Download presentation
Presentation is loading. Please wait.

1
Post G.I. ASCO Update: Colorectal Cancer Ronald Burkes, M.D.

2
Disclosure of Potential Conflicts of Interest Dr. Ronald Burkes Amgen Inc., Eli Lilly and Company, Hoffmann-La Roche, AstraZeneca, Sanofi- Aventis Advisory board: Honoraria:Amgen Inc., Eli Lilly and Company, Hoffmann-La Roche, AstraZeneca, Sanofi-Aventis Speaker:Amgen Inc., Eli Lilly and Company, Hoffmann-La Roche, AstraZeneca

3
Objective(s) Review what was new and interesting from G.I. ASCO, 2012 Put these results in perspective Studies to be reviewed: 181 study – FOLFIRI +/- Panitumumab as 2 nd -line treatment of mCRC NCIC CO.20 study – Cetuximab +/-Brivanib in KRAS WT mCRC (3 rd -line) CORRECT trial – BSC +/- Regorafenib in mCRC (4 th -line) XELOXA trial (N016968) – role of adjuvant XELOX for stage III CRC ACCORD 12 trial – Capox in rectal cancer Assessment of the prognostic and predictive value of mutant KRAS codons 12 & 13
 CORRECT trial – BSC +/- Regorafenib in mCRC (4 th -line) XELOXA trial (N016968) – role of adjuvant XELOX for stage III CRC ACCORD 12 trial – Capox in rectal cancer Assessment of the prognostic and predictive value of mutant KRAS codons 12 & 13.")
12
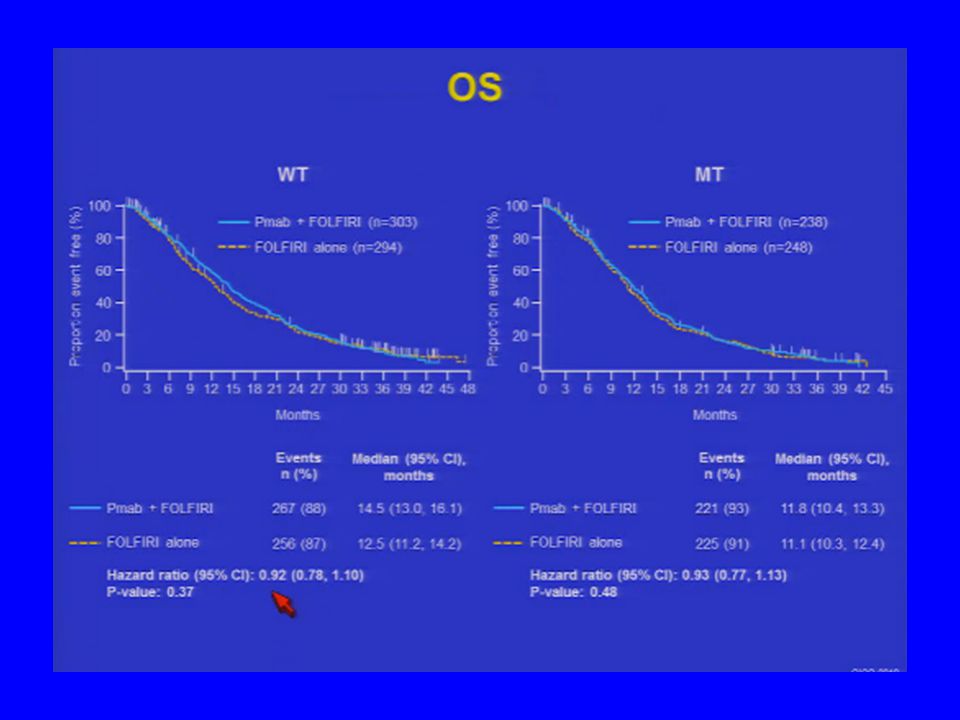
FOLFIRI +/- Panitumumab as 2 nd -line Therapy of mCRC: 181 study Sobrero GI ASCO (#387), 2012 FOLFIRI + P 303 FOLFIRI 284 HR/p-value RR36%9.8% PFS (mos)6.74.9.82/.023 OS (mos)14.512.5.92/.37 Post Rx EGFR MoAb 12%34% OS (mos) by ST (2-4 vs 0-1) 16.4 vs 8.412.7.5 vs 1.48
, 2012 FOLFIRI + P 303 FOLFIRI 284 HR/p-value RR36%9.8% PFS (mos) /.023 OS (mos) /.37 Post Rx EGFR MoAb 12%34% OS (mos) by ST (2-4 vs 0-1) 16.4 vs vs 1.48")
13
Comments: 181 Final analysis is consistent with the primary analysis There is an improvement in PFS and RR but not OS Not likely to be used as a 2 nd -line option since no OS but may be appropriate for some pts when response is necessary (? still potentially resectable) Rash/efficacy interaction seems to be important, but not well understood The inability to mount a skin reaction to an anti- EGFR antibody seems to be associated with a shorter survival → what should we do with patients who don’t develop a rash (should they stop the anti-EGFR MoAb) ?
 Rash/efficacy interaction seems to be important, but not well understood The inability to mount a skin reaction to an anti- EGFR antibody seems to be associated with a shorter survival → what should we do with patients who don’t develop a rash (should they stop the anti-EGFR MoAb) .")
15
Brivanib – anti-VEGFR2 inhibitor and also targets fibroblast growth receptors

