Download presentation
Presentation is loading. Please wait.

1
Chapter 10: Tissue Response to Injury

2
Inflammatory Response
Acute Inflammation Short onset and duration Change in hemodynamics, production of exudate, granular leukocytes Chronic Inflammation Long onset and duration Presence of non-granular leukocytes and extensive scar tissue

3
Cardinal Signs of Inflammation
Rubor (redness) Tumor (swelling) Color (heat) Dolor (pain) Functio laesa (loss of function)
 Tumor (swelling) Color (heat) Dolor (pain) Functio laesa (loss of function)")
4
Phases of the Inflammatory Response
(3 separate phases) 1. Acute phase 2. Repair phase 3. Remodeling phase
 1. Acute phase. 2. Repair phase. 3. Remodeling phase.")
5
Phase I: Acute Phase Initial reaction to an injury occurring 3 hours to 4 days following injury Goal Protect Localize Decrease injurious agents Prepare for healing and repair Caused by trauma, chemical agents, thermal extremes, pathogenic organisms

6
External and internal injury result in tissue death and cell death
Decreased oxygen to area increases cell death Phagocytosis will add to cell death due to excess digestive enzymes Rest, ice, compression & elevation are critical to limiting cell death

7
First hour Vasoconstriction and coagulation occur to seal blood vessels and chemical mediators are released Immediately followed by vasodilation or blood vessel Second hour Vasodilation decreases blood flow, increased blood viscosity resulting in edema (swelling)
")
8
Second hour (continued)
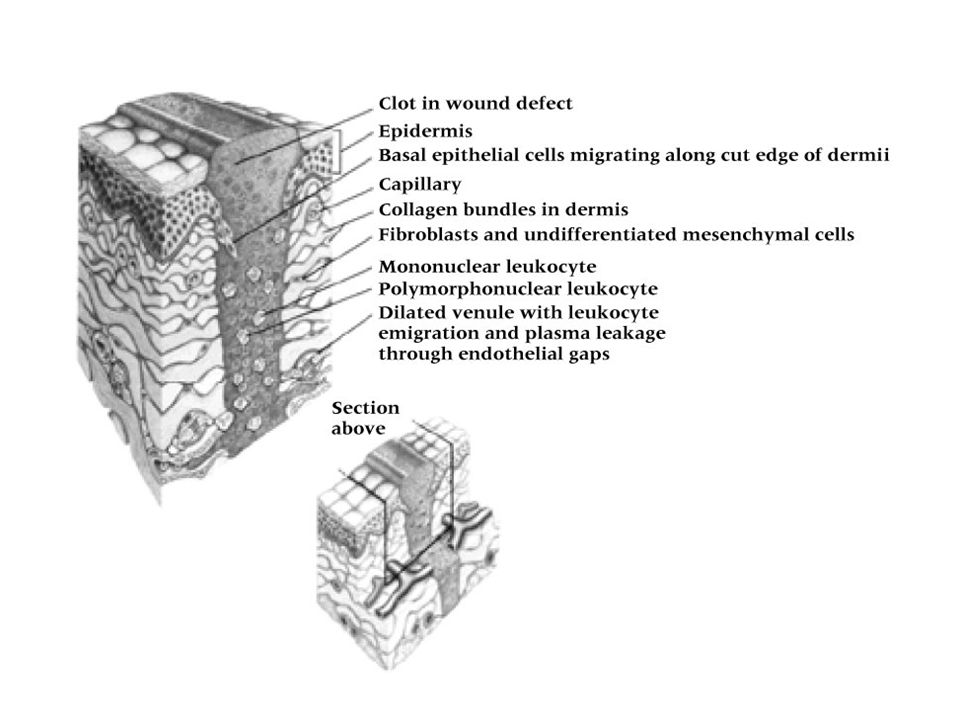
Exudate increases (high concentration of RBC’s) due to increased vessel permeability Permeability changes generally occur in capillary and venules Margination occurs causing leukocytes to fill the area and line endothelial walls Through diapedesis and chemotaxis leukocytes move to injured area
 due to increased vessel permeability. Permeability changes generally occur in capillary and venules. Margination occurs causing leukocytes to fill the area and line endothelial walls. Through diapedesis and chemotaxis leukocytes move to injured area.")
9
Cellular response Mast cells (connective tissue cells) and leukocytes (basophils, monocytes, neutrophils) enter area Mast cells with heparin and histamine serve as first line of defense Basophils provide anticoagulant Neutrophils and monocytes are responsible for small and large particles undergoing phagocytosis - ingestion of debris and bacteria

