Download presentation
Presentation is loading. Please wait.

1
Goals Understand the differences between Hodgkin Lymphoma and non-Hodgkin Lymphoma Clinically and biologically Understand the differences between aggressive NHL and indolent NHL

2
Definition of Lymphoma
C Definition of Lymphoma Heterogeneous group of lymphoproliferative malignancies Results from clonal expansion of tumor cells derived from B, T, or NK cells 85%-90% in the US are derived from B cells Variable clinical presentations Range from asymptomatic pick up on routine blood work to painless adenopathy to an emergent medical problem Pain, failure to thrive, organ failure Characterized by variable natural histories and therapeutic responses Non-Hodgkin’s lymphoma (NHL) is a heterogeneous group of lymphoproliferative malignancies. More than 30 different subtypes of NHL have been identified and categorized according to several prognostic factors, including size, growth rate, and anatomic site. NHL results from clonal expansion of tumor cells derived from B, T, or natural killer (NK) cells. Most NHLs, about 85% to 90% in the United States, are derived from B cells. NHLs are characterized by variable natural histories and therapeutic responses. The clinical courses of NHLs vary greatly, ranging from indolent to rapidly fatal. Although the etiology of NHL is unknown, at least 4 possible factors may contribute to its development: genetic factors, autoimmune disorders, viral infection (eg, HIV), and exposure to carcinogens (eg, herbicides or pesticides). NHL can arise from central and peripheral lymphoid tissues and can spread to other organ systems. Central lymphoid tissue consists of the bone marrow and the thymus; peripheral lymphoid tissue consists of blood, spleen, lymph nodes, and mucosa-associated lymphoid tissue (MALT). Recent advances in molecular and cellular biology have greatly contributed to our understanding of the various forms of NHL and, as we shall discuss, to the development of novel therapeutic strategies. Harris NL, Stein H, Coupland SE, et al. New approaches to lymphoma diagnosis. Hematology (Am Soc Hematol Educ Program). 2001: Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Skarin AT, Dorfman DM. Non-Hodgkin’s lymphomas: current classification and management. CA Cancer J Clin. 1997;47:
 is a heterogeneous group of lymphoproliferative malignancies. More than 30 different subtypes of NHL have been identified and categorized according to several prognostic factors, including size, growth rate, and anatomic site. NHL results from clonal expansion of tumor cells derived from B, T, or natural killer (NK) cells. Most NHLs, about 85% to 90% in the United States, are derived from B cells. NHLs are characterized by variable natural histories and therapeutic responses. The clinical courses of NHLs vary greatly, ranging from indolent to rapidly fatal. Although the etiology of NHL is unknown, at least 4 possible factors may contribute to its development: genetic factors, autoimmune disorders, viral infection (eg, HIV), and exposure to carcinogens (eg, herbicides or pesticides). NHL can arise from central and peripheral lymphoid tissues and can spread to other organ systems. Central lymphoid tissue consists of the bone marrow and the thymus; peripheral lymphoid tissue consists of blood, spleen, lymph nodes, and mucosa-associated lymphoid tissue (MALT). Recent advances in molecular and cellular biology have greatly contributed to our understanding of the various forms of NHL and, as we shall discuss, to the development of novel therapeutic strategies. Harris NL, Stein H, Coupland SE, et al. New approaches to lymphoma diagnosis. Hematology (Am Soc Hematol Educ Program). 2001: Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Skarin AT, Dorfman DM. Non-Hodgkin’s lymphomas: current classification and management. CA Cancer J Clin. 1997;47:")
3
Age at Diagnosis for Hodgkin’s and Non-Hodgkin’s Lymphoma
~56,390 NHL cases/y ~7,350 HD cases/y NHL Cases/100,000 The age at diagnosis for Hodgkin’s lymphoma and NHL, measured in cases per 100,000 population, are compared with one another. The data, derived from the Surveillance, Epidemiology, and End Results (SEER) database, are for patients diagnosed between 1997 and 2001. There are approximately 56,390 new cases of NHL per year and 7,350 cases of Hodgkin’s lymphoma per year. NHL is a disease predominantly of the elderly, whereas Hodgkin’s lymphoma has a slightly bimodal distribution. Hodgkin’s Age at diagnosis (y) Data for diagnoses from 1997 to 2001. At: Accessed March 23, 2005. Available at: Accessed March 23, 2005.
 database, are for patients diagnosed between 1997 and There are approximately 56,390 new cases of NHL per year and 7,350 cases of Hodgkin’s lymphoma per year. NHL is a disease predominantly of the elderly, whereas Hodgkin’s lymphoma has a slightly bimodal distribution. Hodgkin’s. Age at diagnosis (y) Data for diagnoses from 1997 to At: Accessed March 23, Available at: Accessed March 23,")
4
Non-Hodgkin’s Lymphoma: Epidemiology
Estimated annual incidence ~4% compound annual increase in incidence Non-Hodgkin’s lymphoma (NHL) is a heterogeneous group of B- and T-cell malignancies with diverse growth patterns and responses to therapy. Although some types of NHL are among the most common childhood cancers, more than 95% of cases occur in adults. The annual report of cancer statistics issued by the American Cancer Society estimates that 56,390 new cases of NHL will be diagnosed in the United States in the year NHL currently ranks fifth and sixth for newly diagnosed cancers among men and women, respectively, and it accounts for 5% of all cancer-related deaths in the United States. The incidence of NHL in the United States over the last 15 years has increased by approximately 4% annually, despite the decline in age-adjusted incidence rates for all cancers combined. NHL is one of the most rapidly rising cancers; its incidence has doubled since the early 1970s. Potential explanations for the increased incidence of NHL include infectious agents, congenital and acquired immunodeficiency syndromes, environmental exposure, and genetic factors. Year Adapted from Greenlee et al. CA Cancer J Clin. 2001;51:15. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10. Adapted from Greenlee et al. CA Cancer J Clin. 2001;51:15. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10.
 is a heterogeneous group of B- and T-cell malignancies with diverse growth patterns and responses to therapy. Although some types of NHL are among the most common childhood cancers, more than 95% of cases occur in adults. The annual report of cancer statistics issued by the American Cancer Society estimates that 56,390 new cases of NHL will be diagnosed in the United States in the year NHL currently ranks fifth and sixth for newly diagnosed cancers among men and women, respectively, and it accounts for 5% of all cancer-related deaths in the United States. The incidence of NHL in the United States over the last 15 years has increased by approximately 4% annually, despite the decline in age-adjusted incidence rates for all cancers combined. NHL is one of the most rapidly rising cancers; its incidence has doubled since the early 1970s. Potential explanations for the increased incidence of NHL include infectious agents, congenital and acquired immunodeficiency syndromes, environmental exposure, and genetic factors. Year. Adapted from Greenlee et al. CA Cancer J Clin. 2001;51:15. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10. Adapted from Greenlee et al. CA Cancer J Clin. 2001;51:15. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10.")
5
Hodgkin’s Disease

