Download presentation
Presentation is loading. Please wait.

1
S. Alex Stalcup, M.D. New Leaf Treatment Center 251 Lafayette Circle, Suite 150 Lafayette, CA 94549 Tel: 925-284-5200 Fax: 925-284-5204 alex@nltc.comwww.nltc.com

2
Addiction is a Pediatric Disease 80% of addicts have risk factors known in childhood Family history of addiction ADHD (attention deficit hyperactivity disorder) Mood disorder (depression, anxiety, trauma) School failure 80% of adult drinkers try alcohol before age 18. Of children who begin drinking before age 14, 47% will become alcoholics. Average age of initiation to marijuana use is age 15.

3
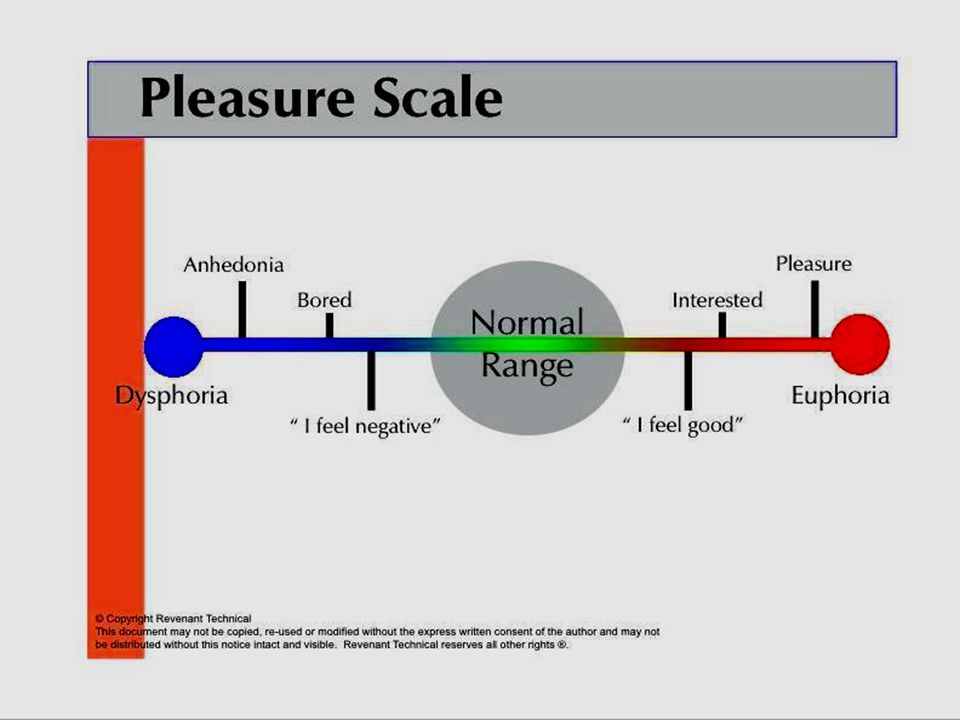
What is a Drug? A drug is a pleasure producing chemical. Drugs activate or imitate chemical pathways in the brain associated with feelings of well-being, pleasure and euphoria.