10
Cellular mediation Histamine provided by platelets, mast cells and basophils to enhance permeability and arterial dilation Serotonin provides for vasoconstriction Bradykinin is a plasma protease that enhance permeability and causes pain. Heparin is provided by mast cells and basophils to prevent coagulation Leukotrienes and prostaglandins are located in cell membranes and develop through the arachadonic acid cascade Leukotrienes alter permeability Prostaglandin add and inhibit inflammation

11
Complimentary systems
Enzymatic proteins that destroy bacteria and other cells through their impact on cell lysis Bleeding and exudate Amount dependent on damage Initial stage: thromboplastin is formed Second stage: Prothrombin is converted to thrombin due to interaction with thromboplastin Third stage: thrombin changes from soluble fibrinogen to insoluble fibrin coagulating into a network localizing the injury

13
Phase II: Repair Phase Phase will extent from 48 hours to 6 weeks following cleaning of fibrin clot, erythrocytes, and debris Repaired through 3 phases Resolution (little tissue damage and normal restoration) Restoration (if resolution is delayed) Regeneration (replacement of tissue by same tissue)
 Restoration (if resolution is delayed) Regeneration (replacement of tissue by same tissue)")
15
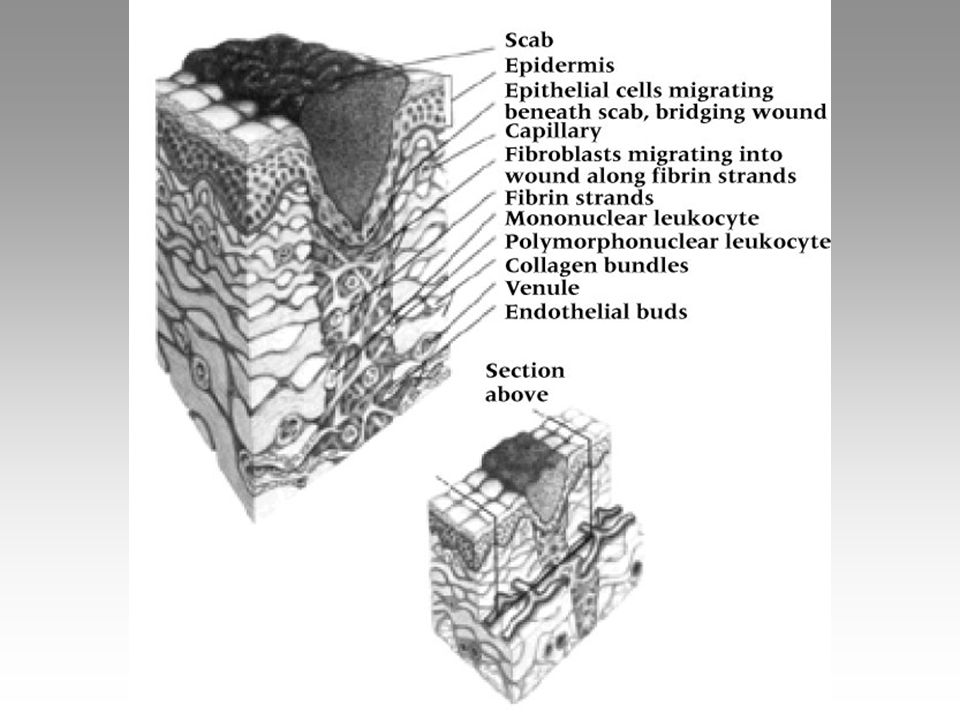
Scar formation Less viable than normal tissue, may compromise healing
Firm, inelastic mass devoid of capillary circulation Develops from exudate with high protein and debris levels resulting in granulation tissue Invaded by fibroblasts and and collagen forming a dense scar and while normally requiring 3-14 weeks may require 6 months to contract

