Download presentation
Presentation is loading. Please wait.

1
Dr.Juan A.Venter Dept. Clinical Imaging Sciences Bloemfontein Academic Hospitals 18/05/2012

4
Most common of all metabolic bone disorders Significant morbidity(50% for hip fractures) and mortality(20% for hip fractures in 1 year) Treatment cost in Europe : 75 billion Euros by 2050. Lifetime Osteoporotic Fracture Risk(Caucasian) Woman- 40% Men - 20% Preventive therapies available.
 Woman- 40% Men - 20% Preventive therapies available..")
5
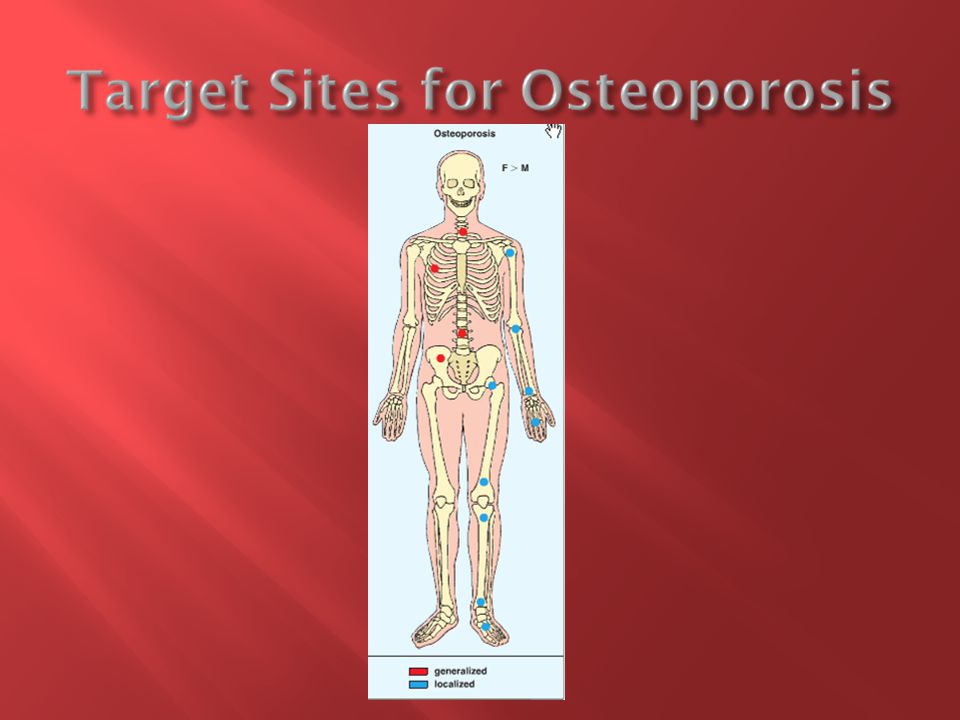
Systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue with a consequent increase in bone fragility and susceptibility to fracture which usually involves the wrist,spine, hip, pelvis,ribs or humerus.

