Download presentation
Presentation is loading. Please wait.

1
Health Related Quality of Life after Transcatheter Aortic Valve Implantation vs. Non-Surgical Therapy among Inoperable Patients with Severe Aortic Stenosis: Results from the PARTNER Trial (Cohort B) David J. Cohen, M.D., M.Sc. On Behalf of the PARTNER Investigators Saint Luke’s Mid America Heart and Vascular Institute University of Missouri-Kansas City Kansas City, Missouri
 David J. Cohen, M.D., M.Sc. On Behalf of the PARTNER Investigators Saint Luke’s Mid America Heart and Vascular Institute University of Missouri-Kansas City Kansas City, Missouri.")
2
Disclosures The PARTNER trial was funded by a research grant from Edwards Lifesciences, Inc.

3
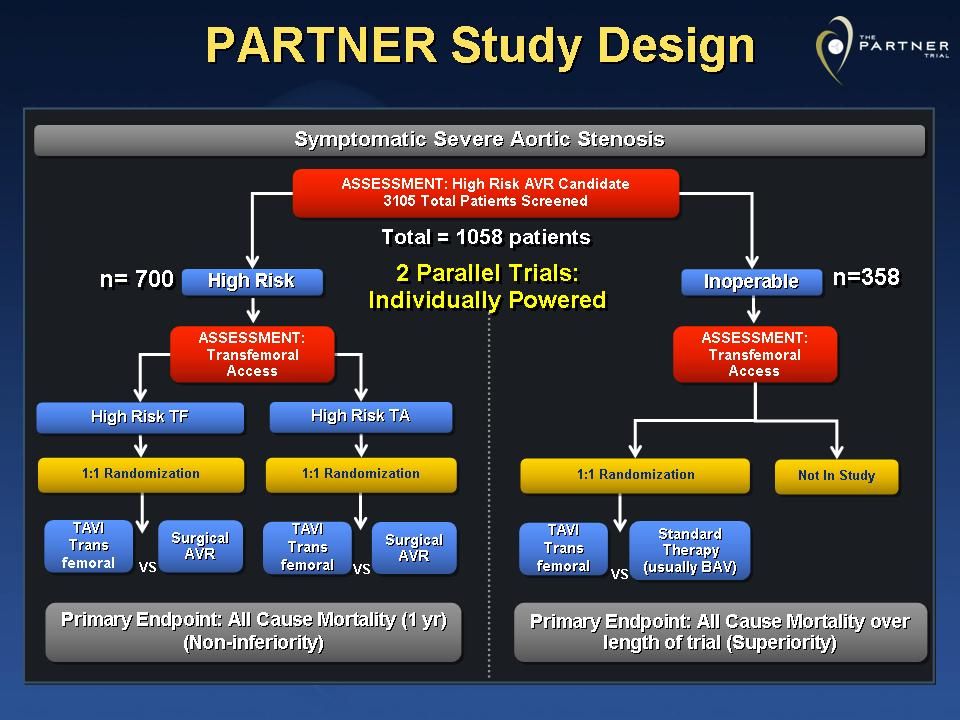
Background Over the past decade, transcatheter aortic valve implantation (TAVI) has been developed as a less-invasive alternative to surgical valve replacement for high-risk patients with severe aortic stenosis Recently, the PARTNER trial demonstrated that for patients who are not suitable candidates for surgery, TAVI led to a significant reduction in all-cause mortality (20% ARR at 1-year, p<0.001) but also an but also an increase in the incidence of major strokes and vascular complications Given the advanced age and multiple comorbid conditions in these inoperable patients, improvements in quality of life may be an equally important therapeutic goal as improved survival
 has been developed as a less-invasive alternative to surgical valve replacement for high-risk patients with severe aortic stenosis Recently, the PARTNER trial demonstrated that for patients who are not suitable candidates for surgery, TAVI led to a significant reduction in all-cause mortality (20% ARR at 1-year, p<0.001) but also an but also an increase in the incidence of major strokes and vascular complications Given the advanced age and multiple comorbid conditions in these inoperable patients, improvements in quality of life may be an equally important therapeutic goal as improved survival")
4
Study Objectives 1.To compare health-related quality of life outcomes among inoperable patients with severe aortic stenosis, treated with either TAVI or standard therapy 2.To examine whether the HRQOL benefits of TAVI are influenced by pre-specified patient characteristics 3.To provide key “input” data for ongoing economic evaluation of TAVI for the inoperable patient population

