Download presentation
Presentation is loading. Please wait.

1
Surgical management in the setting of neo-adjuvant therapy Frances Wright MD MEd FRCSC Associate Professor of Surgery

2
Outline of Talk Locally advanced breast cancer and NAT Smaller high risk tumors and NAT Operations on the breast Operations on the axilla

3
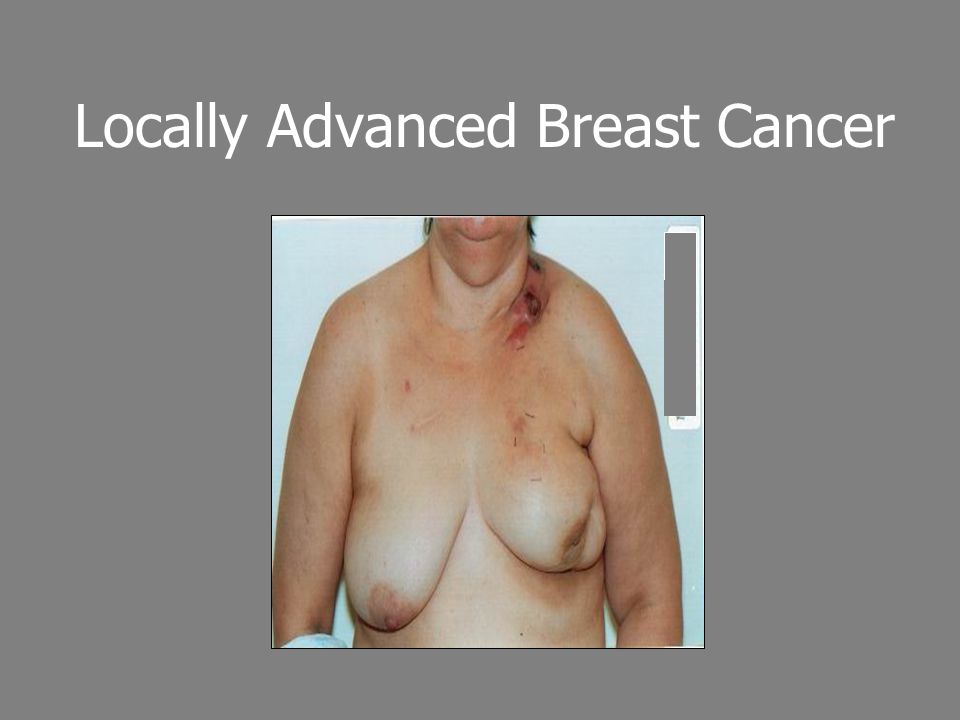
Who gets neo-adjuvant therapy? Locally advanced breast cancer –Tumor > 5cm –Skin involvement, chest wall involvement –Fixed, matted axillary nodes –Supraclavicular nodes –Inflammatory breast cancer Inoperable and operable –Can I get clear margins?

4
Locally Advanced Breast Cancer

6
Inoperable Breast Cancer Neo-adjuvant therapy (NAT) –Assess response Successful - surgery - then radiation post op If fails - change chemotherapy regime If that fails – radiation –Then possibly surgery (some success with triple negative patients with twice daily rads) Shenkier 2004
 –Assess response Successful - surgery - then radiation post op If fails - change chemotherapy regime If that fails – radiation –Then possibly surgery (some success with triple negative patients with twice daily rads) Shenkier 2004")
7
Inoperable Breast Cancer: Inflammatory Breast Cancer Success story of multi-modal treatment Treatment Approach5 year survival Mastectomy 0 Radiation 0 Mastectomy & Radiation 0 Pre-op chemo, surgery, rads 46% Lopez 1996

8
Who gets neo-adjuvant therapy? Smaller high risk tumors (2-5cm) –Her 2 neu positive, triple negative –Node positive –Often younger patients (<50)
 –Her 2 neu positive, triple negative –Node positive –Often younger patients (<50).")
9
Pre-operative work up 2-5cm Node neg 2-5cm Node pos LABC Mammo, U/S MRI Core biopsy and receptors Clip if considering BCS Metastatic work up Bone scan, CT chest, abd pelvis Maybe

10
Pre-operative work up LABC Imaging work up –7% contralateral breast cancer Metastatic work-up –~10% will have mets at presentation

11
NAT and Survival Overall, no demonstrated overall survival benefit with pre-op vs. post-op chemotherapy (NSABP 18, 27) –Subset analysis for women < 50 –Pre-op chemo trend toward improved overall survival vs. post op chemo –At 16 years OS 61% (NAT) vs 55% (post op chemo) Rastogi 2008
 –Subset analysis for women < 50 –Pre-op chemo trend toward improved overall survival vs. post op chemo –At 16 years OS 61% (NAT) vs 55% (post op chemo) Rastogi")
12
NAT provides in vivo tumour assessment Assess response to chemo (Chawla 2012) 91% respond 6% stable 3% progress –Does the chemo need to be changed? –Does the patient need to get to the OR for salvage mastectomy?