10
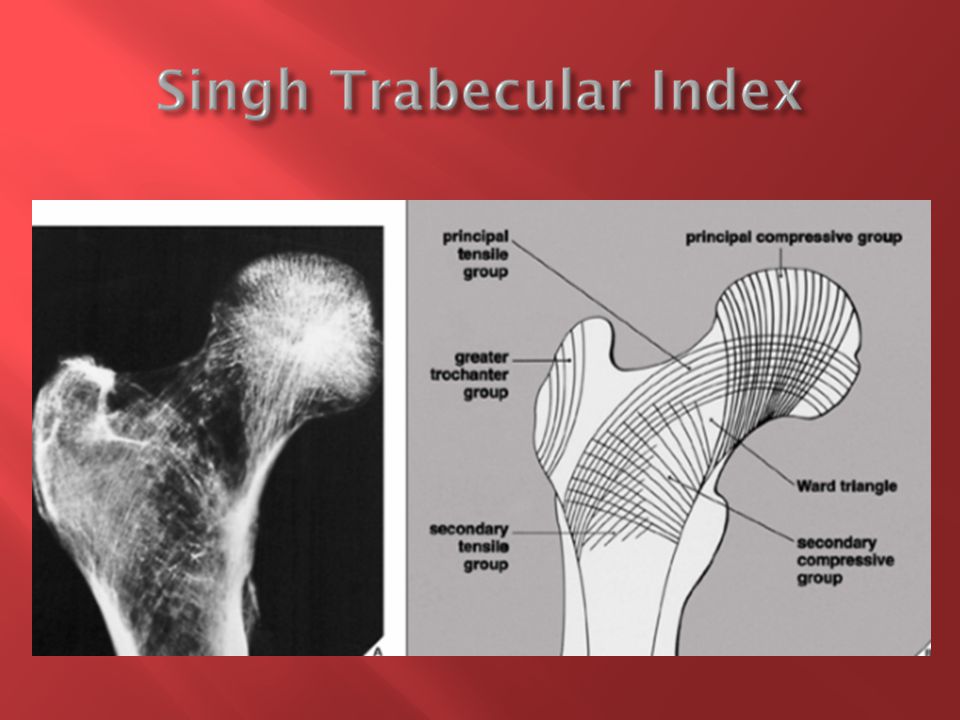
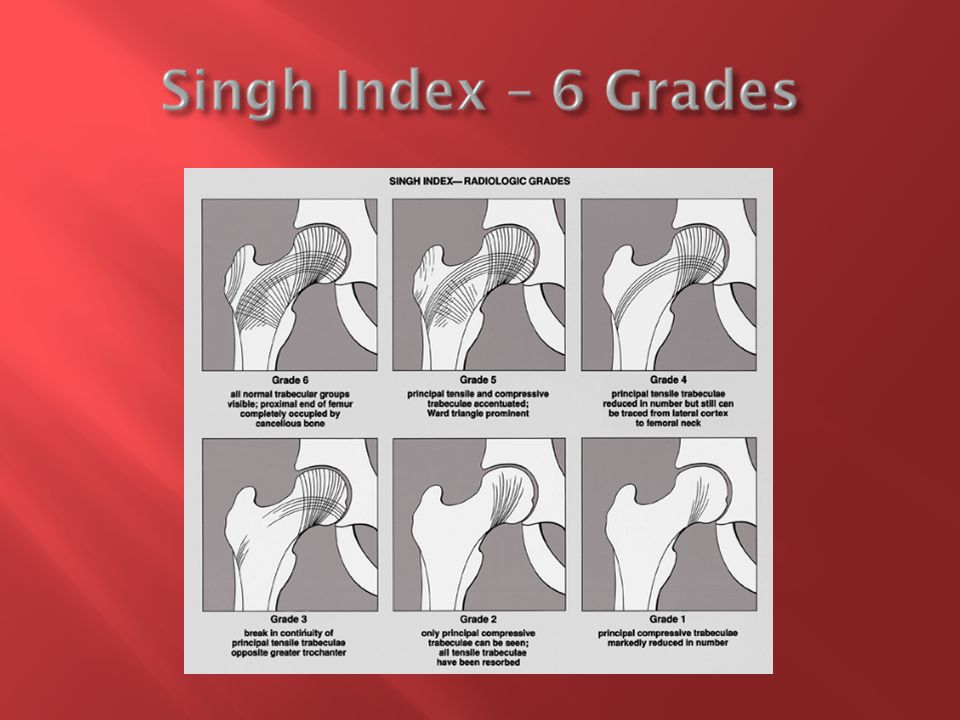
Detect osteoporosis - (Fragility) fractures Quantification -Measure bone mass : Semiquantitative(Conventional Radiography) Quantitative (Bone Mass Densitometry) Morphometry : Radiogrammetry Singh Index Vertebral Morphometry Bone Mineral Densitometry(BMD) : DXA (Dual energy X – ray absorptiometry) - Axial/Peripheral QCT (Quantitative CT – Axial/Peripheral),HRCT Other – QUS,QMR
 fractures Quantification -Measure bone mass : Semiquantitative(Conventional Radiography) Quantitative (Bone Mass