16
Primary healing (healing by first intention)
Closely approximated edges with little granulation tissue production Secondary healing (heal by secondary intention) Gapping, tissue loss, and development of extensive granulation tissue Common in external lacerations and internal musculoskeletal injuries
 Gapping, tissue loss, and development of extensive granulation tissue. Common in external lacerations and internal musculoskeletal injuries.")
17
Regeneration Related to health, nutrition and tissue type
Dependent on levels of: debris (phagocytosis) endothelial production (hypoxia and macrophages stimulate capillary buds) production of fibroblasts (revascularization allows for enhanced fibroblast activity and collagen production which is tied to Vitamin C, lactic acid, and oxygen
 endothelial production (hypoxia and macrophages stimulate capillary buds) production of fibroblasts (revascularization allows for enhanced fibroblast activity and collagen production which is tied to Vitamin C, lactic acid, and oxygen.")
18
Phase III: Remodeling Overlaps repair and regeneration
First 3-6 weeks involves laying down of collagen and strengthening of fibers 3 months to 2 years allowed for enhanced scar tissue strength Balance must be maintained between synthesis and lysis Take into consideration forces applied and immobilization/mobilization time frames relative to tissue and healing time

20
Chronic Inflammation Result of failed acute inflammation resolution within one month termed subacute inflammation Inflammation lasting months/years termed chronic Results from repeated microtrauma and overuse Proliferation of connective tissue and tissue degeneration

21
Characteristics of Chronic Inflammation
Proliferation of connective tissue and tissue degeneration Presence of lymphocytes, plasma cell, macrophages(monocytes) in contrast to neutrophils (during acute conditions) Major chemicals include Kinins (bradykinin) - responsible for vasodilation, permeability and pain Prostaglandin - responsible for vasodilation but can be inhibited with aspirin and NSAID’s
 in contrast to neutrophils (during acute conditions) Major chemicals include. Kinins (bradykinin) - responsible for vasodilation, permeability and pain. Prostaglandin - responsible for vasodilation but can be inhibited with aspirin and NSAID’s.")
22
Factors That Impede Healing
Extent of injury Edema Hemorrhage Poor Vascular Supply Separation of Tissue Muscle Spasm Atrophy Corticosteroids Keloids and Hypertrophic Scars Infection Humidity, Climate, Oxygen Tension Health, Age, and Nutrition

23
Soft Tissue Healing Cell structure/function
All organisms composed of cells Properties of soft tissue derived from structure and function of cells Cells consist of nucleus surrounded by cytoplasm and encapsulated by phospholipid cell membrane Nucleus contains chromosomes (DNA) Functional elements of cells (organelles) include mitochondria, ribosomes, endoplasmic reticulum, Golgi apparatus & centrioles
 Functional elements of cells (organelles) include mitochondria, ribosomes, endoplasmic reticulum, Golgi apparatus & centrioles.")
24
Tissues of the Body Bone - not classified as soft tissue
4 types of soft tissue Epithelial tissue Skin, vessel & organ linings Connective tissue Tendons, ligaments, cartilage, fat, blood, and bone Muscle tissue Skeletal, smooth, cardiac muscle Nerve tissue Brain, spinal cord & nerves

25
Soft Tissue Adaptations
Metaplasia - transformation of tissue from one type to another that is not normal for that tissue Dysplasia - abnormal development of tissue Hyperplasia- excessive proliferation of normal cells in normal tissue arrangement Atrophy- a decrease in the size of tissue due to cell death and re-absorption or decreased cell proliferation Hypertrophy - an increase in the size of tissue without necessarily changing the number of cells