13
NAT and Prognostication Good prognosticator Aim of neo-adjuvant chemotherapy is complete pathological response (pCR) Better response = Improved survival Estevez 2004
 Better response = Improved survival Estevez 2004")
14
Complete Pathological Response and Improved OS in NSABP 18, 27 Rastogi 2008 JCO Chemo Regime Doxorubicin/ cyclophosphamide (AC) x 4 cycles All women > 50 received tamoxifen post op x 5 years pCR 6.7% pCR
 x 4 cycles All women > 50 received tamoxifen post op x 5 years pCR 6.7% pCR")
15
Pathological Complete Response and Breast Cancer Subtype Tumor SubtypePercentage of type of breast cancer Complete pathological response ER/PR pos, her2 neg40-55%8% ER/PR pos, her 2 pos “Triple positive” 15-20%19% ER/PR neg, her 2 pos7-12%39% Triple Negative13-25%31% Houssami 2012 EJC

16
NAT and Impact on Surgery Increased rate of breast conserving surgery (BCS) –Improves cosmesis and patient satisfaction ~ 25% reduction in mastectomy rate to BCS with pre-op chemo Chawla 2012
 –Improves cosmesis and patient satisfaction ~ 25% reduction in mastectomy rate to BCS with pre-op chemo Chawla 2012")
17
Breast Cancer Subtype and Impact on Breast Surgery Patient InfoRate of Breast Conserving Treatment Re-operation rate Overall694 patients40%7.2% Triple Negative25% (170)47%3.5% Her 2 neu positive30% (207)43%6.8% ER/PR+/ her 2 neu neg46% (317)35%9.8% Data from ACOSOG Z1071 – sentinel node biopsy after NAC Patient age, stage did not differ across subgroups Boughey 2014 Annals of Surgery
47%3.5% Her 2 neu positive30% (207)43%6.8% ER/PR+/ her 2 neu neg46% (317)35%9.8% Data from ACOSOG Z1071 – sentinel node biopsy after NAC Patient age, stage did not differ across subgroups Boughey 2014 Annals of Surgery")
18
Is the recurrence rate higher if we downstage patients? StudyNumber of patients Local Recurrence Median Follow up Comments NSABP 18 Pre-op Chemo Downstaged BCS (11/69) vs mastectomy (43/434) 15.9% vs 9.9%9 years When controlled for age, initial tumor size, no difference in LRR NSABP 18 – pre operative vs post operative chemo Higher local recurrence in women < 50 (p=0.00003) (13.1% vs 5.2%) Tumor size did not correlate with local recurrence Biology more important
 vs mastectomy (43/434) 15.9% vs 9.9%9 years When controlled for age, initial tumor size, no difference in LRR NSABP 18 – pre operative vs post operative chemo Higher local recurrence in women < 50 (p= ) (13.1% vs 5.2%) Tumor size did not correlate with local recurrence Biology more important.")
19
Updated MD Anderson data 652 patients received NAT At 5 years –93% LRR free survival rates for NAT –97% LRR for surgery first –Patients receiving NAT had more advanced disease Mittendorf 2013

20
Updated MD Anderson data Multivariate analysis for local regional recurrence age < 50 clinical stage III, grade 3 ER neg disease ER positive (but not take treatment) LVI multifocal disease on pathology close/ positive margins (wanted at least 2 mm) LRR driven predominantly by disease stage/ tumor biology Mittendorf 2013
 LVI multifocal disease on pathology close/ positive margins (wanted at least 2 mm) LRR driven predominantly by disease stage/ tumor biology Mittendorf 2013")
21
BCS margins after NAT MD Anderson wants 2mm margin with BCS after pre-op chemo They do not remove entire pre-chemo tumor volume (Mittendorf 2013) There is no data from prospective trials regarding margin width and oncologic safety (Kummel 2014)
 There is no data from prospective trials regarding margin width and oncologic safety (Kummel 2014)")
22
Surgical Complications after NAT NSQIP study (2005-11) –Compared outcomes in patients who had NAT and those who did not –NAT was independently associated with a lower overall morbidity for patients who did and did not have breast reconstruction –Unclear why NAT protective Abt 2014 JAMA
 –Compared outcomes in patients who had NAT and those who did not –NAT was independently associated with a lower overall morbidity for patients who did and did not have breast reconstruction –Unclear why NAT protective Abt 2014 JAMA")
23
Choosing who should get BCS after NAT Difficult to judge clinically, amount of disease present –Not all tumours are discrete masses