6
Patient Population Inclusion Criteria Severe, symptomatic AS (AVA 40 mmHg, or peak aortic jet velocity >4.0 m/sec) “Inoperable” Predicted risk of mortality or irreversible morbidity >50% as determined by 2 independent surgeons Exclusion Criteria (Selected) LVEF < 20% Severe (>3+) MR or AR Untreated CAD requiring revascularization Serum creatinine > 3.0 mg/dl or hemodialysis Recent MI (1 month), stroke or TIA (6 months) Life expectancy < 12 months
 Inoperable Predicted risk of mortality or irreversible morbidity >50% as determined by 2 independent surgeons Exclusion Criteria (Selected) LVEF < 20% Severe (>3+) MR or AR Untreated CAD requiring revascularization Serum creatinine > 3.0 mg/dl or hemodialysis Recent MI (1 month), stroke or TIA (6 months) Life expectancy < 12 months")
7
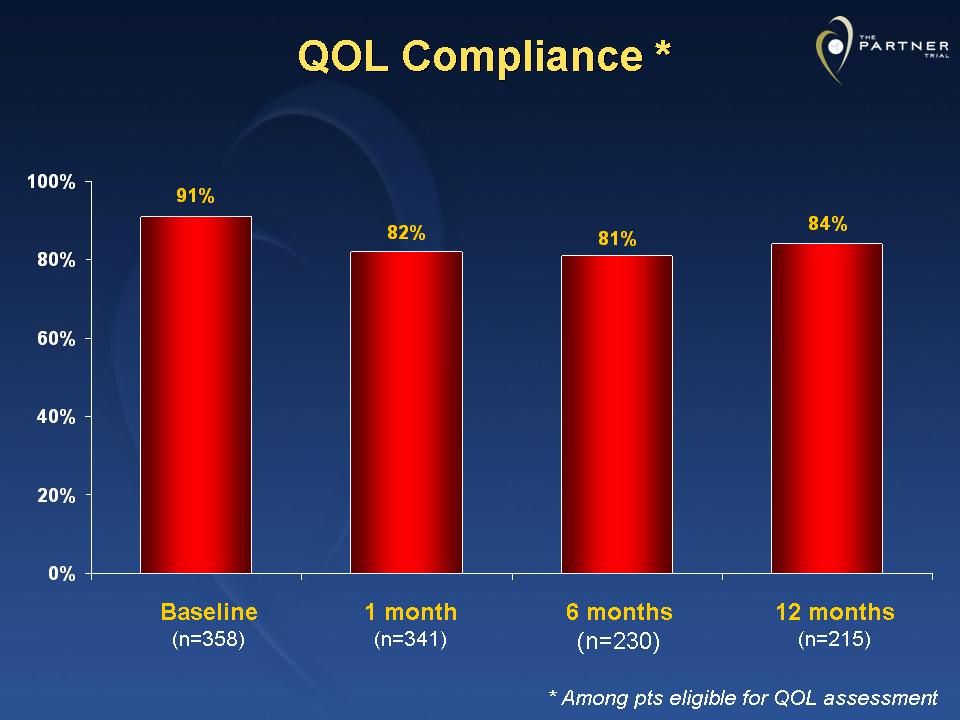
Methods: Quality of Life Assessments performed by self-administered questionnaires at baseline, 1, 6, & 12 months InstrumentDescription/Role Kansas City Cardiomyopathy Questionnaire (KCCQ) Heart Failure-specific QOL Domains: Symptoms, Physical Limitations, Quality of Life, Social Limitations Scores: 0-100 (higher = better) SF-12General physical and mental health Scores standardized such that mean=50, standard deviation=10 (higher = better) EQ-5D (EuroQOL)Generic instrument for assessment of utilities and QALYs Scores: 0-1 (0=death; 1=perfect health)
 Heart Failure-specific QOL Domains: Symptoms, Physical Limitations, Quality of Life, Social Limitations Scores: (higher = better) SF-12General physical and mental health Scores standardized such that mean=50, standard deviation=10 (higher = better) EQ-5D (EuroQOL)Generic instrument for assessment of utilities and QALYs Scores: 0-1 (0=death; 1=perfect health)")
8
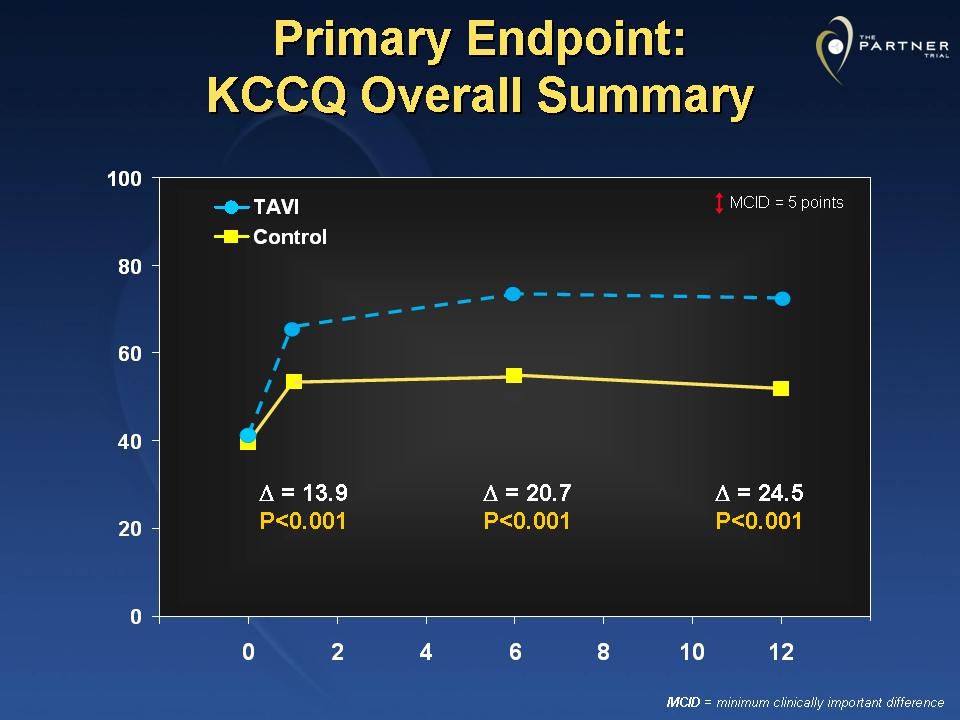
KCCQ: Development and Validation 23 items that measure 5 clinically relevant domains of health status from the patient’s perspective Symptoms Physical Limitation Quality of LifeSocial Limitation Self-Efficacy Individual scales combined into an global summary scale (KCCQ Overall Summary) Independently predictive of mortality and cost among patients with HF Green CP et al. JACC 2000; 35:1245-55 Soto G, et al. Circulation 2004;110:546-51