5
Neuroadaptation, Tolerance, and Withdrawal Neuroadaptation is the brain’s response to over stimulation from drugs. Drug-specific circuits cause a mixture of sedation and stimulation or intoxication. Tolerance is the process by which the reward and pleasure centers of the brain adapt to high concentrations of pleasure neurotransmitters. In direct response to overstimulation, the brain regions decrease in sensitivity and become unresponsive (deaf) to normal levels of stimulation. In addition to pleasure circuits each drug type affects other specific circuits. Other brain pathways overstimulated by drugs also neuroadapt and become under active, directly leading to anxiety, depression, and loss of energy. Once neuroadaptation develops (tolerance), there will always be withdrawal symptoms that are the mirror image of the drug effects. Cessation of drug use leads to ‘inversion of the high’; sobriety becomes pleasureless, anxious, sleepless, and lacking energy Under unstimulated conditions (without drugs) there is profound interference with the ability to experience normal pleasure. When sober, the user feels anhedonia, anxiety, anger, frustration and craving. The pleasure system remains impaired for months to years, interfering with sobriety, learning, and impulse inhibition.
 to normal levels of stimulation. In addition to pleasure circuits each drug type affects other specific circuits. Other brain pathways overstimulated by drugs also neuroadapt and become under active, directly leading to anxiety, depression, and loss of energy. Once neuroadaptation develops (tolerance), there will always be withdrawal symptoms that are the mirror image of the drug effects. Cessation of drug use leads to ‘inversion of the high’; sobriety becomes pleasureless, anxious, sleepless, and lacking energy Under unstimulated conditions (without drugs) there is profound interference with the ability to experience normal pleasure. When sober, the user feels anhedonia, anxiety, anger, frustration and craving. The pleasure system remains impaired for months to years, interfering with sobriety, learning, and impulse inhibition..")
6
Compulsion: loss of control The user can’t not do it s/he is compelled to use. Compulsion is not rational and is not planned. Continued use despite adverse consequences An addict is a person who uses even though s/he knows it is causing problems. Addiction is staged based on adverse consequences. Craving: daily symptom of the disease The user experiences intense psychological preoccupation with getting and using the drug. Craving is dysphoric, agitating and it feels very bad. Denial/hypofrontality: distortion of cognition caused by craving Under the pressure of intense craving, the user is temporarily blinded to the risks and consequences of using. Definition of Addiction

7
Abuse versus Addiction Substance Abuse is distinguished from Addiction by the appearance of tolerance and withdrawal, leading to loss of control over use. Substance abusers require motivation to stop. Addicts require treatment to stop.

8
AssessmentAssessment Emergency Room Domestic Violence Family Court Family Court Probation - Parole Schools Schools Psych Emergency Entrance into SystemArrestArrest

9
EntryAssessment Monitoring Random UDS 6 tests/90 days ? Unsure Addict Intensive Outpatient IOP Discharge Residential Treatment In-custody Treatment IOP + Sober Living Re-entry Monitoring Random UDS 6 months (Positive UDS) Monitoring and Treatment Discharge
 Monitoring and Treatment Discharge.")
12
National Survey on Drug Use and Health Statistics 2007

13
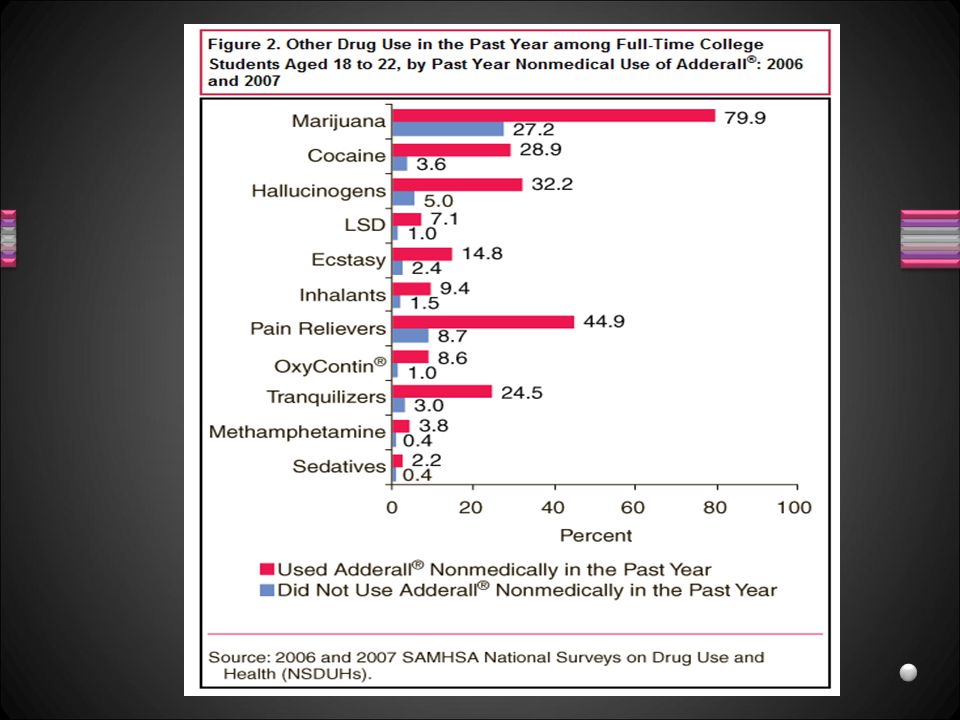
Prescription Drug Abuse Opiate pain medications Benzodiazepine tranquilizers Prescription stimulants (Adderall, Ritalin) Sleeping pills, muscle relaxants
 Sleeping pills, muscle relaxants")
14
Sentinel Events in Prescription Drug Abuse Overdoses in younger individuals DUI arrests with low BAL Youth falling asleep in school Youth stealing from parents and friends Increased schoolyard drug and pill sales