24
Imaging Accuracy after NAT StudyNo. of patients Correlation of residual disease after NAT with pathology as the gold standard ClinicalMRMUSMRI Yeh 2005 31 IIB, IIIA19%26%35%71% Akazawa 2006 30R=0.55R=0.49R=0.9 Balu-Maestro 2002 6052%38%43%63% Partridge 2002 52R=0.6R=0.89 Rosen 2003 21 LABCR=0.61R= 0.75 Londero 2004 15 LABCR=0.67R=0.57R=0.70 Cheung 2003 33 LABCR=0.98 Weatherall 2001 20R=0.72R=0.63R=0.94 Segara 2007 68 I, II, IIIR=0.44R= 0.61R=0.75 Belli 2006 45R= 0.97 Range 0.44 – 0.7226% - 0.6735%-0.6163%-0.97

25
Meta-analysis of accuracy of MRI after NAT MRI – slightly overestimate pathologic size –Measurement errors can be large enough to be clinical significant –Chemotherapy effect – decrease in contrast enhancement parameters –Loss of tumour continuity – to non-continuous small foci –Decrease tumour cellularity (Rieber 2002, Warren 2004, Schott 2005, Thibault 2004, Rosen 2003, Rajan 2004) MRI more accurate than mammogram Need studies comparing MRI to ultrasound Marinovich 2013
 MRI more accurate than mammogram Need studies comparing MRI to ultrasound Marinovich 2013")
26
Pre-Treatment Circumscribed mass with rim enhancement After NAT Tumour shrank to Smaller mass, resectable

27
Pre-Treatment MRI of Breast Cancer After NAT Tumour shrunk to lesser volume along septa

28
BCS decisions based on breast cancer histology Lobular carcinoma –Very difficult to assess extent of disease clinically, mammogram and MRI –Not respond as well to pre-op chemo Inflammatory carcinoma –High rate of recurrence (39%) if no surgery and just radiation after chemotherapy (Danforth 1998 – did if post chemo biopsy was negative)
 if no surgery and just radiation after chemotherapy (Danforth 1998 – did if post chemo biopsy was negative)")
29
Lymph Node Staging and LABC

30
Likelihood of having lymph node involvement Diameter of primary tumour Percent with positive axillary nodes 0.5 - 0.9 cm20.6% 1.0 - 1.9 cm33.2% 2.0 – 2.9 cm44.9% 3.0 – 3.9 cm55.2% 4.0 – 4.9 cm 60.0 % > 5.0cm70.0% Carter 1989

31
Node Negative before NAT Clinically and radiologically node negative prior to NAT SNB –We have asked our radiologists not to biopsy indeterminate lymph nodes Allows for patient to get benefit from NAT if nodes were positive 40% downstaging

32
Node positive before NAT Is sentinel node biopsy accurate when nodes are positive and the patient then receives NAT?

33
ACOSOG Z1071 663 evaluable patients with positive axillary nodes (biopsy proven) –649 had chemo followed by SNB + ALND –7.1% (46) could not identify SNB –12% (78 patients) had only 1 SNB –No cancer in 41% (215) = pCR 41% –39 no cancer in SNB but cancer found on ALND False negative 12.6% Boughey 2013 JAMA
 –649 had chemo followed by SNB + ALND –7.1% (46) could not identify SNB –12% (78 patients) had only 1 SNB –No cancer in 41% (215) = pCR 41% –39 no cancer in SNB but cancer found on ALND False negative 12.6% Boughey 2013 JAMA")
34
ACOSOG Z1071 What decreased the false negative ? –Mapping performed with two agents (blue dye and radiocolloid 89% of time ) vs one agent FNR = 10.8% vs 20.8% –Examination of at least 3 sentinel nodes FNR = 9.1% vs 21.1% Boughey 2013 JAMA
 vs one agent FNR = 10.8% vs 20.8% –Examination of at least 3 sentinel nodes FNR = 9.1% vs 21.1% Boughey 2013 JAMA.")
35
Similar Trials – Assessing accuracy of SNB in node positive patients post chemo Sentina –1737 patients had NAT For clinically node positive group All got SNB and ALND Detection rate overall 80% When > 3 sentinel nodes removed after chemo, FNR < 10% Double mapping, FNR 8.6% Kuehn 2013 Lancet Oncology