26
Cartilage Healing Limited capacity to heal
Little or no direct blood supply Chrondrocyte and matrix disruption result in variable healing Articular cartilage that fails to clot and has no perichondrium heals very slowly If area involves subchondral bone (enhanced blood supply) granulation tissue is present and healing proceeds normally
 granulation tissue is present and healing proceeds normally.")
27
Ligament Healing Follows similar healing course as vascular tissue
Proper care will result in acute, repair, and remodeling phases in same time required by other vascular tissue Repair phase will involve random laying down of collagen which, as scar forms, will mature and realign in reaction to joint stresses and strain Full healing may require 12 months

28
Skeletal Muscle Healing
Skeletal muscle cannot undergo mitotic activity to replace injured cells New myofibril regeneration is minimal Healing and repair follow the same course as other soft tissues developing tensile strength (Wolff’s Law)
")
29
Nerve Healing Cannot regenerate after injury
Regeneration can take place within a nerve fiber Proximity of injury to nerve cell makes regeneration more difficult For regeneration, optimal environment is required Rate of healing occurs at 3-4 mm per day Injured central nervous system nerves do not heal as well as peripheral nerves

30
Modifying Soft-Tissue Healing
Varying issues exist for all soft tissues relative to healing (cartilage, muscle, nerves) Blood supply and nutrients is necessary for all healing Healing in older athletes or those with poor diets may take longer Certain organic disorders (blood conditions) may slow or inhibit the healing process
 Blood supply and nutrients is necessary for all healing. Healing in older athletes or those with poor diets may take longer. Certain organic disorders (blood conditions) may slow or inhibit the healing process.")
31
Management Concepts Drug utilization
Anitprostaglandin agents used to combat inflammation Non-steroidal anti-inflammatory agents (NSAID’s) Medications will work to decrease vasodilatation and capillary permeability
 Medications will work to decrease vasodilatation and capillary permeability.")
32
Therapeutic Modalities
Thermal agents are utilized Heat stimulates acute inflammation (but works as a depressant in chronic conditions) Cold is utilized as an inhibitor Electrical modalities Treatment of inflammation Ultrasound, microwave, electrical stimulation (includes transcutaneous electrical muscle stimulation and electrical muscle stimulation
 Cold is utilized as an inhibitor. Electrical modalities. Treatment of inflammation. Ultrasound, microwave, electrical stimulation (includes transcutaneous electrical muscle stimulation and electrical muscle stimulation.")
33
Therapeutic Exercise Major aim involves pain free movement, full strength power, and full extensibility of associated muscles Immobilization, while sometimes necessary, can have a negative impact on an injury Adverse biochemical changes can occur in collagen Early mobilization (that is controlled) may enhance healing
 may enhance healing.")
34
Fracture Healing Potential serious bone fractures are part of athletics Time is necessary for proper bone union to occur and is often out of the control of a physician Conservative treatment will be necessary for adequate healing to occur