10
Statistical Analysis Primary QOL Endpoint = KCCQ Overall Summary Score All other QOL scales considered secondary endpoints Scores at each follow-up time point compared between groups by ANCOVA, adjusting for baseline Longitudinal analyses performed using random effect growth curve models, adjusting for treatment group (TAVI vs. control), time (linear, quadratic, cubic effects), and all potential 2-way and 3-way interactions
, time (linear, quadratic, cubic effects), and all potential 2-way and 3-way interactions.")
11
Baseline Characteristics TAVI(N=179)Control(N=179) Age (yrs) 83 983 8 Female gender 54.2%54.1% STS Risk Score 11.2 5.812.2 6.1 STS > 15% 21.2%24.7% Prior MI 18.6%26.4% Prior CABG 37.4%45.6% Cerebrovascular Dz 27.4%27.5% COPD (O2 dependent) 21.2%25.7% Creatinine > 2.0 mg/dl 5.6%9.6% Frailty 18.1%28.0% P=NS for all comparisons
Control(N=179) Age (yrs) 83 983 8 Female gender 54.2%54.1% STS Risk Score 11.2 6.1 STS > 15% 21.2%24.7% Prior MI 18.6%26.4% Prior CABG 37.4%45.6% Cerebrovascular Dz 27.4%27.5% COPD (O2 dependent) 21.2%25.7% Creatinine > 2.0 mg/dl 5.6%9.6% Frailty 18.1%28.0% P=NS for all comparisons")
13
Baseline QOL TAVI(N=179)Control(N=179) KCCQ Overall Summary 36.2 20.534.4 20.1 75-100 (~NYHA I) 4.1%3.8% 60-74 (~NYHA II) 10.6%7.0% 45-59 (~NYHA III) 15.9%17.8% 0-45 (~NYHA IV) 69.4%71.3% SF-12 Physical 28.2 7.727.7 6.9 SF-12 Mental 44.5 12.245.2 11.0 EQ-5D Utilities 0.59 0.230.57 0.23 P=NS for all comparisons
Control(N=179) KCCQ Overall Summary 36.2 (~NYHA I) 4.1%3.8% (~NYHA II) 10.6%7.0% (~NYHA III) 15.9%17.8% 0-45 (~NYHA IV) 69.4%71.3% SF-12 Physical 28.2 6.9 SF-12 Mental 44.5 11.0 EQ-5D Utilities 0.59 0.23 P=NS for all comparisons")
18
KCCQ-Summary: Significant Improvement * * Improvement ≥ 10 points vs. baseline among patients with available QOL data P <0.001 for all time points

19
KCCQ-Summary: Substantial Improvement * * Improvement ≥ 20 points vs. baseline among patients with available QOL data P <0.001 for all time points

20
KCCQ-Summary: Favorable Outcome * *Favorable Outcome = Alive and KCCQ-Summary Score improved ≥ 10 points vs. baseline P <0.001 for all time points

21
KCCQ-Summary: Excellent Outcome * * Excellent Outcome = Alive and KCCQ-Summary Score improved ≥ 20 points vs. baseline P <0.001 for all time points