6
Hodgkin Biology RS is a “crippled” germinal center B cell
does not have normal B cell surface antigens micromanipulation of single RS followed by PCR demonstrates clonally rearranged, but non functional immunoglobulin genes somatic mutations result in stop codon (no sIg) no apoptotic death malignant transformation unclear how this occurs; ? EBV unclear how cells end up with RS phenotype
 no apoptotic death malignant transformation. unclear how this occurs; EBV. unclear how cells end up with RS phenotype.")
7
Hodgkin’s Disease Clinical features Often seen in young adults
Wide variety of presentations B symptoms (fevers, night sweats, wt loss) Pruritis Cough/SOB Pain Painless adenopathy
 Pruritis. Cough/SOB. Pain. Painless adenopathy.")
8
Hodgkin’s Disease Approach to the Patient staging evaluation H & P
CBC, diff, plts ESR, LDH, albumin, LFT’s, Cr CT scans chest/abd/pelvis bone marrow evaluation PET scan in selected cases

9
Ann Arbor Staging System for Hodgkin's Disease and Non-Hodgkin's Lymphoma
Historically, this staging methodology was designed for Hodgkin’s disease but has been adapted to NHL. Staging defines the extent of a cancer along three axes: tumor (T); node (N); and metastasis (M). The rationale behind a staging system is to accomplish the following: Plan treatment strategies Help evaluate the treatment results Standardize information to facilitate exchanges between health-care professionals and treatment centers Formulate a more accurate prognosis Promote the continuity of cancer investigation The Ann Arbor Staging System is the most commonly used in NHL. It is divided into four stages (I to IV), according to nodal and extralymphatic involvement, and subclassified into A and B categories. A designates the absence of the so-called B symptoms. B signals their presence. The B symptoms are as follows: Unexplained loss of more than 10% of body weight in the 6 months before diagnosis Unexplained fever with temperatures above 38o Celsius Drenching night sweats Skarin AT, ed. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology. Philadelphia: Lippincott; New York: Gower Medical Pub; 1991. Available at Accessed 6/25/02. Stage I Stage II Stage III Stage IV Reprinted with permission. Adapted from Skarin. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology
; node (N); and metastasis (M). The rationale behind a staging system is to accomplish the following: Plan treatment strategies. Help evaluate the treatment results. Standardize information to facilitate exchanges between health-care professionals and treatment centers. Formulate a more accurate prognosis. Promote the continuity of cancer investigation. The Ann Arbor Staging System is the most commonly used in NHL. It is divided into four stages (I to IV), according to nodal and extralymphatic involvement, and subclassified into A and B categories. A designates the absence of the so-called B symptoms. B signals their presence. The B symptoms are as follows: Unexplained loss of more than 10% of body weight in the 6 months before diagnosis. Unexplained fever with temperatures above 38o Celsius. Drenching night sweats. Skarin AT, ed. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology. Philadelphia: Lippincott; New York: Gower Medical Pub; Available at Accessed 6/25/02. Stage I Stage II Stage III Stage IV. Reprinted with permission. Adapted from Skarin. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology")
10
Hodgkin’s Disease Typical staging results
Most often disease is localized to above the diaphragm Common to have extensive mediastinal disease Tends to spread to contiguous nodal groups Unlike NHL