35
Bone undergoes constant remodeling through osteocyte activity
Osteocytes cellular component of bone Osteoblasts are responsible for bone formation while osteoclasts resorb bone Cambium (periosteum) A fibrous covering involved in bone healing Vascular and very dense Inner cambium less vascular and more cellular. Provides attachments for muscle, ligaments and tendons
 A fibrous covering involved in bone healing. Vascular and very dense. Inner cambium. less vascular and more cellular. Provides attachments for muscle, ligaments and tendons.")
36
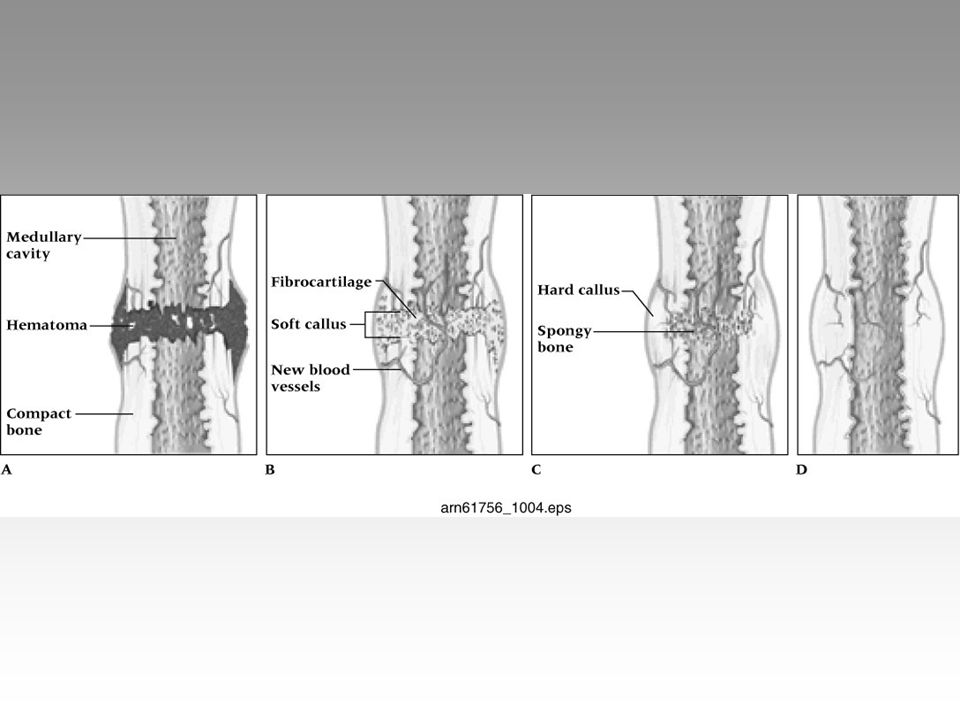
Acute Fracture of Bone Follows same three phases of soft tissue healing Less complex process Acute fractures have 5 stages Hematoma formation Cellular proliferation Callus formation Ossification Remodeling

38
Hematoma Formation Trauma to the periosteum and surrounding soft tissue occurs due to the initial bone trauma During the first 48 hours a hematoma within the medullary cavity and the surrounding tissue develops Blood supply is disrupted by clotting vessels and cellular debris Dead bone results in an inflammatory response (vasodilation, exudate cell migration)
")
39
Cellular Formation Granulation forms constructing fibrous union between fractured ends Capillary buds allow endosteal cells influx from cambium layer Cells evolve from fibrous callus to cartilage, to woven bone High oxygen tension = fibrous tissue Low oxygen tension = cartilage tissue Bone growth will occur with optimal oxygen tension and compression

40
Callus Formation Soft callus is a random network of woven bone
Osteoblasts fill the internal and external calluses to immobilize the site Calluses are formed by bone fragments that bridge the fracture gap The internal callus creates a rigid immobilization early

41
Hard callus formation occurs after 3-4 weeks and lasts 3-4 months
Hard callus is a gradual connection of bone filaments to the woven bone Less than ideal immobilization produces a cartilagenous union instead of a bony union

42
Ossification Adequate immobilization and compression will result in new Haversian systems developing Haversian canals allow for the laying down of primary bone Ossification is complete when bone has been laid down and the excess callus has been resorbed by osteoclasts.

43
Remodeling Occurs following callus resorption and trabecular bone is laid along lines of stress Bioelectric stimulation plays a major role in completing the remodeling process Osteoblasts are attracted to the electronegative (concave/compression) side Osteoclasts are attracted to the electropositive (convex/tension) side The process is complete when the original shape is achieved or the structure can withstand imposed stresses
 side. Osteoclasts are attracted to the electropositive (convex/tension) side. The process is complete when the original shape is achieved or the structure can withstand imposed stresses.")
44
Acute Fracture Management
Must be appropriately immobilized, until X-rays reveal the presence of a hard callus Fractures can limit participation for weeks or months A clinician must be certain that the following areas do not interfere with healing Poor blood supply Poor immobilization Infection

