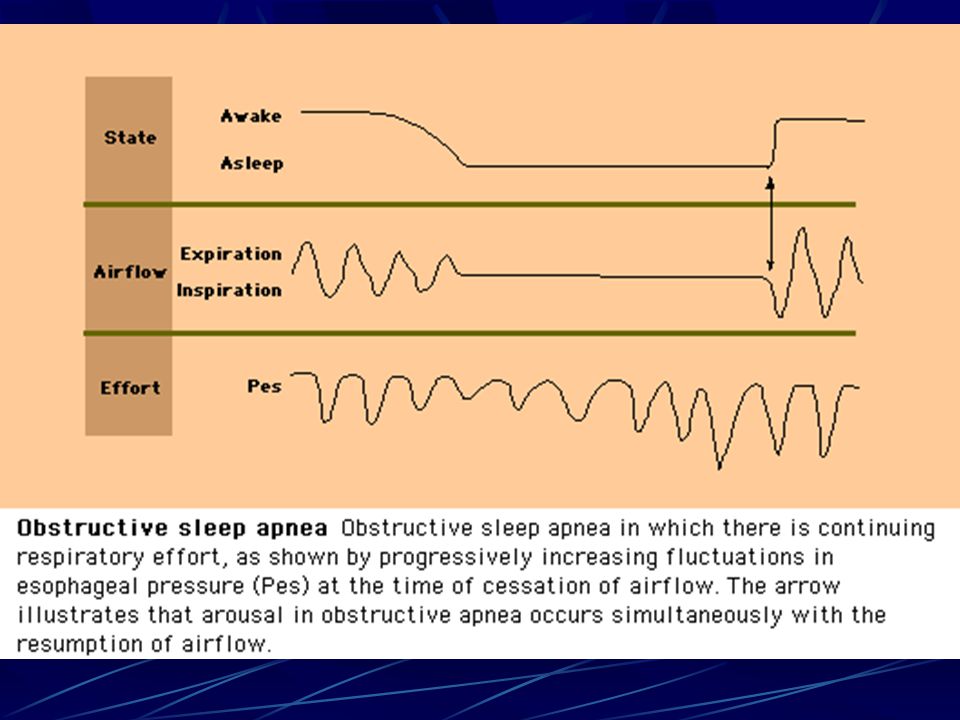
UARS Upper Airway Resistance Syndrome Cannot be diagnosed with PSG Repetitive arousals that probably result from increased Respiratory effort and high resistance in the airway Can be diagnosed by measuring esophageal pressure (Pes)
")
37
Medical Complications Uncontrolled HTN Diminished quality of life from chronic sleep deprivation Increase risk for CVA Worsening of CAD and CHF

38
Treatment Behavioral Tx- weight loss Sleep hygeine Avoiding alcohol too close to bedtime Avoid sedatives and hypnotics, narcotics Avoid caffeine

39
Treatment(contd.) Positional Tx- helpful with Primary snoring Positive Airway pressure (CPAP or BiPAP) ENT Surgery Oral appliances
 Positional Tx- helpful with Primary snoring Positive Airway pressure (CPAP or BiPAP) ENT Surgery Oral appliances")
40
Positive airway pressure Effective, Non-invasive Mask fit, air seal, comfort and humidification are important Nasal mask, full face- masks, nasal pillows, Nasal aire prongs

41
Complications of CPAP Local dermatitis Air leak, nasal congestion,rhinorrhea Dry eyes Nose bleed Aerophagia Rare- tympanic rupture, pneumothorax Compliance is the biggest issue

42
Surgery Except tracheostomy,helps only mild to moderate cases or only primary snoring Not curative for OSA Somnoplasty- office procedure- radiofrequency ablation of the soft palate- only for snoring