Densitometry) Morphometry : Radiogrammetry Singh Index Vertebral Morphometry Bone Mineral Densitometry(BMD) : DXA (Dual energy X – ray absorptiometry) - Axial/Peripheral QCT (Quantitative CT – Axial/Peripheral),HRCT Other – QUS,QMR")
11
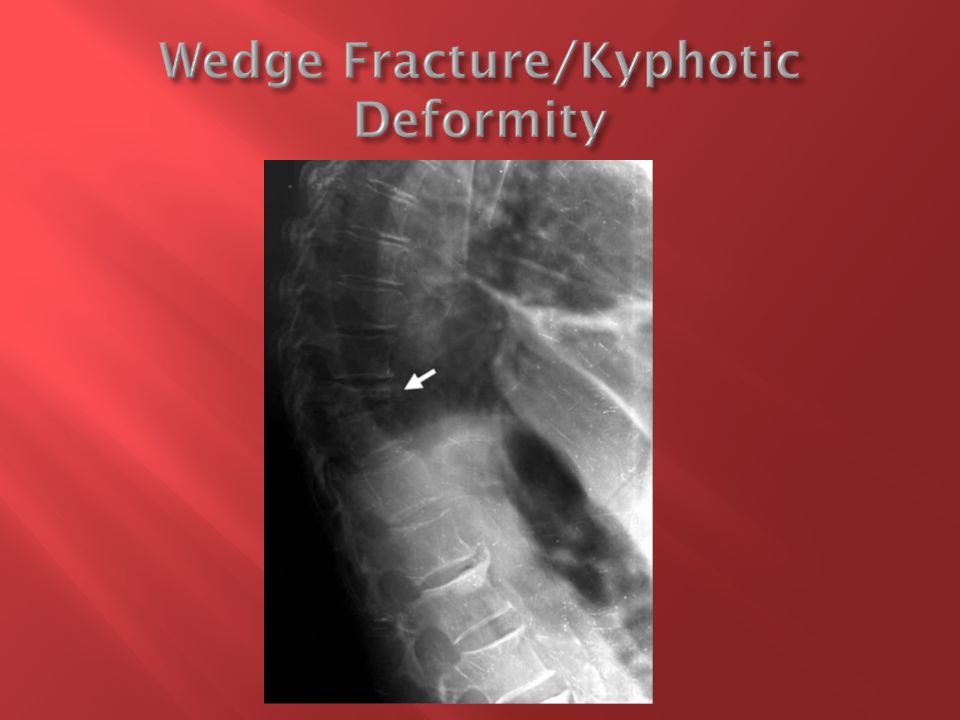
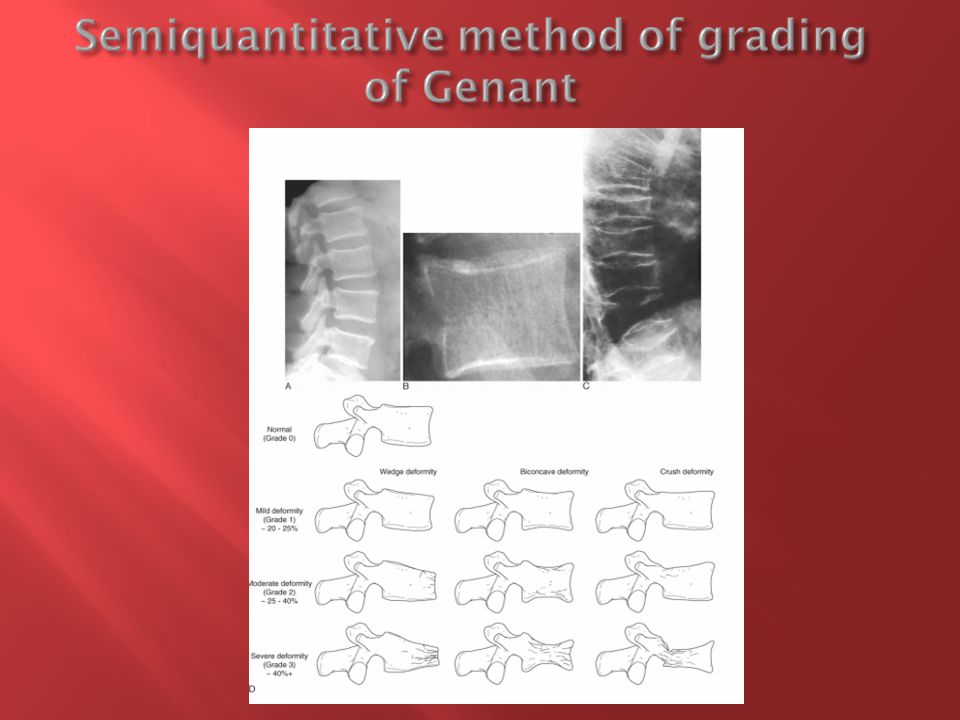
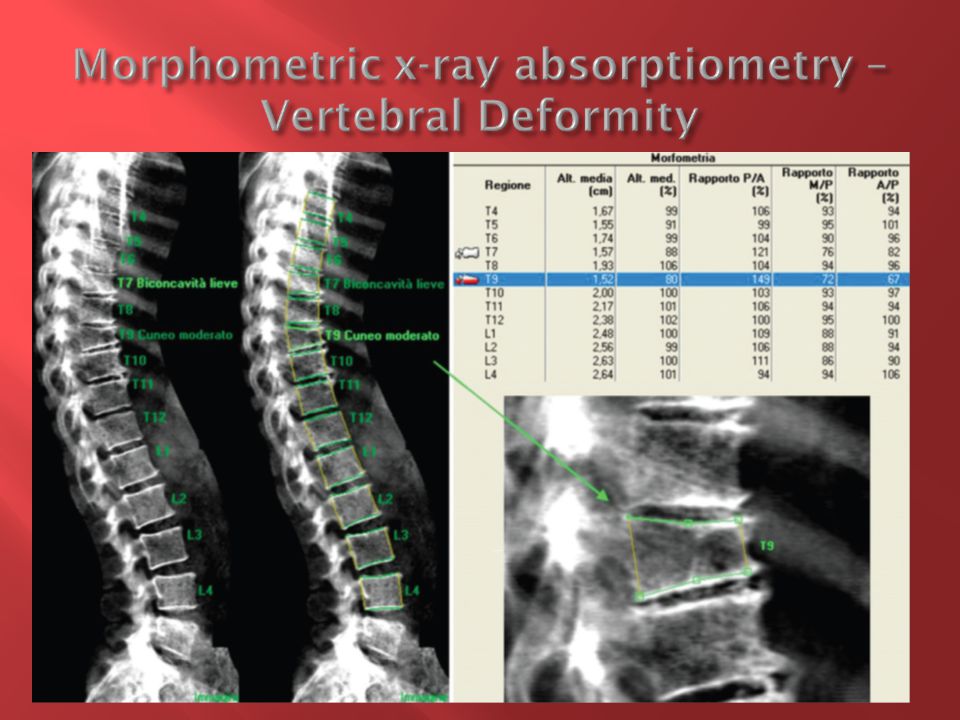
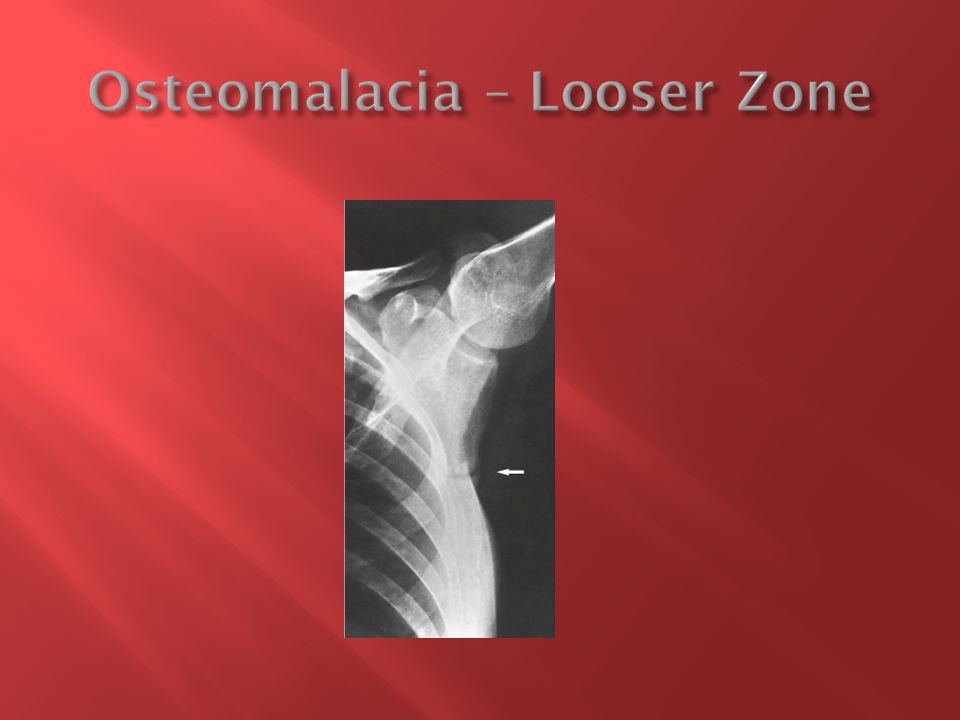
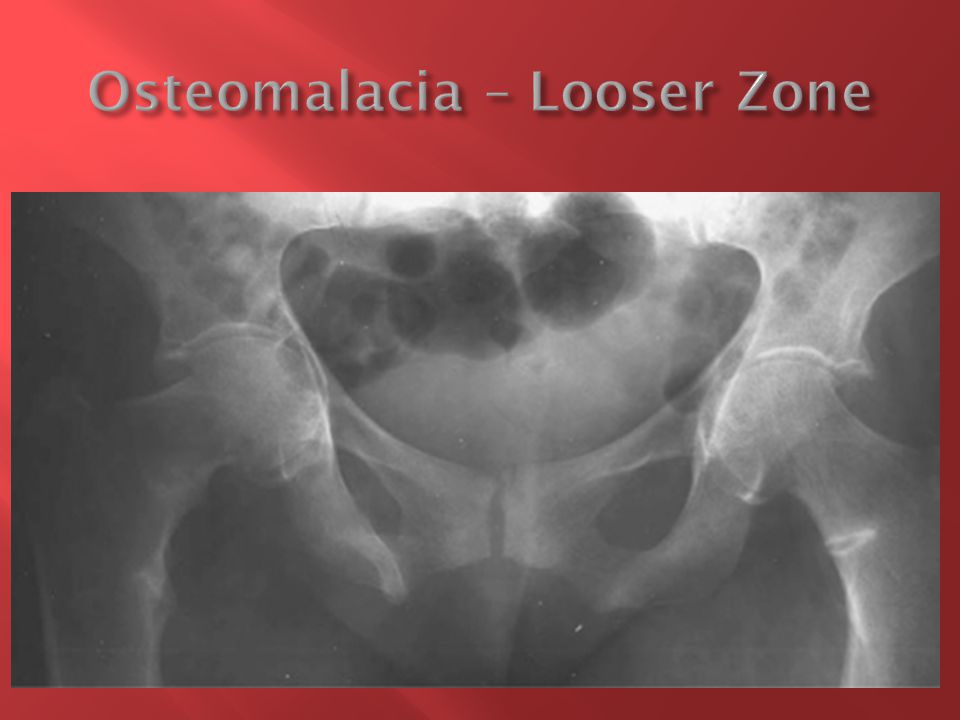
Increased Radiolucency/Cortical Thinning Notoriously inaccurate : 30 – 40 % loss of bone mass need to be present before detection 25 % of apparent osteopenia on radiography (technical faults) or vertebral fractures(juvenile epiphysitis,normal