45
Poor blood supply Poor immobilization
Bone may die and union/healing will not occur (avascular necrosis) Common sites include: Head of femur, navicular of the wrist, talus, and isolated bone fragments Relatively rare in healthy, young athletes except in navicular of the wrist Poor immobilization Result of poor casting allowing for motion between bone parts May prevent proper union or result in bony deformity
 Common sites include: Head of femur, navicular of the wrist, talus, and isolated bone fragments. Relatively rare in healthy, young athletes except in navicular of the wrist. Poor immobilization. Result of poor casting allowing for motion between bone parts. May prevent proper union or result in bony deformity.")
46
Infection May interfere with normal healing, particularly with compound fractures Severe streptococcal and staphylococcal infections Modern antibiotics has reduced the risk of infections Closed fractures are not immune to infections within the body or blood If soft tissue alters bone positioning, surgery may be required to ensure proper union

47
Healing of Stress Fractures
Result of cyclic forces, axial compression or tension from muscle pulling Electrical potential of bone changes relative to stress (compression, tension, or torsional) Constant stress axially or through muscle activity can impact bone resorption, leading to microfracture
 Constant stress axially or through muscle activity can impact bone resorption, leading to microfracture.")
48
If osteoclastic activity is not in balance with oesteoblastic activity bone becomes more susceptible to fractures To treat stress fractures a balance between osteoblast and osteoclast activity must be restored Early recognition is necessary to prevent complete cortical fractures Decreased activity and elimination of factors causing excess stress will be necessary to allow for appropriate bone remodeling

49
Pain Major indicator of injury Pain is individual and subjective
Factors involved in pain Anatomical structures Physiological reactions Psychological, social, cultural and cognitive factors

50
Nociception Pain receptors -free nerve endings sensitive to extreme mechanical, thermal and chemical energy Located in meninges, periosteum, skin, teeth, and some organs Pain information transmitted to spinal cord via myelinated C fibers and A delta fibers Nociceptor stimulation results in release of substance P

51
Signal travels along afferent nerves to the spinal cord
A delta fiber (fast) transmit information to the thalamus concerning location of pain and perception of pain being sharp, bright or stabbing C fibers (slower conduction velocity) deal with diffused, dull, aching and unpleasant pain C fibers signal also passed to limbic cortex providing emotional component to pain Nociceptive stimuli is at or close to an intensity which would result in tissue injury
 transmit information to the thalamus concerning location of pain and perception of pain being sharp, bright or stabbing. C fibers (slower conduction velocity) deal with diffused, dull, aching and unpleasant pain. C fibers signal also passed to limbic cortex providing emotional component to pain. Nociceptive stimuli is at or close to an intensity which would result in tissue injury.")
52
Endogenous Analgesics
Nervous system is electrochemical in nature Chemicals called neurotransmitters are released by presynaptic cell Two types mediate pain Endorphins Seretonin Neurotransmitters release stimulated by noxious stimuli- resulting in activation of pain inhibition transmission

53
Analgesia is the result of opioids release
Stimulation of periaqueductal gray matter (PGA) and raphe nucleus of pons and medulla cause analgesia Analgesia is the result of opioids release Morphine like substance manufactured in the PGA and CNS Endorphins and enkephalins Other pain modulators Norepinephrine (noradrenergic Seretonin also will serve as neuromodulator
 and raphe nucleus of pons and medulla cause analgesia. Analgesia is the result of opioids release. Morphine like substance manufactured in the PGA and CNS. Endorphins and enkephalins. Other pain modulators. Norepinephrine (noradrenergic. Seretonin also will serve as neuromodulator.")
54
Pain Categories Pain sources Fast versus slow pain
Acute versus chronic Projected or referred pain

55
Pain sources Cutaneous, deep somatic, visceral and psychogenic
Cutaneous pain is sharp, bright and burning with fast and slow onset Deep somatic pain originates in tendons, muscles, joints, periosteum and blood vessels Visceral pain begins in organs and is diffused at first and may become localized Psychogenic pain is felt by the individual but is emotional rather than physical