25
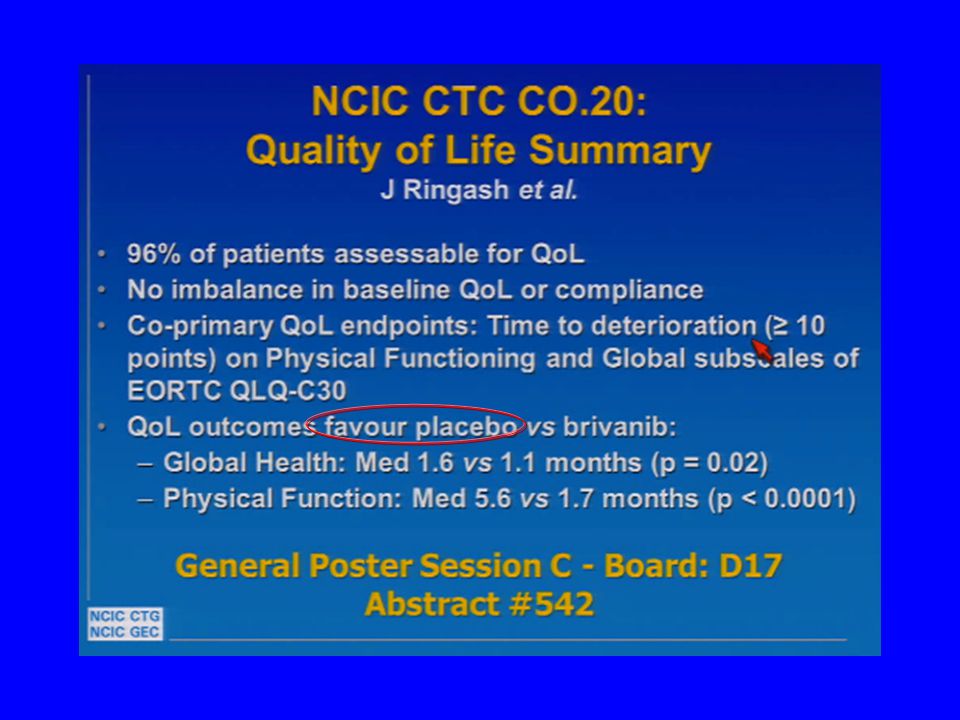
Cetuximab +/- Brivanib in Refractory KRAS WT mCRC: NCIC CO.20 Siu GI ASCO (#386), 2012 Cetux + Ber 376 Cetux + Pl 374 HR/p-value OS (mos)8.88.1.88/.12 PFS (mos)53.4.72/<.0001 RR13.6%7.2%.004 DI cetux57%83% AEs (gr3/4)78%53% D/C Cetux/Br8%/22%4%/3%
, 2012 Cetux + Ber 376 Cetux + Pl 374 HR/p-value OS (mos) /.12 PFS (mos) /<.0001 RR13.6%7.2%.004 DI cetux57%83% AEs (gr3/4)78%53% D/C Cetux/Br8%/22%4%/3%")
26
Comments: CO.20 PFS and RR benefit but no OS benefit (primary endpoint!) → no significant x-over Toxicity of the combination may have confounded efficacy → DI; D/C Rx 2 0 AEs Potential biological antagonism → PACCE and CAIRO-2 Unlikely to gain regulatory approval and/or use in combination with cetuximab Phase III HCC monotherapy trials are ongoing
 → no significant x-over Toxicity of the combination may have confounded efficacy → DI; D/C Rx 2 0 AEs Potential biological antagonism → PACCE and CAIRO-2 Unlikely to gain regulatory approval and/or use in combination with cetuximab Phase III HCC monotherapy trials are ongoing")
30
NB: no PS 2 patients on study