15
National Survey on Drug Use and Health Statistics 2007

18
“You’ve Got Drugs V” Prescription Drug Pushers on the Internet. National Center on Addiction and Substance Abuse, Columbia University 2008

20
Prescription Opiates Generic: Brand NameNon Tolerant 24 hr. dose Codeine w/acetaminophen500 mg Hydrocodone:Vicodin, Lortab, Norco20mg-60 mg Hydromorphone: Dilaudid20 mg-60 mg Oxycodone: Percodan, OxyContin20 mg-60 mg Morphine sulfate: MS Contin30 mg-60 mg Fentanyl: Duragesic (transdermal), Actiq25 mcg-50 mcg Tolerant Users onlyTolerant 24 hr. dose Morphine sulfate: MS Contin60 mg-upward Fentanyl: Duragesic (transdermal)75 mcg-300 mcg Methadone: Methadose60 mg-300 mg Buprenorphine: Suboxone, Subutex 6 mg-32 mg
, Actiq25 mcg-50 mcg Tolerant Users onlyTolerant 24 hr. dose Morphine sulfate: MS Contin60 mg-upward Fentanyl: Duragesic (transdermal)75 mcg-300 mcg Methadone: Methadose60 mg-300 mg Buprenorphine: Suboxone, Subutex 6 mg-32 mg.")
21
Opiate progression from pills to the needle Historically, untreated dependence on prescription opiates led to a trajectory from Pills ingested orally Pills crushed and snorted or smoked Heroin snorted or smoked Heroin used intravenously

22
A 33-year follow-up of narcotics addicts.

23
Overview of Buprenorphine: Suboxone and Subutex Highly safe medication (acute & chronic dosing). Primary side effects: like other mu agonist opioids (e.g.,nausea, constipation) but may be less severe. No evidence of significant disruption in cognitive or psychomotor performance with buprenorphine maintenance. No evidence of organ damage with chronic dosing. Use of Buprenorphine in the Pharmacologic Management of Opioid Dependence: A Curriculum of Physicians. (eds: Strain EC, Trhumble JG, Jara GB) CSAT. 2001
 but may be less severe. No evidence of significant disruption in cognitive or psychomotor performance with buprenorphine maintenance. No evidence of organ damage with chronic dosing. Use of Buprenorphine in the Pharmacologic Management of Opioid Dependence: A Curriculum of Physicians. (eds: Strain EC, Trhumble JG, Jara GB) CSAT")
24
Prescription Tranquillizers Dose Equivalent To Alcohol (2oz liquor or 2 glasses of wine or 2 cans of beer) Alprazolam (Xanax®)0.5- 1mg Diazepam (Valium®)10mg Chlordiazepoxide (Librium®)25mg Clonazepam (Klonopin®)1-2mg Lorazepam (Ativan®)2mg Temazepam (Restoril®)30mg Butalbital (in Fiorinal®)100mg Carisoprodol (Soma ®)350mg Zolpidem (Ambien®) 10 mg
 Alprazolam (Xanax®)0.5- 1mg Diazepam (Valium®)10mg Chlordiazepoxide (Librium®)25mg Clonazepam (Klonopin®)1-2mg Lorazepam (Ativan®)2mg Temazepam (Restoril®)30mg Butalbital (in Fiorinal®)100mg Carisoprodol (Soma ®)350mg Zolpidem (Ambien®) 10 mg")
25
Sedative-Hypnotic Effects Effects Calm Euphoria Release of Inhibitions Sleep Inducing Sedation/Sleepiness Slurred Speech Unsteady gait (Ataxia) Confusion Forgetfulness Slows heart rate Decreases blood pressure * Symptom may continue for months Withdrawal Dysphoria * Anxiety * Insomnia * Sweating (Diaphoresis) * Tremor Tachycardia Hypertension Hyperventilation Elevated temperature Hallucinations Seizures Delirium tremens
 Confusion Forgetfulness Slows heart rate Decreases blood pressure * Symptom may continue for months Withdrawal Dysphoria * Anxiety * Insomnia * Sweating (Diaphoresis) * Tremor Tachycardia Hypertension Hyperventilation Elevated temperature Hallucinations Seizures Delirium tremens")
26
Prescription Stimulants Adderall is a brand-name pharmaceutical psychostimulant composed of mixed amphetamine salts. Adderall is widely reported to increase alertness, concentration and overall cognitive performance while decreasing user fatigue. Prescription Stimulants are Schedule II drugs under the Controlled Substance Act for the United States. Concerta, Vyvanse, Dexedrine are similar, often abused, prescription psycho-stimulants.