23
Summary Among patients with severe, inoperable aortic stenosis, TAVI– as compared with non-operative therapy (including BAV in ~80%)-- led to substantial and sustained improvement across a broad range of health status and quality of life domains The extent of benefit was large for both disease- specific and general QOL and was consistent across all pre-specified subgroups KCCQ Summary Score 20-25 points (~2-level NHYA Class improvement on average) SF-12 Physical Component 5 points (~10 year reduction in effective age)
-- led to substantial and sustained improvement across a broad range of health status and quality of life domains The extent of benefit was large for both disease- specific and general QOL and was consistent across all pre-specified subgroups KCCQ Summary Score points (~2-level NHYA Class improvement on average) SF-12 Physical Component 5 points (~10 year reduction in effective age)")
24
Summary- 2 When QOL was considered along with survival, the number needed to treat to obtain an excellent outcome (i.e., 1-year survival with at least a 20 point improvement in the KCCQ ) was ~3 Clinical Implications: These findings add further support to the concept that TAVI should be considered an emerging standard of care for patients with severe aortic stenosis who are not candidates for surgical AVR
 was ~3 Clinical Implications: These findings add further support to the concept that TAVI should be considered an emerging standard of care for patients with severe aortic stenosis who are not candidates for surgical AVR")
25
Study Administration Co-Principal InvestigatorsCo-Principal Investigators Martin B. Leon, Craig R. Smith Columbia University Med Center Executive CommitteeExecutive Committee Martin B. Leon, Michael Mack, D. Craig Miller, Jeffrey W. Moses, Craig R. Smith, Lars G. Svensson, E. Murat Tuzcu, John G. Webb Data & Safety Monitoring BoardData & Safety Monitoring Board Chairman: Joseph P. Carrozza Tufts University School of Med Clinical Events CommitteeClinical Events Committee Chairman: John L. Petersen Duke University Med Center Echo Core LaboratoryEcho Core Laboratory Chairman: Pamela C. Douglas Duke University Med Center Quality of Life and Cost Effectiveness AssessmentsQuality of Life and Cost Effectiveness Assessments Chairman: David J. Cohen Mid-America Heart Inst, KC Independent Biostatistical Core LaboratoryIndependent Biostatistical Core Laboratory Chairman: Stuart Pocock London School of Hygiene & Tropical Medicine William N. Anderson Publications CommitteePublications Committee Co-Chairman: Jeffrey W. Moses, Lars G. Svensson SponsorSponsor Edwards Lifesciences: Jodi J. Akin

26
Enrollment by Site - Inoperable Cedars-Sinai Medical Ctr Los Angeles, CA G. Fontana, R. Makkar 36 Columbia University New York City, NY M. Leon, C. Smith 33 Medical City Dallas Dallas, TX D. Brown, M. Mack 21 Emory University Atlanta, GA P. Block, R. Guyton 43 Washington Hospital Ctr District of Columbia P. Corso, A. Pichard 50 Cleveland Clinic Found Cleveland, OH L. Svensson, M. Tuzcu 45 University of Pennsylvania University of Pennsylvania Philadelphia, PA J. Bavaria, H. Herrmann 21 University of Miami Miami, FL W. O’Neill, D. Williams 15 Barnes-Jewish Hospital St. Louis, MO R. Damiano, J, Lasala 12 St. Paul's Hospital Vancouver, BC, Canada A. Cheung, J. Webb 22 Stanford University Palo Alto, CA C. Miller, A. Yeung 6 Northwestern University Chicago, IL C. Davidson, P. McCarthy 6

27
St. Luke’s Hospital Kansas City, MO K. Allen, D. Cohen 5 Mass General Hospital Boston, MA I. Palacios, G. Vlahakis 2 Mayo Clinic Rochester, MN C. Rihal, T. Sundt 7 Scripps Clinic La Jolla, CA S. Brewster, P. Teirstein 8 Univ of Washington Seattle, WA M. Reisman, E. Verrier 8 Northshore Univ Health Sys Evanston, IL J. Alexander, T. Feldman 10 Universitaire de Quebec Laval, Quebec, CA D. Doyle, J. Rodes-Cabau 4 Herzzentrum Leipzig Leipzig, Germany F. Mohr, G. Schuler 2 University of Virginia Charlottesville, VA I. Kron, S. Lim 0 Brigham & Women’s Hosp Boston, MA M. Davidson, A. Eisenhauer 0 Cornell University New York City, NY K. Krieger, C. Wong 0 Ochsner Foundation New Orleans, LA E. Parrino, S. Ramee 0 Intermountain Med Center Salt Lake City, UT K. Jones, B. Whisenant 0 Toronto General Hospital Toronto, Ontario, CA C. Feindel, E. Horlick 2 Enrollment by Site - Inoperable

Similar presentations