variants,trauma) have normal BMD Can detect osteomalacia/hyperparathyroidism Loss of at least 20% or 4 mm vertebral body height required for diagnosis of vertebral fracture – increase risk of subsequent fractures of vertebrae x 2 and hip x 5
 or vertebral fractures(juvenile epiphysitis,normal variants,trauma) have normal BMD Can detect osteomalacia/hyperparathyroidism Loss of at least 20% or 4 mm vertebral body height required for diagnosis of vertebral fracture – increase risk of subsequent fractures of vertebrae x 2 and hip x 5")
17
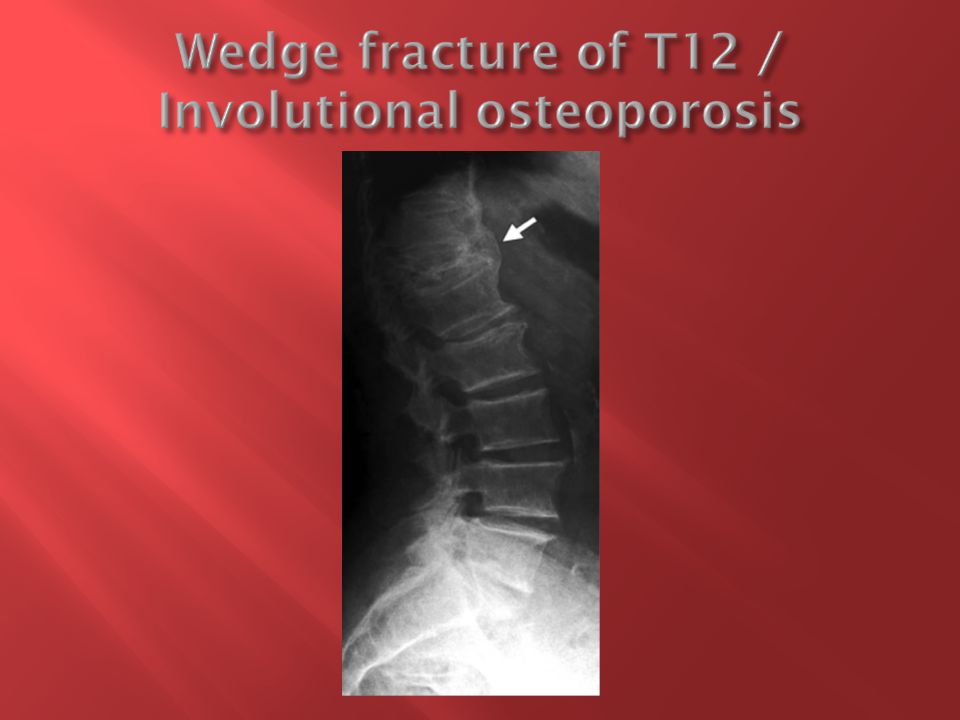
Not pain free within 6-8 weeks Non Anterior Wedge Posterior Wedge(other than L4+5) Above T7 Concave posterior vertebral border is more likely a sign of benign osteoporotic fracture, whereas a convex posterior border suggests malignant disease. Consider : Neoplastic disease – multiple myeloma/metastases Osteomalacia Schauermans disease(Juvenile epiphysistis) Trauma Degeneration MR imaging findings of malignant disease include multiple contrast enhancing lesions or soft-tissue masses, with or without encasing epidural masses and destructive changes
 Trauma Degeneration MR imaging findings of malignant disease include multiple contrast enhancing lesions or soft-tissue masses, with or without encasing epidural masses and destructive changes.")