56
Acute versus Chronic Pain
Fast versus Slow Pain Fast pain localized and carried through A-delta axons Slow pain is perceived as aching, throbbing, or burning (transmitted through C fibers) Acute versus Chronic Pain Acute pain is less than six months in duration Chronic pain last longer than six months Chronic pain classified by IASP as pain continuing beyond normal healing time
 Acute versus Chronic Pain. Acute pain is less than six months in duration. Chronic pain last longer than six months. Chronic pain classified by IASP as pain continuing beyond normal healing time.")
57
Projected (Referred) Pain
Pain which occurs away from actual site of injury/irritation Unique to each individual and case May elicit motor and/or sensory response A-alpha fibers are sensitive to pressure and can produce paresthesia Three types of referred pain include: myofascial, sclerotomic, and dermatomic

58
Myofascial Pain Trigger points or small hyperirritable areas within muscle resulting in bombardment of CNS Acute and chronic pain can be associated with myofascial points Often described as fibrositis, myositis, myalgia, myofasciitis and muscular strain Two types of trigger points (active and latent) Active points cause obvious complaint Latent points are dormant potentially causing loss of ROM
 Active points cause obvious complaint. Latent points are dormant potentially causing loss of ROM.")
59
Sclerotomic and dermatomic pain
Trigger points do not follow patterns Trigger point area referred to as reference zone which may or may not be proximal to the point of irritation Sclerotomic and dermatomic pain Deep pain with slow or fast characteristics May originate from sclerotomic, myotomic or dermatomic nerve irritation/injury Sclerotomic pain transmitted by C fibers causing deep aching and poorly localized pain Can be projected to multiple areas of brain causing depression, anxiety, fear or anger

60
Autonomic changes result (vasomotor control, BP and sweating
Dermatomic pain (irritation of A-delta fibers) is sharp and localized Projects to the thalamus and cortex directly
 is sharp and localized. Projects to the thalamus and cortex directly.")
61
Gate Theory Area in dorsal horn of spinal cord causes inhibition of pain impulses ascending to cortex T-cells will transmit signals to brain Substantia gelatinosa functions as gate determining if stimulus sent to T-cells Pain stimuli exceeding threshold results in pain perception Stimulation of large fast nerves can block signal of small pain fiber input Rationale for TENS, accupressure/puncture, thermal agents and chemical skin irritants

62
Central Biasing Theory

63
Release of B-Endorphins

64
Variation of Pain Sensitivity
Hyperesthesia, paresthia or analgesia Pain modulation Mixture of physical and psychological factors Pain management is a challenge to treat Generally acute pain management in athletic training setting

65
Pain assessment Pain Treatment
Self report is the best reflection of pain and discomfort Assessment techniques include: visual analog scales (0-10, marked no pain to severe pain) verbal descriptor scales (marked none, slight, moderate, and severe) Pain Treatment Must break pain-spasm-hypoxia-pain cycle through treatment Agents used; heat/cold, electrical stimulation-induced analgesia, pharmacological agents
 verbal descriptor scales (marked none, slight, moderate, and severe) Pain Treatment. Must break pain-spasm-hypoxia-pain cycle through treatment. Agents used; heat/cold, electrical stimulation-induced analgesia, pharmacological agents.")
66
Heat/Cold Induced analgesia
Heat increases circulation, blood vessel dilation, reduces nociception and ischemia caused by muscle spasm Cold applied for vasoconstriction and prevention of extravasation of blood into tissue Pain reduced through decrease in swelling and spasm Induced analgesia Utilize electrical modalities to reduce pain TENS and acupuncture commonly used to target Gate Theory

67
Pharmacological Agents
Oral, injectable medications Commonly analgesics and anti-inflammatory agents

68
Psychological Aspects of Pain
Pain can be subjective and psychological Pain thresholds vary per individual Pain is often worse at night due to solitude and absence of external distractions Personality differences can also have an impact A number of theories relative to pain exist and it physiological and psychological components Athlete, through conditioning are often able to endure pain and block sensations of minor injuries

Similar presentations















>")




