Download presentation
Presentation is loading. Please wait.

1
Chapter 15 Hypersensitivity Reactions, Allergies Dr. Capers
immunology

2
Kindt • Goldsby • Osborne
Kuby IMMUNOLOGY Sixth Edition Chapter 15 Hypersensitivity Reactions Copyright © 2007 by W. H. Freeman and Company

3
Hypersensitivity – responding inappropriately to an antigen
Inflammatory response can have deleterious effects Tissue injury Disease death

4
Hypersensitivity Reactions
May develop in course of humoral OR cell-mediated response Immediate hypersensitivity Anaphylactic Antibody-antigen complexes Manifests in minutes Delayed-type hypersensitivity May occur in days

6
Type I – IgE-Mediated Hypersensitivity
Induced by antigens referred to as allergens Induces humoral response but induces high secretion of IgE Fc portion of IgE binds with Fc receptors on mast cells and basophils Degranulation occurs

7
Type I

8
Type 1 Common components Allergens IgE Mast cells and basophils
Atopy – hereditary predisposition to development of immediate hypersensitivity reactions to common antigens Allows nonparasitic antigens to induce IgE response IgE Normally lowest of all antibody classes in serum Half-life is 2-3 days but once bound to mast cells or basophils, can last for weeks Mast cells and basophils IgE binding receptors High affinity Low affinity Atopic individuals have higher amount of soluble IgE receptor that has been shown to increase IgE production by B cells

10
IgE cross-linkage initiates degranulation
Once cross-linkage of antigen has occurred, intracellular signaling result in mast cell degranulation Cooperation among protein and lipid kinases, phosphatases, rearrangement of the cytoskeleton

11
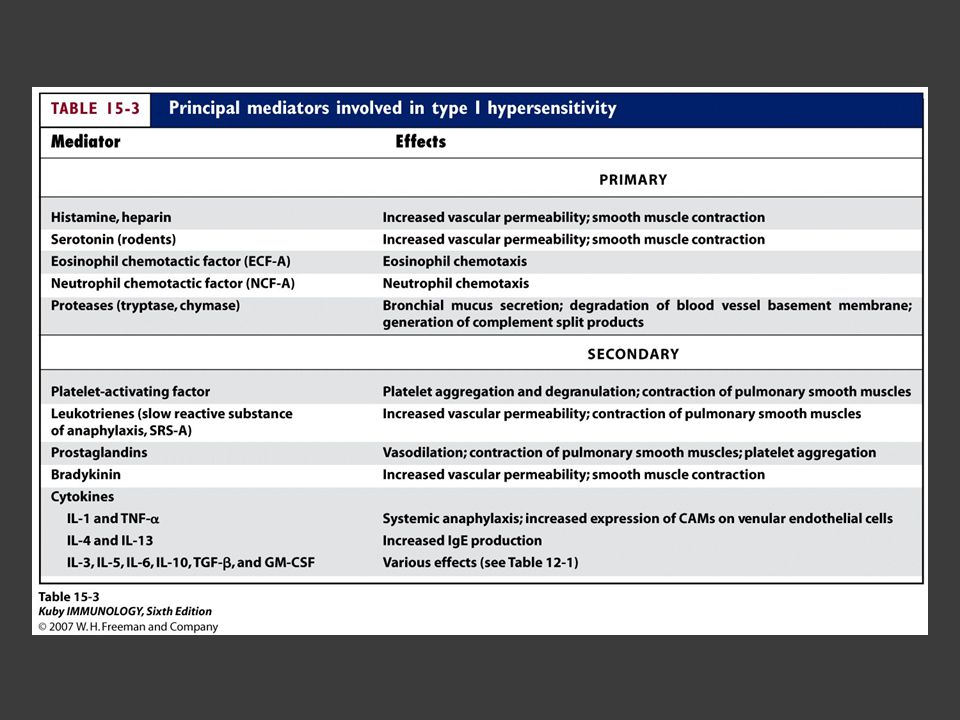
Pharmacologic agents that mediate Type I
Primary mediators Made before and stored in granules Histamine, proteases, eosinophil chemotactic factor, heparin Secondary mediators Synthesized after Platelet-activating factor, leukotrienes, prostaglandins, bradykinins, some cytokines and chemokines