25
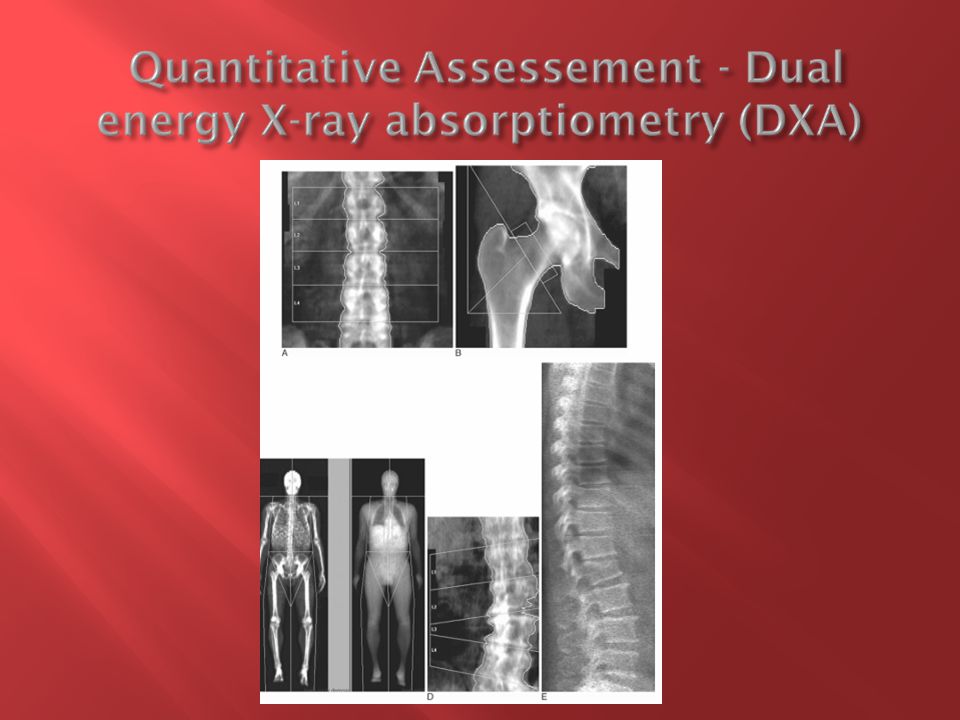
Rapid scanning Precise results if performed meticulously Extreme low doses of radiation Vertebral assessement from lateral images obtained on fan beam DXA system can be done at 1/100 th of dose of conventional radiography. Central/Peripheral DXA

26
Calibrated at least 1/week Meassurement monoplanar – g/cm2 and therefor size dependant (children) All calcium in path of electron beam contributes to BMD(Aortic calcifications degenerative/hyperostotic changes/vertebral wedging,metallic pinning) with overestimation of BMD.Exclude these areas from analysis/Lateral scanning Strontium ranelate treatment – artefactual increase in BMD Results of different scanners not interchangeable
 All calcium in path of electron beam contributes to BMD(Aortic calcifications degenerative/hyperostotic changes/vertebral wedging,metallic pinning) with overestimation of BMD.Exclude these areas from analysis/Lateral scanning Strontium ranelate treatment – artefactual increase in BMD Results of different scanners not interchangeable")
27
Need appropriate race and sex matched BMD reference ranges – ethnic differences in BMD and fracture prevelance Expressed as standard deviation from : Age matched – Z Score Peak bone mass – T Score Normal - > – 1 sd Osteopenia - – 2.5 sd Osteoporosis - < -2.5 sd Severe Osteoporosis - fragility fractures

28
Woman > 65 years and men > 70 years Radiographic evidence of osteoporotic vertebral fractures or apparent osteopenia History of fragility fractures after age 40 Known causes of secondary osteoporosis : Early menopause(< 45 years of age) / hypo gonadism in men/woman Systemic diseases with adverse effect on bone Bone toxic drugs
 / hypo gonadism in men/woman Systemic diseases with adverse effect on bone Bone toxic drugs")
29
Facilitate desicions regarding initiation/ discontinuation of drug therapy (biphosphonates /HRT) Strong clinical risk factors: Family history of hip fractures or osteoporosis BMI < 19 kg/m2 Regular C2H5OH intake(>3 drinks/day) Smoking Poor nutrition /Calcium intake/Vitamin D exposure
 Strong clinical risk factors: Family history of hip fractures or osteoporosis BMI < 19 kg/m2 Regular C2H5OH intake(>3 drinks/day) Smoking Poor nutrition /Calcium intake/Vitamin D exposure")
30
Low specificity – < 50 % of known osteoporotic fractures have BMD in osteoporotic range(T < - 2.5) Other risk factors like propensity to falls or qualitative risk factors like bone turnover not included Extrapolation to other populations measured at different skeletal sites with other techniques (QUS,QCT) not acceptable. Other metabolic bone diseases Intervention threshold applicable to all

31
Confirm diagnosis with BMD or presence of fragility fracture before initiation of treatment with bone active drugs. Axial BMD to be used to diagnose and access rate of bone loss/gain. QCT/QUS not recommended and results cannot be applied to T score based WHO diagnostic classification Lowest BMD value measured at spine,total femur and femur neck(or distal radius if invalid) Express results for post menopausal Caucasian woman as T scores and Z scores for pre menopausal woman and men < 50 year Men over 50 years : Employ female reference data to determine T score Local black population : use reference data for Caucasian females for all subjects of all races until local reference values become available.