43
Surgery( contd.) LAUP- laser assisted uvuloplasty, only for snoring, office procedure UPPP (UP3)- (Uvulo-palato-pharyngo- plasty) Complicated surgery Patients have to observed in the hospital overnight
 LAUP- laser assisted uvuloplasty, only for snoring, office procedure UPPP (UP3)- (Uvulo-palato-pharyngo- plasty) Complicated surgery Patients have to observed in the hospital overnight")
44
UPPP(contd.) Decreases AHI by only 50% Complications include- nasal regurgitation of fluids, pharyngeal stensosis In children- tonsillectomy and adenoidectomy alone is curative
 Decreases AHI by only 50% Complications include- nasal regurgitation of fluids, pharyngeal stensosis In children- tonsillectomy and adenoidectomy alone is curative")
45
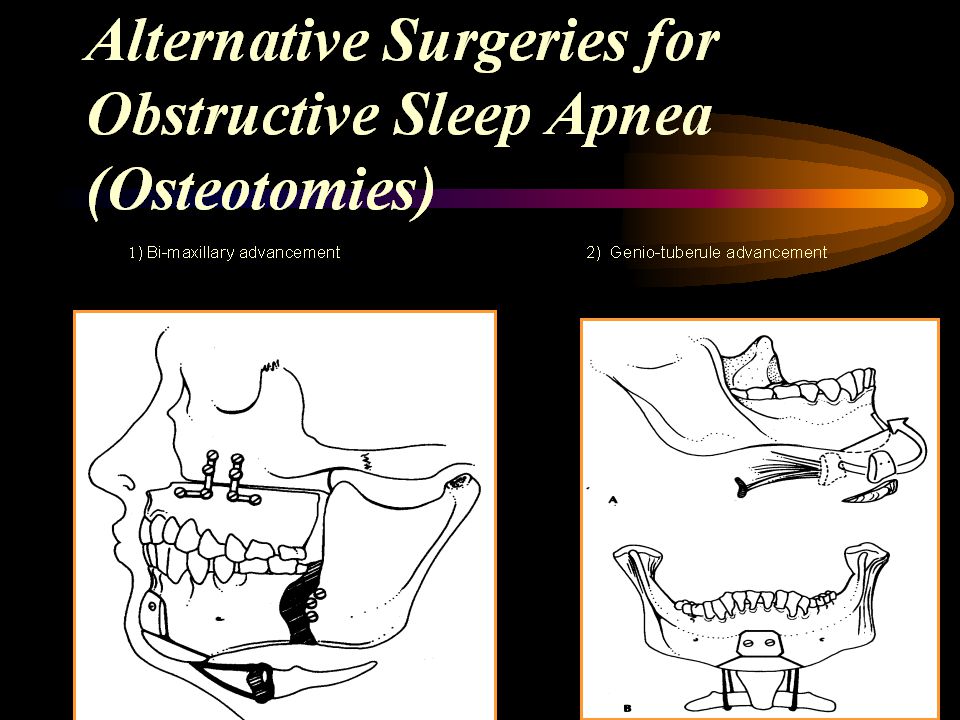
Jaw surgery Useful for retrognathia, involves partial excision of maxilla or mandible Genioplasty Complicated surgery

46
Bariatric surgery Gastric bypass Weight loss and decrease in adipose tissue of the parapharyngeal region leads to improvement or cure of OSA Weight loss has to be at least 20-30lbs before any change in AHI can be seen

47
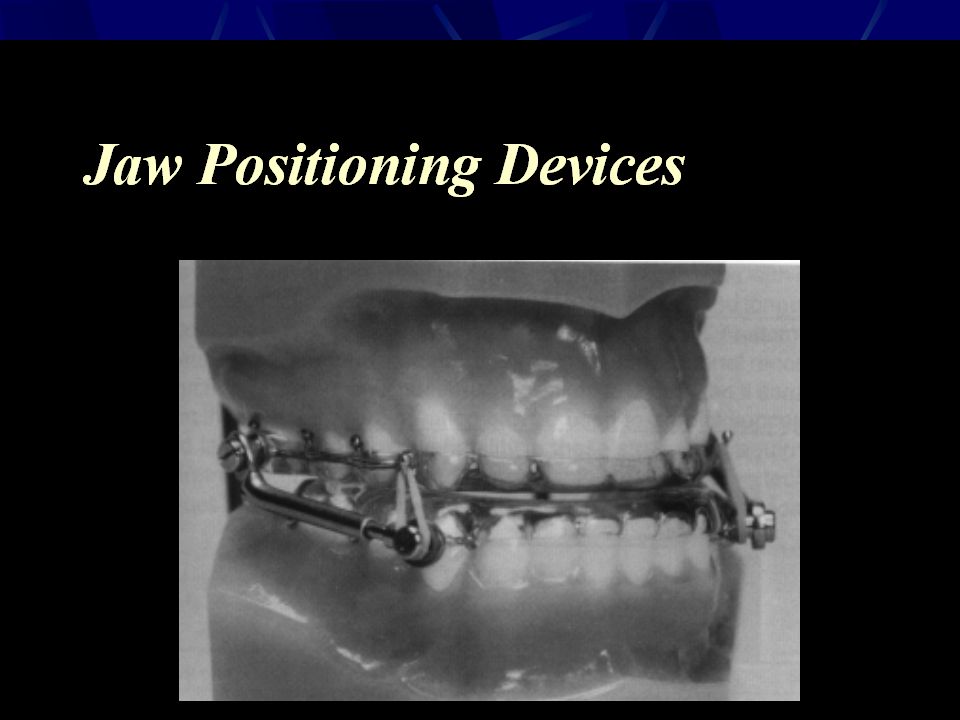
Oral appliances Devices that are worn during sleep that retract the jaw and alleviate upper airway obstruction Tongue retaining devices for people with macroglossia

52
CPAP Therapy Positive impact on subjective sleepiness and depression (in RCTs) Fatigue, generic health related quality of life, vigilance, driving performance are all improved ( prospective trials) These parameters are sensitive to Tx duration and compliance
 Fatigue, generic health related quality of life, vigilance, driving performance are all improved ( prospective trials) These parameters are sensitive to Tx duration and compliance")
53
Commercial driving and OSA OSA has to be effectively treated before clearing the patient for work Objective documentation of regular CPAP use and testing by Multiple sleep latency test and/or MWT( Maintainance of Wakefulness Test)
")
Similar presentations









 is a sleeping disorder that causes a person to stop breathing for a span of seconds In OSA, the airway.>")

 286-7455 Fax: (703) 286-7462.>")




 Necessary for Physical and Mental Health $50 Billion / Year in Lost Productivity Occupies 1/3 of our Lives.>")