27
Medications for Stimulant Dependence Antidepressants (anhedonia/anergia) Effexor XR150-300 mg Cymbalta60 mg Wellbutrin XL150-300 mg Desipramine100-200 mg Anti-Craving Medications Modafinil100-200 mg Methylphenidate LA 10-40 mg Buproprion150-300 mg Concerta18-54 mg Dexedrine SR20-30 mg Disorders of Sleep Trazedone50-300 mg Seroquel25-100 mg Imipramine100-200 mg Disorders of Thought Abilify2-10 mg Haldol1-2 mg Risperdal1-3 mg
 Effexor XR mg Cymbalta60 mg Wellbutrin XL mg Desipramine mg Anti-Craving Medications Modafinil mg Methylphenidate LA mg Buproprion mg Concerta18-54 mg Dexedrine SR20-30 mg Disorders of Sleep Trazedone mg Seroquel mg Imipramine mg Disorders of Thought Abilify2-10 mg Haldol1-2 mg Risperdal1-3 mg")
28
Are you at Risk? B P S M The Bio-Psycho-Social Model E W M S Environment Withdrawal Mental Health Stress

29
Bio-Psycho-Social Model Predisposition Genetics Childhood Sexual Abuse Mental Illness Acquired Hypofrontality in utero alcohol/drug exposurelow birth weight perinatal asphyxiahead injury The Drug / Circumstances of First Use Enabling System

30
C I M Model Treatment Causes of Craving EWMS Environmental cues (Triggers ) immediate, catastrophic, overwhelming craving stimulated by people, places, things associated with prior drug-use experiences Drug Withdrawal inadequately treated or untreated Mental illness symptoms inadequately treated or untreated Stress equals craving
 immediate, catastrophic, overwhelming craving stimulated by people, places, things associated with prior drug-use experiences Drug Withdrawal inadequately treated or untreated Mental illness symptoms inadequately treated or untreated Stress equals craving")
31
Environmental Cueing = Conditioned Craving Drug pleasure becomes associated with specific people, places, and things; to encounter any of those things in the environment is to trigger craving for the drug. Such triggers persist for decades after use.