11
Approach to the Patient
Hodgkin’s Disease approach dictated mainly by where the disease is located rather (results of staging) than the exact histologic subtype NHL approach is often dictated more by the histologic subtype than the results of staging
 than the exact histologic subtype. NHL. approach is often dictated more by the histologic subtype than the results of staging.")
12
Hodgkin Lymphoma: Treatment of limited stage disease

13
Hodgkin Lymphoma: Prognostic Factors

14
Hodgkins Disease Summary
B cell lymphoma several histologic subtypes Generally does not affect the approach to the patient Reed-Sternberg Cells Tends to occur in young adults Mediastinal disease common Spreads to contiguous nodes Common to have a “localized” presentation Highly curable with current treatments

15
Non-Hodgkin’s Lymphoma
30ish histologic subtypes B cell (85%), T cell, NK cell Histologic subtype dictates the approach to the patient Median age at diagnosis 60 Often widespread disease at diagnosis Wide variation in outcome Some cases rapidly fatal Some cases readily curable Some cases incurable but patient can live for many years with good quality of life
, T cell, NK cell. Histologic subtype dictates the approach to the patient. Median age at diagnosis 60. Often widespread disease at diagnosis. Wide variation in outcome. Some cases rapidly fatal. Some cases readily curable. Some cases incurable but patient can live for many years with good quality of life.")
16
WHO Classification: B-Cell Malignancies
Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma Mature (peripheral) B-cell neoplasms B-cell chronic lymphocytic leukemia/ small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma Splenic marginal-zone B-cell lymphoma Nodal marginal-zone lymphoma Extranodal marginal-zone B-cell lymphoma, mucosa-associated lymphoid tissue (MALT) type Hairy cell leukemia Plasma-cell myeloma/ plasmacytoma Follicular lymphoma Mantle-cell lymphoma Diffuse large B-cell lymphoma (DLBCL) Burkitt's lymphoma/Burkitt's cell leukemia Blastic NK-cell leukemia This slide presents the World Health Organization (WHO) classification for B-cell lymphomas. B-cell lymphomas are classified by stage of differentiation, whether precursor or mature (peripheral) B-cell neoplasms. Mature neoplasms are in turn classified according to morphology, location of tumor, genotype, and phenotype. Examples include: Follicular lymphomas are characterized by the growth pattern of the cells. The various marginal-zone lymphomas have characteristic phenotypic markers and present at distinct locations. Hairy cell leukemia consists of a monoclonal population that has characteristic cytoplasmic projections on the cell surface. Burkitt’s lymphoma is characterized by clonal B lymphocytes with an Ig/myc translocation in the Ig heavy chain gene. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Harris NL et al. J Clin Oncol. 1999;17:
 B-cell neoplasms. B-cell chronic lymphocytic leukemia/ small lymphocytic lymphoma. B-cell prolymphocytic leukemia. Lymphoplasmacytic lymphoma. Splenic marginal-zone B-cell lymphoma. Nodal marginal-zone lymphoma. Extranodal marginal-zone B-cell lymphoma, mucosa-associated lymphoid tissue (MALT) type. Hairy cell leukemia. Plasma-cell myeloma/ plasmacytoma. Follicular lymphoma. Mantle-cell lymphoma. Diffuse large B-cell lymphoma (DLBCL) Burkitt s lymphoma/Burkitt s cell leukemia. Blastic NK-cell leukemia. This slide presents the World Health Organization (WHO) classification for B-cell lymphomas. B-cell lymphomas are classified by stage of differentiation, whether precursor or mature (peripheral) B-cell neoplasms. Mature neoplasms are in turn classified according to morphology, location of tumor, genotype, and phenotype. Examples include: Follicular lymphomas are characterized by the growth pattern of the cells. The various marginal-zone lymphomas have characteristic phenotypic markers and present at distinct locations. Hairy cell leukemia consists of a monoclonal population that has characteristic cytoplasmic projections on the cell surface. Burkitt’s lymphoma is characterized by clonal B lymphocytes with an Ig/myc translocation in the Ig heavy chain gene. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Harris NL et al. J Clin Oncol. 1999;17:")
17
WHO Classification: T-Cell Malignancies