37
BSC +/- Regorafinib in Refractory mCRC: CORRECT Trial (no PS2, no x-over) Grothey GI ASCO (#385), 2012 Regorafinib 505 BSC 255 HR/p-value KRAS mut54.1%61.6% MST (mos)6.45.77/.0052 PFS (mos)1.91.7.49/<.00001 RR/DCR1%/44.8%.4%/15.3%p<.000001 Toxicity H/F, ↑BP, Diarrhea D/C 2 0 AEs8.2%1%
 Grothey GI ASCO (#385), 2012 Regorafinib 505 BSC 255 HR/p-value KRAS mut54.1%61.6% MST (mos) /.0052 PFS (mos) /< RR/DCR1%/44.8%.4%/15.3%p< Toxicity H/F, ↑BP, Diarrhea D/C 2 0 AEs8.2%1%")
38
Comments: CORRECT OS and PFS benefit –Statistically significant –Clinically meaningful –Toxicity profile not insiginificant (H/F, diarrhea, fatigue, ↑BP) but acceptable –Lack of x-over helped achieve endpoints Clinical impact –Likely to become an available standard for refractory mCRC – when??? (unmet need) –Role in PS 2 patients is unknown –Role of continuous dosing is unknown
 –Role in PS 2 patients is unknown –Role of continuous dosing is unknown.")
46
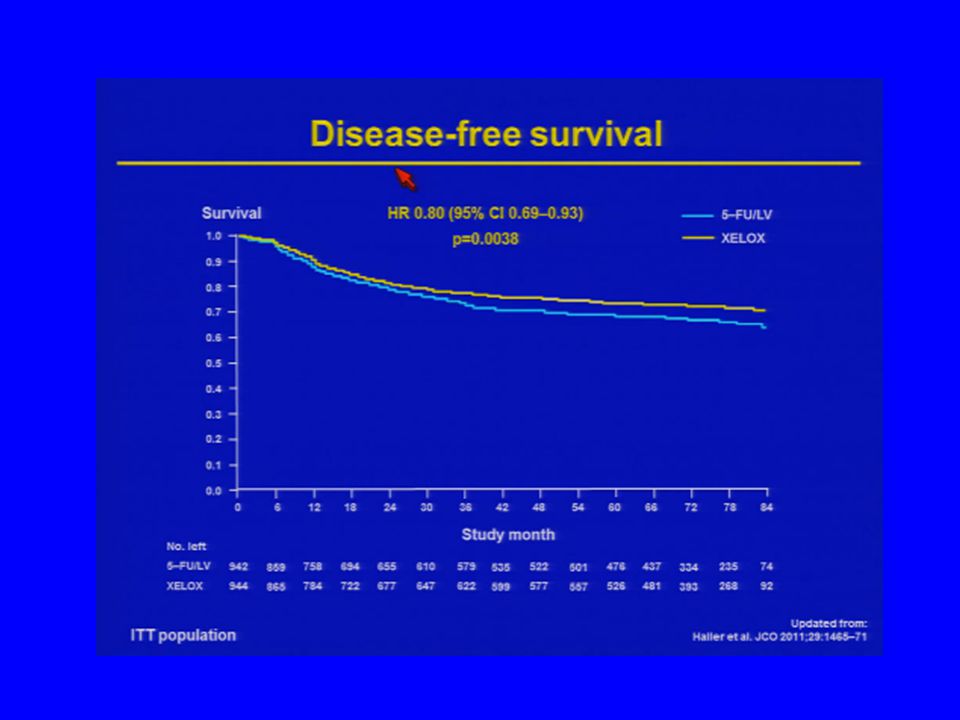
X-ACT vs XELOXA CapeMayoHR/pBolusXeloxHR/p N1004983942944 DFS60.8%56.7%.88/<.0001(.068)59.8%66.1%.8/.0038 OS71.4%68.4%.86/<.0001(.06)70%75%.83/.038 X-ACTXELOXA Twelves GI ASCO (#274), 2008
59.8%66.1%.8/.0038 OS71.4%68.4%.86/<.0001(.06)70%75%.83/.038 X-ACTXELOXA Twelves GI ASCO (#274), 2008")
50
Comments: XELOXA XELOX improves DFS and OS compared to bolus 5-FU in patients with stage III colon cancer (median follow-up of 7 years) Benefit is less in patients > 70 years XELOX should be considered a treatment option in the adjuvant therapy of stage III colon cancer q3weeks less infusion time (impact on chemo unit) less need for central lines it is not for everyone – keep a close watch for toxicity
 Benefit is less in patients > 70 years XELOX should be considered a treatment option in the adjuvant therapy of stage III colon cancer q3weeks less infusion time (impact on chemo unit) less need for central lines it is not for everyone – keep a close watch for toxicity")
56