13
Histamine Formed by decarboxylation of amino acid Histidine
Major component of granules Effects observed in minutes Contraction of smooth muscle (intestinal and bronchial), increase permeability of venules, increased mucus secretion by goblet cells
, increase permeability of venules, increased mucus secretion by goblet cells.")
14
Leukotrienes and prostaglandins
Effects longer to become apparent Effects longer lasting than histamine Bronchoconstriction, vascular permeability, mucus production

15
Type 1 can be systemic or localized
Systemic anaphylaxis Quick, can be fatal Respiration labored, blood pressure drops, bronchiole constriction, edema, shock Epinephrine treats, relaxes smooth muscle and increases cardiac output (prevents vascular collapse)
")
16
Type 1 can be systemic or localized
Localized Hypersensitivity Reactions (Atopy) Allergic Rhinitis Most common, “hay fever” Asthma Triggered like hay fever but doesn’t happen in nasal cavity, happens in lower respiratory tract Food allergies Hives, vomiting Atopic dermatitis Allergic eczema
 Allergic Rhinitis. Most common, hay fever Asthma. Triggered like hay fever but doesn’t happen in nasal cavity, happens in lower respiratory tract. Food allergies. Hives, vomiting. Atopic dermatitis. Allergic eczema.")
17
Asthma Inflammatory disease
Induce expression of adhesion molecules on endothelial cells for eosinophils and neutrophils Cause significant injury because of toxic enzymes, cytokines Notice sloughing of the pseudostratified ciliated columnar epithelial cells lining the bronchiole

18
Clinical Methods to detect Type 1
Skin testing Checking serum level of IgE

19
Control of Type 1 Avoiding contact Immunotherapy Drug therapies
Subcutaneous injections of allergens Causes shift to IgG production instead of IgE Monoclonal anti-human IgE Drug therapies

20
Type II – Antibody-Mediated Cytotoxic Hypersensitivity
Transfusion Reactions Due to exposure to microorganisms in gut, individuals have antibodies to blood types not their own Antibody attaches to RBC and initiates complement system to lyse RBC After lysis: Hemoglobin detected in plasma, starts to filter through kidneys and found in urine (hemoglobinuria) Hemoglobin converted to bilirubin – toxic at high levels Fever, chills, blood clotting
 Hemoglobin converted to bilirubin – toxic at high levels. Fever, chills, blood clotting.")
21
Type II – Antibody-Mediated Cytotoxic Hypersensitivity
Hemolytic disease of newborn Rh+ fetus, Rh- mother IgG antibodies cross placenta Some of these antibodies may be anti-Rh antibodies Can have severe consequences Antibodies against ABO blood groups produce less consequences, can be easily treated Rhogam shot Given to mother Anti-Rh antibodies bind to fetal cells that might have entered mother’s system during birthing process, facilitates clearing before there is a B cell response

23
Type III – Immune complex-mediated hypersensitivity
Complexing of antigen plus antibody facilitates phagocytosis and clearing of antigen Large amounts of these complexes can lead to tissue damage

25
Type III can be localized
Injection of antigen intradermally or subcu into animal that has high level of antibody for that antigen Arthus reaction Bug bites

26
Type III can be generalized
Serum sickness After receiving antiserum (serum from another animal that may contain antitoxins for treatment) Use of monoclonal antibodies for use of cancer treatment Patient developed antibody against mouse monoclonal antibody Autoimmune diseases Lupus, Rheumatoid arthritis Drug reactions Penicillin, sulfonamides Infectious disease
 Use of monoclonal antibodies for use of cancer treatment. Patient developed antibody against mouse monoclonal antibody. Autoimmune diseases. Lupus, Rheumatoid arthritis. Drug reactions. Penicillin, sulfonamides. Infectious disease.")
27
Type IV – Delayed-type Hypersensitivity
Some subpopulations of TH cells encounter antigen, secrete cytokines and induce localized inflammatory response Most cases are not detrimental

28
Type IV Sensitization phase and Effector phase of DTH

29
Prolonged DTH can lead to formation of granuloma Tuberculosis test is done this way

30
Type IV – contact dermatitis

31
Chronic Inflammation Causes: Infections
Continuing physical damage to tissue Obesity autoimmunity

Similar presentations





 is an inappropriate immune response that may develop in the humoral or cell- mediated responses -Was first.>")
 A practice exam for exam 5 Learning objectives for exam 5>")








 hypersensitivities Characterized by.>")





 leading to damage Require sensitizing dose(s) Introduction to Lab Ex. 24:>")