Precursor T-cell neoplasm Precursor T-lymphoblastic leukemia/lymphoma Mature (peripheral) T-cell neoplasms T-cell prolymphocytic leukemia T-cell granular lymphocytic leukemia Aggressive NK-cell leukemia Adult T-cell lymphoma/leukemia (HTLV1+) Extranodal NK/T-cell lymphoma, nasal type Enteropathy-type T-cell lymphoma Hepatosplenic gamma-delta T-cell lymphoma Subcutaneous panniculitis-like T-cell lymphoma Mycosis fungoides/Sézary syndrome Primary cutaneous anaplastic large cell lymphoma, T/null cell Peripheral T-cell lymphoma, unspecified Angioimmunoblastic T-cell lymphoma Primary systemic anaplastic large cell lymphoma, T/null cell Blastic NK lymphoma This slide presents the World Health Organization (WHO) classification for T-cell lymphomas. T-cell lymphomas are classified by stage of differentiation, whether precursor or mature (peripheral) T-cell neoplasms. Mature neoplasms are in turn classified according to morphology, location of tumor, genotype, and phenotype. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Harris NL et al. J Clin Oncol. 1999;17:
 T-cell neoplasms. T-cell prolymphocytic leukemia. T-cell granular lymphocytic leukemia. Aggressive NK-cell leukemia. Adult T-cell lymphoma/leukemia (HTLV1+) Extranodal NK/T-cell lymphoma, nasal type. Enteropathy-type T-cell lymphoma. Hepatosplenic gamma-delta T-cell lymphoma. Subcutaneous panniculitis-like T-cell lymphoma. Mycosis fungoides/Sézary syndrome. Primary cutaneous anaplastic large cell lymphoma, T/null cell. Peripheral T-cell lymphoma, unspecified. Angioimmunoblastic T-cell lymphoma. Primary systemic anaplastic large cell lymphoma, T/null cell. Blastic NK lymphoma. This slide presents the World Health Organization (WHO) classification for T-cell lymphomas. T-cell lymphomas are classified by stage of differentiation, whether precursor or mature (peripheral) T-cell neoplasms. Mature neoplasms are in turn classified according to morphology, location of tumor, genotype, and phenotype. Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November J Clin Oncol. 1999;17: Harris NL et al. J Clin Oncol. 1999;17:")
18
B-Cell Development Stem cell Immature B cell Follicle-center B cell
s-IgM s-IgM/G/A CD22 CD79a CD79a TdT CD21 CD10 CD22 HLA-DR CD20 HLA-DR bcl6 CD21 HLA-DR CD34 CD19 CD20 CD19 Pre-pre–B cell Immunoblast s-IgM/G/A TdT c-CD22 c-CD79a CD22 Mature B cell CD79a CD138± c-Ig s-IgM & IgD CD20 HLA-DR CD19 The successive stages of B-cell development can be identified by surface marker expression that correlates with a sequence of genetic events. All B cells arise in the bone marrow from stem cells. Lymphoid progenitor cells receive signals from bone marrow stromal cells to begin B-cell development. Differentiation from stem cell to the mature B cell occurs in the bone marrow and is antigen-independent. Differentiation from follicle-center B cell to plasma cell occurs in the germinal centers of the secondary lymphoid organs and is antigen-dependent. CD20, a marker that is a therapeutic target for certain B-cell lymphomas, is expressed in stages pre–B cell through immunoblast. The human multiple myeloma oncogene 1 (MUM1), a marker that was recently characterized and may aid in correct tumor subclassification, is expressed in the immunoblast and plasma-cell stages. CD79a CD19 HLA-DR CD22 MUM1 HLA-DR CD21 Pre–B cell CD20 CD10 TdT c-CD22 c-CD79a c-m CD19 Plasma cell CD20 CD79a CD138 CD19 c-Ig HLA-DR Precursor cells Virgin (naïve) B cells Germinal-center and post–germinal-center B cells PCA-1 MUM1
, a marker that was recently characterized and may aid in correct tumor subclassification, is expressed in the immunoblast and plasma-cell stages. CD79a. CD19. HLA-DR. CD22. MUM1. HLA-DR. CD21. Pre–B cell. CD20. CD10. TdT c-CD22 c-CD79a c-m. CD19. Plasma cell. CD20. CD79a. CD138. CD19. c-Ig. HLA-DR. Precursor cells. Virgin (naïve) B cells. Germinal-center and post–germinal-center B cells. PCA-1. MUM1.")
19
Antigen Expression in B-Cell Lineage