36
Similar Trials – Assessing accuracy of SNB in node positive patients post chemo SN FNAC (Canadian) –FNR 8.4% overall –FNR 4.9% when >2 nodes removed Boileau 2014 in press
 –FNR 8.4% overall –FNR 4.9% when >2 nodes removed Boileau 2014 in press")
37
A (complicated) way forward ? MD Anderson –TAD (targeted axillary dissection) –Placing a clip at time of the lymph node biopsy –At time of surgery (after neo-adjuvant chemo), lymph node is localized –During the SNB – all SLNs and the clipped nodes are removed and doing ALND (to see accuracy) Undergoing study now Mittendorf 2014
 –Placing a clip at time of the lymph node biopsy –At time of surgery (after neo-adjuvant chemo), lymph node is localized –During the SNB – all SLNs and the clipped nodes are removed and doing ALND (to see accuracy) Undergoing study now Mittendorf")
38
New frontiers Sentinel node positive after NAT –ALND? –Radiation? (would it deal with chemo resistant disease?)
.")
39
Lymph Nodes as prognosticators after NAT Post NAT nodal status5 year survival Negative nodes75% 1-4 nodes40-50% 5-10 nodes30% > 10 nodes20% McCready 1989

40
Future directions Further chemotherapy post operatively for patients who do NOT have pCR Especially high risk patients –Young patients –Triple neg –Her 2 neu positive (KATHERINE TRIAL)
")
41
Summary NAT – standard for patients < 50, triple negative, Her2 neu positive, LABC Pathological complete response affected by subtype (triple neg, Her 2 neu pos) which in turn can affect surgery Need to do pre and post imaging including MRI to assess extent and pattern of disease to decide if BCS appropriate
 which in turn can affect surgery Need to do pre and post imaging including MRI to assess extent and pattern of disease to decide if BCS appropriate")
42
Summary Who not to offer BCS –Inflammatory –Multifocal on initial MRI or post chemo MRI –Diffuse pre-op malignant calcifications on pre chemo mammogram

43
Summary Nodes –Node negative prior to NAT It is safe to offer sentinel node biopsy if lymph nodes clinically/ radiologically node negative prior to NAT –Node positive prior to NAT Likely sentinel node safe if use dual tracer and take out at least 3 nodes Jury out at the moment

44
New Chemotherapeutic Agents – better response for LABC Better response in subsets of breast cancers –Triple negative, Her 2 neu positive Her2 Positive patients (15-20% of all cancers) –NOAH study (Giani 2010) – chemo ( doxorubicin, paclitaxel, cyclophosphamide, methotrexate and 5 fluorouracil) + herceptin vs chemo alone – 38% vs 19% pCR –GeparQuinto study (2012) – chemo + herceptin vs chemo alone – 30% vs. 23% –Neosphere trial – Her2 positive/ER/PR positive pCR 26% and Her2neu positive/ER/PR-negative patients 63% pCR

45
New Chemotherapeutic Agents – better response for LABC Triple negative (15% of all breast cancers) –22% pCR (MD Anderson Liedke 2010) –Now using cisplatin especially for BRCA patients
 –22% pCR (MD Anderson Liedke 2010) –Now using cisplatin especially for BRCA patients")
46
Considerations based on Receptor Status Higher pCR with triple negative (25%), her 2 neu positive patients (40%) If good clinical and imaging response then I will consider lumpectomy post treatment even if large tumor to begin with Can always go back if margins positive or diffuse disease across lumpectomy specimen to do mastectomy
, her 2 neu positive patients (40%) If good clinical and imaging response then I will consider lumpectomy post treatment even if large tumor to begin with Can always go back if margins positive or diffuse disease across lumpectomy specimen to do mastectomy")
47
Personal Practice We use NAT in young patients < 50 who are Her 2 neu positive and triple negative I will consider BCS if one quadrant of disease or larger if patient is triple negative or her 2 neu positive and has had good response Nodes – moving toward SNB if node positive prior to NAT –Difficulty what to do if sentinel node positive – ? Will radiation deal with chemo-resistant disease –? Does patient need ALND

Similar presentations












>")