 Express results for post menopausal Caucasian woman as T scores and Z scores for pre menopausal woman and men < 50 year Men over 50 years : Employ female reference data to determine T score Local black population : use reference data for Caucasian females for all subjects of all races until local reference values become available..")
32
Children:Low BMD + significant fracture history Follow up scans every 18-24 months or earlier in GIOP Search for evidence of vertebral compression fractures in all who qualify for BMD measurement – Standard x-ray and use modified Genant semiquintative system to grade (Gr.1-3) Higher grade = higher risk for subsequent fractures of hip and vertebrae or DXA VFA.
 Higher grade = higher risk for subsequent fractures of hip and vertebrae or DXA VFA.")
33
Considered treatment after prior fragility fracture(wrist, spine,hip,pelvis,rib,humerus) regardles of BMD value Considered treatment if DXA T Score < -2.5 at hip or spine Considered treatment if DXA T score -1- -2.5 (osteopenia) if significant clinical risk factors. BMD measured on all patients on long term glucocorticosteroids(50% develop GIOP regardless of dose)-start treatment if T Score < - 1.5 Biphophonates – 1 st line preventative therapy and anabolics reserved for advanced disease
-start treatment if T Score < Biphophonates – 1 st line preventative therapy and anabolics reserved for advanced disease.")
35
Reduce the high subjectivity and poor reproducibility of qualitative readings Vertebral fractures are one of the most important CRF – 60% asymptomatic and go undetected if not routinely searched for Visualize lateral spine on DXA with VFA software Lower radiation dose and cost compared to conventional radiography Conventional radiography remain gold standard – often only requested if fracture is suspected

37
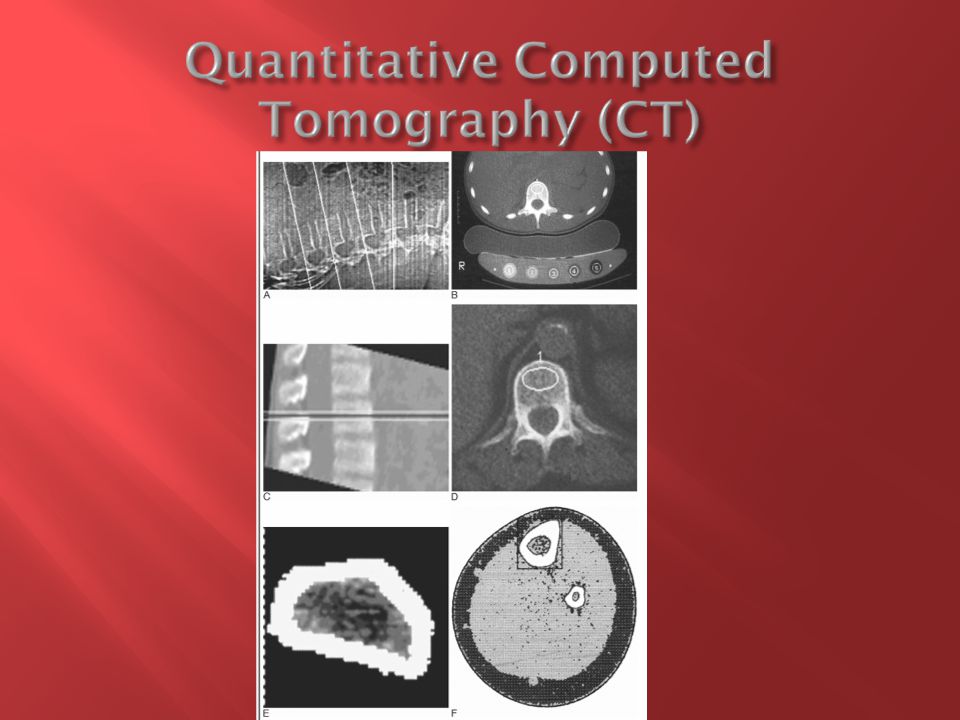