Pre-B Early B Mature B Plasmacytoid B Type of B cell lymphoma is a function of: Where the cell was in development/maturation when it went “bad” What molecular derangement occurred Plasma Activated B Stem cell Burkitts, FL, DLBCL WM MM MCL, CLL ALL Germinal center Individual stages of B-cell differentiation are identified by characteristic morphology and expression patterns of cell-surface antigens (CDs). CD19 is a marker of B-cell commitment, and its expression is first detected during the pre–B-cell stage.1 Changes in morphology and antigen expression during B-cell differentiation are reflected in the malignant counterparts of individual B cells. Detection of specific subsets of antigens has become an important method for identifying leukemia and lymphoma subtypes. For example, chronic lymphocytic leukemia (CLL) is a malignancy of intermediate B cells characterized by expression of CD19, CD20, CD23, and CD5 antigens.2 The malignant clone of follicular lymphoma (FL) is a more mature B cell, expressing CD19, CD20, and CD22, but not CD5. Several CD20, CD22, and CD52 monoclonal antibodies (mAbs) are currently being investigated for the treatment of B-cell malignancies. With the advent of mAb therapy, understanding of specific patterns of antigen expression will be critical for successful treatments. The hashed lines on the bars depict lower or variable expression levels. ALL = acute lymphoblastic leukemia; MCL = mantle cell lymphoma; PLL = prolymphocytic leukemia; DLBCL = diffuse large B-cell lymphoma; HCL = hairy cell leukemia; WM = Waldenström’s macroglobulinemia; MM = multiple myeloma. Jaffe. In: Non-Hodgkin’s Lymphoma. 1997:84. Jaffe. In: Non-Hodgkin’s Lymphoma. 1997:84. Ginaldi et al. J Clin Pathol. 1998;51:364.
. CD19 is a marker of B-cell commitment, and its expression is first detected during the pre–B-cell stage.1. Changes in morphology and antigen expression during B-cell differentiation are reflected in the malignant counterparts of individual B cells. Detection of specific subsets of antigens has become an important method for identifying leukemia and lymphoma subtypes. For example, chronic lymphocytic leukemia (CLL) is a malignancy of intermediate B cells characterized by expression of CD19, CD20, CD23, and CD5 antigens.2 The malignant clone of follicular lymphoma (FL) is a more mature B cell, expressing CD19, CD20, and CD22, but not CD5. Several CD20, CD22, and CD52 monoclonal antibodies (mAbs) are currently being investigated for the treatment of B-cell malignancies. With the advent of mAb therapy, understanding of specific patterns of antigen expression will be critical for successful treatments. The hashed lines on the bars depict lower or variable expression levels. ALL = acute lymphoblastic leukemia; MCL = mantle cell lymphoma; PLL = prolymphocytic leukemia; DLBCL = diffuse large B-cell lymphoma; HCL = hairy cell leukemia; WM = Waldenström’s macroglobulinemia; MM = multiple myeloma. Jaffe. In: Non-Hodgkin’s Lymphoma. 1997:84. Jaffe. In: Non-Hodgkin’s Lymphoma. 1997:84. Ginaldi et al. J Clin Pathol. 1998;51:364.")
20
Models of Chromosomal Translocations in NHL
REG REG REG REG CODING CODING CODING CODING Proto-oncogene Proto-oncogene TRANSLOCATION TRANSLOCATION REG REG All NHL translocations that have been cloned to date have a proto-oncogene in the vicinity of 1 of 2 chromosomal recombination sites. As shown on the left side of this slide, chromosomal translocations in mature B- and T-cell malignancies juxtapose the proto-oncogene to heterologous regulatory sequences derived from the partner chromosome, resulting in deregulated expression of the proto-oncogene. The 2 exceptions to the deregulation model are translocation t(2;5) of T-cell anaplastic large-cell lymphoma (ALCL) and translocation t(11;18) of mucosa-associated lymphoid tissue (MALT) type lymphoma, both of which result in gene fusions coding for chimeric proteins, as shown on the right side of this slide. Harris NL, Stein H, Coupland SE, et al. New approaches to lymphoma diagnosis. Hematology (Am Soc Hematol Educ Program). 2001: CODING COD ING TRANSCRIPTIONAL DEREGULATION FUSION PROTEIN REG = regulatory sequence. Harris NL et al. Hematology (Am Soc Hematol Educ Program). 2001:
 of T-cell anaplastic large-cell lymphoma (ALCL) and translocation t(11;18) of mucosa-associated lymphoid tissue (MALT) type lymphoma, both of which result in gene fusions coding for chimeric proteins, as shown on the right side of this slide. Harris NL, Stein H, Coupland SE, et al. New approaches to lymphoma diagnosis. Hematology (Am Soc Hematol Educ Program). 2001: CODING. COD. ING. TRANSCRIPTIONAL DEREGULATION. FUSION PROTEIN. REG = regulatory sequence. Harris NL et al. Hematology (Am Soc Hematol Educ Program). 2001:")
21
Chromosomal Translocations Commonly Associated With Activation in B-Cell Malignancies