Capecitabine + RT(45) vs Capox + RT (50) in Rectal Cancer: ACCORD 12 Trial Gerard GI ASCO (#389), 2012 Cape 45 299 Capox 50 299 DFS (3 yrs)68.3%73.7% OS (3 yrs)87.6%88.3% pCR13.9%19.2% Local recurrence6.1%4.7% Systemic recurrence25%21% Diarrhea gr ¾11%25%
 vs Capox + RT (50) in Rectal Cancer: ACCORD 12 Trial Gerard GI ASCO (#389), 2012 Cape Capox DFS (3 yrs)68.3%73.7% OS (3 yrs)87.6%88.3% pCR13.9%19.2% Local recurrence6.1%4.7% Systemic recurrence25%21% Diarrhea gr ¾11%25%")
57
Comments: ACCORD 12 This study introduced 3 changes to the approach to the pre-operative therapy of rectal cancer Oxaliplatin increases toxicity (diarrhea) without any significant impact on ypCR (not a radiosensitizer), local or systemic recurrences, DFS and OS 50Gy/5 weeks compatible with surgery and also increased the CRM negative rate Capecitabine has the same activity as 5-FU
 without any significant impact on ypCR (not a radiosensitizer), local or systemic recurrences, DFS and OS 50Gy/5 weeks compatible with surgery and also increased the CRM negative rate Capecitabine has the same activity as 5-FU")
66
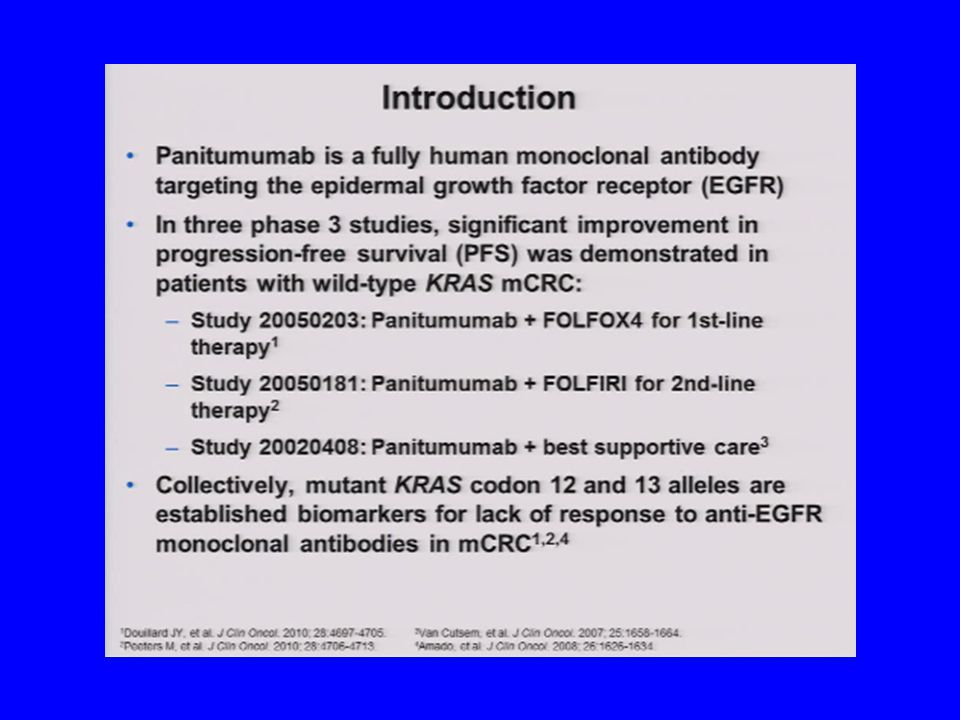
Comments: KRAS Mutation Analysis in mCRC Peeters GI ASCO (#383), 2012 Patients with mCRC that harbor most of the common codon 12 and 13 mutant KRAS alleles are unlikely to benefit from panitumumab therapy Currently only mCRC patients with WT KRAS tumors should be treated with anti-EGFR MoAbs
, 2012 Patients with mCRC that harbor most of the common codon 12 and 13 mutant KRAS alleles are unlikely to benefit from panitumumab therapy Currently only mCRC patients with WT KRAS tumors should be treated with anti-EGFR MoAbs")
Similar presentations














































 vs FOLFIRI plus bev>")




 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")






 treated with FOLFIRI with or without cetuximab:>")



adjuvant chemo-radiotherapy for locally advanced rectal cancer: Long term results.>")
 for 6 cycles followed by XELOX plus BEV or single agent (s/a) BEV as maintenance therapy in.>")