Separate estimation of cortical and trabecular bone True volumetric density – g/cm3 making it non size dependant (children/small stature) Performed with calibration reference phantom to transform HU into BMD equivalents Radiation dose compares favourably with conventional radiography Excellent for predicting vertebral fractures and serially measuring bone loss - selectively assesses the metabolically active and structurally trabecular bone Increase in marrow fat is age related, single-energy CT data can be corrected with use of age-related reference databases
 Performed with calibration reference phantom to transform HU into BMD equivalents Radiation dose compares favourably with conventional radiography Excellent for predicting vertebral fractures and serially measuring bone loss - selectively assesses the metabolically active and structurally trabecular bone Increase in marrow fat is age related, single-energy CT data can be corrected with use of age-related reference databases")
39
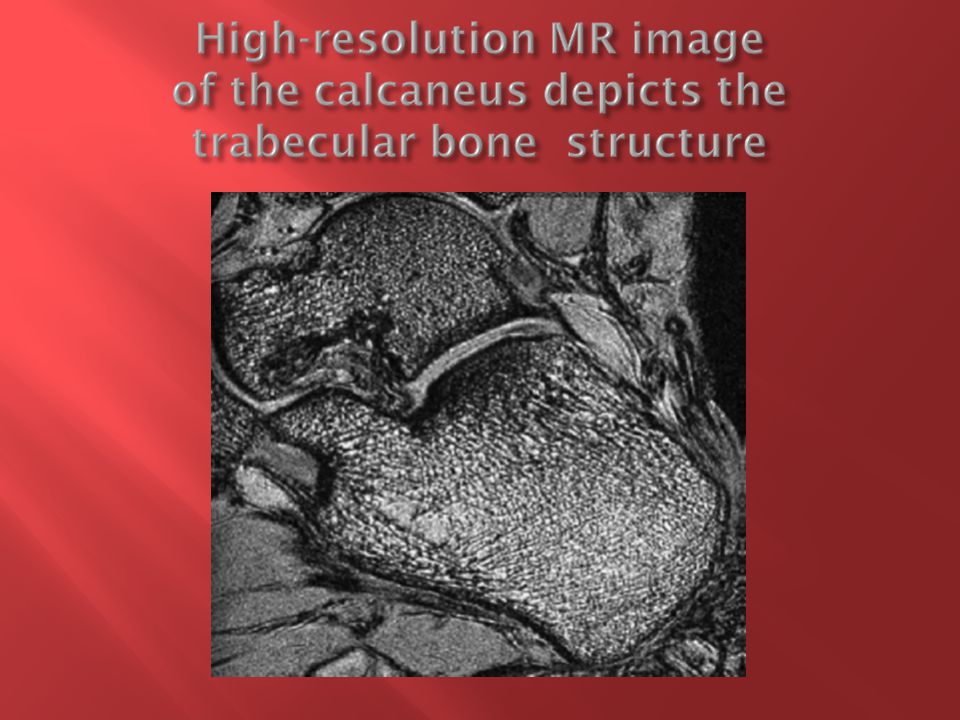
Can be used to detect differences in trabecular structure depending on patient age, BMD, and osteoporotic status Most often performed at peripheral sites such as the calcaneus, knee, and wrist. Substantial improvement in fracture discrimination made possible by considering structural information as well as BMD May replace biopsy when this would be advocated.

50
http://www.iofbonehealth.org/ - accessed 28/04/2012 http://www.iofbonehealth.org/ Grainger and Allison’s Diagnostic Radiology A Textbook of Medical Imaging,5 th Edition Orthopedic Imaging A Practical Approach Adam Greenspan,5 th Edition Radiographics : September – October 2011 Integrated Imaging Approach to Osteoporosis: State-of-the-Art Review and Update

Similar presentations








, Fellowship Diabetes/Endocrinology (AKUH), PG Dip Diab (UK) Consultant Endocrinologist.>")


>")








 This is the gold standard in Osteoporosis diagnosis. Reported as.>")



 Dr Malith Kumarasinghe MBBS (Colombo)>")