Oncogene Protein Translocation Disease bcl-1 Cyclin D1 t(11;14) MCL bcl-2 BCL2 (antiapoptosis) t(14;18) FL myc Transcription factor t(8;14) Burkitt’s NHL bcl-6 Zinc-finger transcription factor t(3;14) DLBCL (some follicular NHL) Chromosomal translocations are commonly associated with activation or worse prognosis in B-cell malignancies. The table reviews some of the more common translocations associated with different B-cell malignancy histologies and the relationship of the translocation to the corresponding oncogene. MCL frequently has chromosomal translocation t(11;14)(q13;q32). This juxtaposes the bcl1 locus with the IgG locus. Such an alteration results in deregulation of the bcl1 locus and expression of its gene product cyclin D1 which is not normally expressed in B cells. Activation of bcl1 appears to be critical in the pathogenesis of MCL. Cyclin D1 is important in cell cycle control, and bcl1 is considered a proto-oncogene. A translocation of t(14;18) (q32;q21) is present in approximately 85% of cases FL and 15%-20% of DLBCL cases. This change results in rearrangement of the bcl2 gene, leading to activated forms of NHL. Some translocations are very frequently and highly associated with a particular histology and prognosis; in DLBCL, which is an aggressive heterogeneous lymphoma, there are several different translocations observed, each with a different prognosis. Examples include: 30% of cases have t(14;18) with bcl2 overexpression, 35% have 3q27 rearrangements with bcl6 overexpression, and rare cases have t(8;14) with c-myc overexpression. National Comprehensive Cancer Network. Practice Guidelines in Oncology. v National Comprehensive Cancer Network, Inc. Practice Guidelines in Oncology. v Skarin and Dorfman. CA Cancer J Clin. 1997;47:351. Jennings and Foon. Blood. 1997;90:2863.
 MCL. bcl-2. BCL2 (antiapoptosis) t(14;18) FL. myc. Transcription factor. t(8;14) Burkitt’s NHL. bcl-6. Zinc-finger transcription factor. t(3;14) DLBCL (some follicular NHL) Chromosomal translocations are commonly associated with activation or worse prognosis in B-cell malignancies. The table reviews some of the more common translocations associated with different B-cell malignancy histologies and the relationship of the translocation to the corresponding oncogene. MCL frequently has chromosomal translocation t(11;14)(q13;q32). This juxtaposes the bcl1 locus with the IgG locus. Such an alteration results in deregulation of the bcl1 locus and expression of its gene product cyclin D1 which is not normally expressed in B cells. Activation of bcl1 appears to be critical in the pathogenesis of MCL. Cyclin D1 is important in cell cycle control, and bcl1 is considered a proto-oncogene. A translocation of t(14;18) (q32;q21) is present in approximately 85% of cases FL and 15%-20% of DLBCL cases. This change results in rearrangement of the bcl2 gene, leading to activated forms of NHL. Some translocations are very frequently and highly associated with a particular histology and prognosis; in DLBCL, which is an aggressive heterogeneous lymphoma, there are several different translocations observed, each with a different prognosis. Examples include: 30% of cases have t(14;18) with bcl2 overexpression, 35% have 3q27 rearrangements with bcl6 overexpression, and rare cases have t(8;14) with c-myc overexpression. National Comprehensive Cancer Network. Practice Guidelines in Oncology. v National Comprehensive Cancer Network, Inc. Practice Guidelines in Oncology. v Skarin and Dorfman. CA Cancer J Clin. 1997;47:351. Jennings and Foon. Blood. 1997;90:2863.")
22
Lymphoma Biology Aggressive NHL Indolent NHL
short natural history (patients die within months if untreated) disease of rapid cellular proliferation Potentially curable with chemotherapy Indolent NHL long natural history (patients can live for many years untreated) disease of slow cellular accumulation Generally incurable with chemotherapy
 disease of rapid cellular proliferation. Potentially curable with chemotherapy. Indolent NHL. long natural history (patients can live for many years untreated) disease of slow cellular accumulation. Generally incurable with chemotherapy.")
23
NHL: Presentation and Staging
Aggressive NHL Patients likely to present with symptoms Indolent NHL Patients likely to present with painless adenopathy Initial workup similar to Hodgkin Lymphoma