32
Bio-Psycho-Social Model Are you at Risk? Apply B P S M (bio-psycho-social model) to yourself: Family history of addiction? Do you have a tendency to boredom or ADHD? Are you anxious or depressed? Have you suffered sexual trauma? Do you use substances to reduce stress? Did drug and alcohol use enter your life at a difficult time? Are you surrounded by drug and alcohol users?
 to yourself: Family history of addiction. Do you have a tendency to boredom or ADHD. Are you anxious or depressed. Have you suffered sexual trauma. Do you use substances to reduce stress. Did drug and alcohol use enter your life at a difficult time. Are you surrounded by drug and alcohol users .")
33
Bio-Psycho-Social Model Are you in trouble? How can you tell if you are getting into trouble? Are you using more frequently and using greater amounts? Have you developed tolerance? Is your use causing adverse consequences: grades, friends, money, health, unwanted sexual behavior? Do you crave the drug under addiction conditions: Environment, Withdrawal, Mental Health, Stress (EWMS) If so, when you crave the drug, can you talk yourself into using it, even when you have resolved to not use? When you have resolved not to use, under known craving conditions, do you find yourself using: environmental cues, anxiety or blue, withdrawal (bored, irritable, sleep), or when you are stressed?
 If so, when you crave the drug, can you talk yourself into using it, even when you have resolved to not use. When you have resolved not to use, under known craving conditions, do you find yourself using: environmental cues, anxiety or blue, withdrawal (bored, irritable, sleep), or when you are stressed .")
34
Bio-Psycho-Social Model Are You an Addict? TRY THE “EXPERIMENT” Resolve not to use for 5 weeks. Go about your usual daily activities. Put yourself around the drug and people using it.

35
Bio-Psycho-Social Model Are You an Addict? AFTER 5 WEEKS Were you able to not use? Did you find your mind talking you into using? Did you struggle not to use? Were you able to have pleasure without using? Did you have problems with boredom, depression or anxiety?

36
Bio-Psycho-Social Model What to do Get out of the using environment. Find alternative sources of pleasure. Work on balancing stress. Seek help for mental health issues and other personal stresses.

37
Addiction: Risk & Resilience Inherited predisposition (genetics) Childhood trauma or abuse Unwanted sexual involvement before age 13 Mental Illness: depression, anxiety, personality disorder Attention Deficit Disorder (ADD) Learning disabilities/school failure Subjected to teasing, bullying Acne and/or obesity Other than heterosexual orientation Social rejection Early sexual involvement Onset of drug use before age 16 Enabling environment Ignorance No family history of addiction Good mental health Academic competence Positive relationship with an adult Family eats dinner together 5 days/wk Peer group participation (clubs) Participation in sports Participation in music, drama or dance Involvement in faith-based activities Taking care of pets Volunteer activities Social acceptance Environment disapproves of drug use Immediate, appropriate scaled consequences for alcohol/drug use. Early intervention for alcohol/drug use

38
REFERENCES 1. --- Responsibility and choice in addiction. Psychiatric Services. 53(6):707- 13 (2002). 2. Bechara A. Decision making, impulse control and loss of willpower to resit drugs: a neurocognitive perspective. Nature Neuroscience. 8:1458-63 (2005) 3. Dackis C, O’Brien C. Neurobiology of addiction: treatment and public policy ramifications. Nature Neuroscience. 8(11):1431-6 (2005). 4. Nestler EJ, Malenka RC. The addicted brain. Scientific American.com February 9, 2004. 5. Stalcup SA, Christian D, Stalcup JA, Brown M Galloway GP. A treatment model for craving identification and management. Journal of Psychoactive Drugs. 38:235-44, 2006 6. Volkow ND, Fowler JS, Wang GJ. The addicted human brain: insights from imaging studies. The Journal of Clinical Investigation. 111(10:1444- 51 (2003). 7. Weinberger DR, Elvevag B, Giedd JN. The adolescent brain: a work in progress. National Campaign to Prevent Teen Pregnancy. June 2005.
: (2002). 2. Bechara A. Decision making, impulse control and loss of willpower to resit drugs: a neurocognitive perspective. Nature Neuroscience. 8: (2005) 3. Dackis C, O’Brien C. Neurobiology of addiction: treatment and public policy ramifications. Nature Neuroscience. 8(11): (2005). 4. Nestler EJ, Malenka RC. The addicted brain. Scientific American.com February 9, Stalcup SA, Christian D, Stalcup JA, Brown M Galloway GP. A treatment model for craving identification and management. Journal of Psychoactive Drugs. 38:235-44, Volkow ND, Fowler JS, Wang GJ. The addicted human brain: insights from imaging studies. The Journal of Clinical Investigation. 111(10: (2003). 7. Weinberger DR, Elvevag B, Giedd JN. The adolescent brain: a work in progress. National Campaign to Prevent Teen Pregnancy. June")
Similar presentations