24
NHL: Approach to the Patient
Approach dictated mainly by histology reliable hematopathology crucial Aggressive NHL Cure is often the goal Indolent NHL Cure is rarely the goal Control is the goal

25
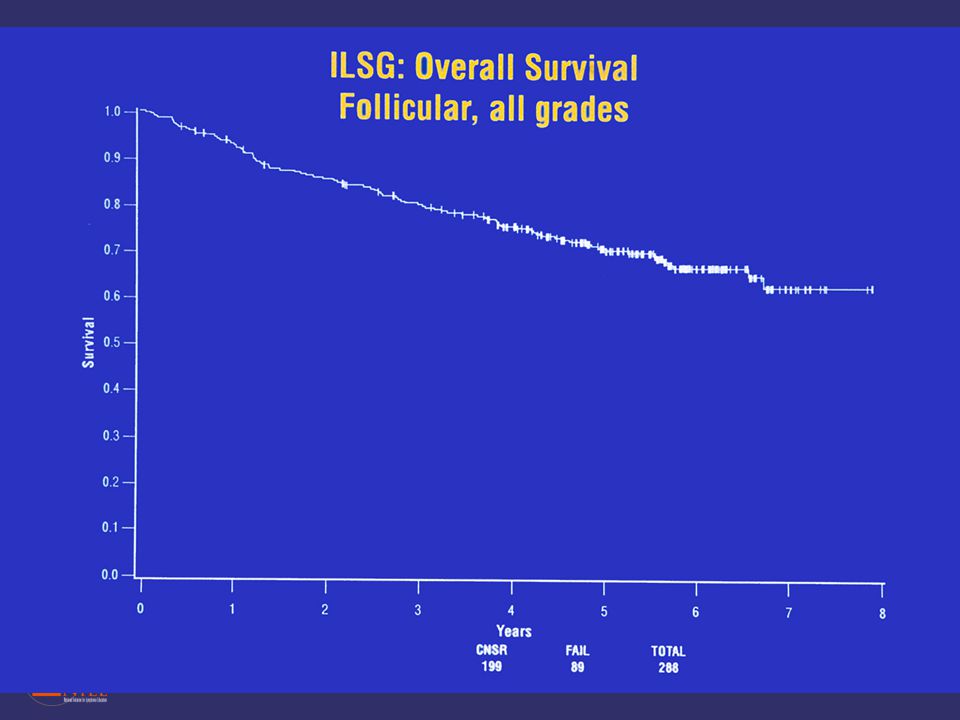
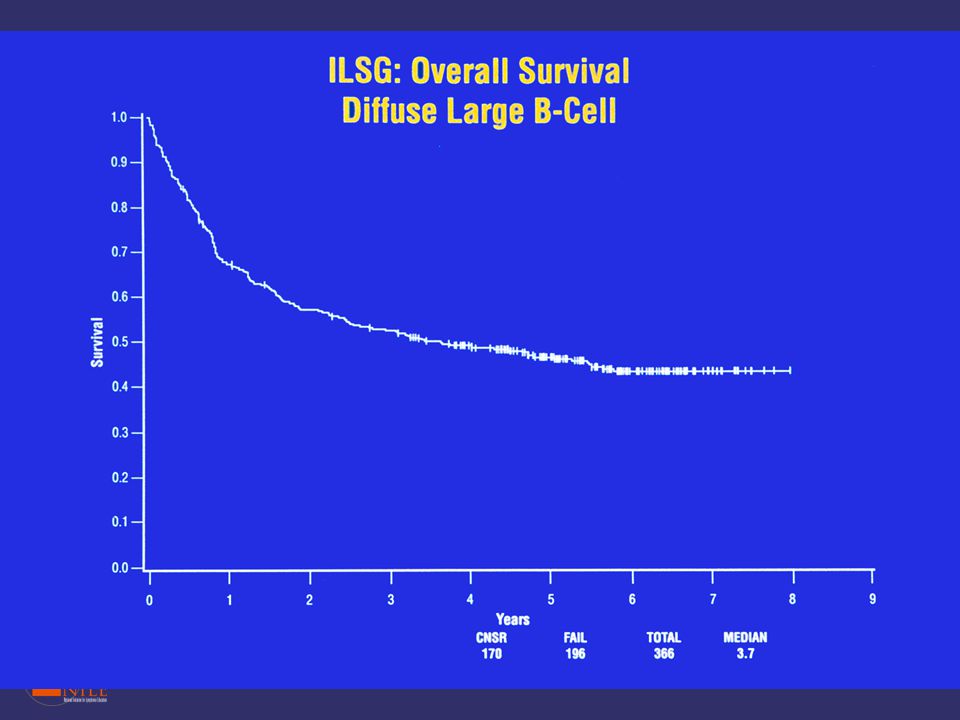
Most Common NHLs Category Frequency (%) Diffuse large B-cell 31
Follicular 22 Marginal-zone B-cell, MALT 8 Peripheral T-cell 7 Small B-lymphocytic/CLL Mantle-cell lymphoma 6 Primary mediastinal large B-cell 2 Anaplastic large T/null cell High-grade B-cell, Burkitt-like Marginal-zone B-cell, nodal Precursor T-lymphoblastic lymphoma The vast majority (85%-90%) of lymphomas encountered by clinicians in the United States are of B-cell origin. Based on the World Health Organization (WHO) classification, the 2 most common NHLs are diffuse large B-cell lymphoma, occurring in 31% of patients, and follicular lymphoma, occurring in 22% patients. The 11 most frequent lymphomas, shown in this table, occur in more than 2% of patients. All the remaining categories occur at a frequency of less than 1%. Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin's lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin’s Lymphoma Classification Project. J Clin Oncol. 1998;16: Armitage JO, Weisenburger DD. J Clin Oncol. 1998;16:
 of lymphomas encountered by clinicians in the United States are of B-cell origin. Based on the World Health Organization (WHO) classification, the 2 most common NHLs are diffuse large B-cell lymphoma, occurring in 31% of patients, and follicular lymphoma, occurring in 22% patients. The 11 most frequent lymphomas, shown in this table, occur in more than 2% of patients. All the remaining categories occur at a frequency of less than 1%. Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin s lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin’s Lymphoma Classification Project. J Clin Oncol. 1998;16: Armitage JO, Weisenburger DD. J Clin Oncol. 1998;16:")
26
Follicular Lymphoma

27
Approach to Indolent NHL
Indolent NHL: guiding treatment principle immediate treatment does not prolong overall survival for many patients When to treat? constitutional symptoms compromise of a vital organ by compression or infiltration, particularly the bone marrow bulky adenopathy rapid progression evidence of transformation Will often begin with relatively non-toxic treatments and escalate the intensity of the therapy

29
Diffuse Large B Cell Lymphoma

30
Approach to Aggressive NHL
Patients have the potential to be cured Administer most effective therapy (no matter how harsh) at diagnosis If not cured, patients typically die within a few years of diagnosis
 at diagnosis. If not cured, patients typically die within a few years of diagnosis.")
32
International Prognostic Index for Age-Adjusted
Risk Group Number of Factors Present 5-year DFS Age≤60 (%) 5-year OS Age≤60 Low 86 83 Low-Intermediate 1 66 69 High-Intermediate 2 53 46 High 3 58 32 Factor Adverse PS ≥2 LDH >Normal Stage III-IV The analysis for 1,274 patients 60 years is shown here. The overall survival rates were somewhat lower when assessed for the entire population without regard to age. The International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med. 1993;329: The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med. 1993;329:
 5-year OS Age≤60. Low Low-Intermediate High-Intermediate High Factor. Adverse. PS. ≥2. LDH. >Normal. Stage. III-IV. The analysis for 1,274 patients 60 years is shown here. The overall survival rates were somewhat lower when assessed for the entire population without regard to age. The International Non-Hodgkin s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin s lymphoma. N Engl J Med. 1993;329: The International Non-Hodgkin s Lymphoma Prognostic Factors Project. N Engl J Med. 1993;329:")
33
DLBCL: Subtypes Revealed by Expression Array
1.0 Germinal-center B-cell–like 0.8 0.6 Probability Activated B-cell–like 0.4 0.2 P = 7.9 E-6 0.0 2 4 6 8 10 Some cases of diffuse large B-cell lymphoma (DLBCL) respond well to multi-agent chemotherapy and have prolonged survival; however, about 60% of cases are incurable. This clinical heterogeneity may be due to the existence of multiple unidentified tumor subtypes. The use of gene-expression array analysis identifies 2 molecularly distinct forms of DLBCL which had gene-expression patterns indicative of different stages of B-cell differentiation. The center panel on the slide compares expression patterns. The gene array on the left shows the hierarchical clustering of genes selectively expressed in different tumor samples. For comparison, the gene array on the right shows expression profiles of normal B-cell types at different stages of activation. Patients with germinal-center B-cell–like DLBCL had a significantly better overall survival than those with activated B-cell–like DLBCL (see survival curve). Alizadeh AA, Eisen MB, Davis RE et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403: Overall survival (years) Single histology with multiple molecular subtypes …with different outcomes Alizadeh AA et al. Nature. 2000;403:
 respond well to multi-agent chemotherapy and have prolonged survival; however, about 60% of cases are incurable. This clinical heterogeneity may be due to the existence of multiple unidentified tumor subtypes. The use of gene-expression array analysis identifies 2 molecularly distinct forms of DLBCL which had gene-expression patterns indicative of different stages of B-cell differentiation. The center panel on the slide compares expression patterns. The gene array on the left shows the hierarchical clustering of genes selectively expressed in different tumor samples. For comparison, the gene array on the right shows expression profiles of normal B-cell types at different stages of activation. Patients with germinal-center B-cell–like DLBCL had a significantly better overall survival than those with activated B-cell–like DLBCL (see survival curve). Alizadeh AA, Eisen MB, Davis RE et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403: Overall survival (years) Single histology with. multiple molecular. subtypes. …with different outcomes. Alizadeh AA et al. Nature. 2000;403:")
34
Summary NHL incidence increasing
Hodgkin incidence stable or decreasing Hodgkin Lymphoma Characterized by the Reed-Sternberg Cells Stage more important that histologic subtype Often limited stage (stage I or II) Spreads to contiguous nodes Often affects younger patients Very responsive to therapy Cure rate quite high
 Spreads to contiguous nodes. Often affects younger patients. Very responsive to therapy. Cure rate quite high.")
35
Summary NHL cure rate mediocre Many histologic subtypes
Often more important that the stage indolent vs. aggressive Function of underlying biology indolent: Often asymptomatic Treatment: Less is more aggressive: Often symptomatic require aggressive treatment ASAP to achieve cure

Similar presentations



>")













>")

