Download presentation
Presentation is loading. Please wait.

1
Associate Prof. Dr. Meltem Ergun
Dysphagia Associate Prof. Dr. Meltem Ergun Yeditepe University Department of Gastroenterology

2
Learning Objectives What is dysphagia? What are types of dysphagia?
What are the causes of dysphagia? How to investigate a patient with dysphagia? How is dysphagia treated?

3
Difficulty in swallowing=dysphagia
Dysphagia suggests the presence of an organic abnormality in the passage of solids or liquids from the oral cavity to the stomach. Patients' complaints range from the inability to initiate a swallow to the sensation of solids or liquids being hindered during their passage through the esophagus into the stomach.

4
Dysphagia is an alarm symptom that warrants immediate evaluation to define the exact cause and initiate appropriate therapy. Dysphagia in older adult subjects should not be attributed to normal aging. Aging alone causes mild esophageal motility abnormalities, which are rarely symptomatic

5
The Normal Swallow Innate ability which is present in the developing fetus Necessary to maintain nutrition and hydration Adults swallow approximately 580 times daily unconsciously Swallowing is a four-phase process: Oral preparatory phase Oral phase Pharyngeal phase Esophageal phase

6
Oral Preparatory Phase
Begins as food or liquid enters the mouth Containing, manipulating, and preparing the food or liquid into a bolus Chewing (mastication) occurs to grind solid bolus into manageable texture Requires coordination of lips, tongue, teeth, mandible, and cheeks Duration: variable depending on substance Respiration: normal through the nose (mouth closed)
 occurs to grind solid bolus into manageable texture. Requires coordination of lips, tongue, teeth, mandible, and cheeks. Duration: variable depending on substance. Respiration: normal through the nose (mouth closed)")
7
Oral Phase Bolus is propelled to the back of the mouth
“stripping action” by the tongue Tension in the cheeks (buccal muscles) Duration: seconds Respiration: normal through the nose
 Duration: seconds. Respiration: normal through the nose.")
8
Pharyngeal Phase Begins as the bolus reaches the tonsils (faucial pillars) Pharygeal swallow reflex is triggered: Pharyngeal wall and back of tongue move together and pharyngeal muscles squeeze to move bolus down through the pharynx Upper esophageal sphincter opens to allow passage of bolus into esophagus Time: 1 second Respiration: briefly halted (apneic moment) During bolus transit, risk of food or liquid entering the airway
 During bolus transit, risk of food or liquid entering the airway.")
9
Pharyngeal Phase – Protective Mechanisms
Soft palate elevates to stop bolus from flowing upward into nasal area Larynx moves forward and higher in the neck to reduce risk of entrance into airway Epiglottis forms a cover over the larynx Vocal folds come together to close the entrance into the larynx If material does enter the larynx, reflexive cough to expel it will occur

10
Esophageal Phase Bolus is propelled through the esophagus by an involuntary wave or contraction Moves from the upper esophageal sphincter through the lower esophageal sphincter and into the stomach Time: 8-20 seconds, can be influenced by age (often increase in duration in elderly population) Respiration: normal through nose and mouth
 Respiration: normal through nose and mouth.")
11
Disordered Swallow: Dysphagia
Impairment can occur in one, some, or all of the four phases of swallowing Some persons have impairments that result in aspiration (food or liquid moves below the level of vocal folds into the airway) Some persons have to alter their diet to control the consistencies, but this can cause difficulty maintaining hydration and nutrition Some persons require an enteral feeding tube for nutritional maintenance
 Some persons have to alter their diet to control the consistencies, but this can cause difficulty maintaining hydration and nutrition. Some persons require an enteral feeding tube for nutritional maintenance.")
12
CLASSIFICATION Two distinct syndromes
Oropharyngeal dysphagia Esophageal dysphagia Produced by abnormalities affecting the finely tuned neuromuscular mechanism of the striated muscle of the mouth, pharynx, and UES Caused by the variety of disorders affecting the smooth muscle esophagus

13
Oropharyngeal dysphagia
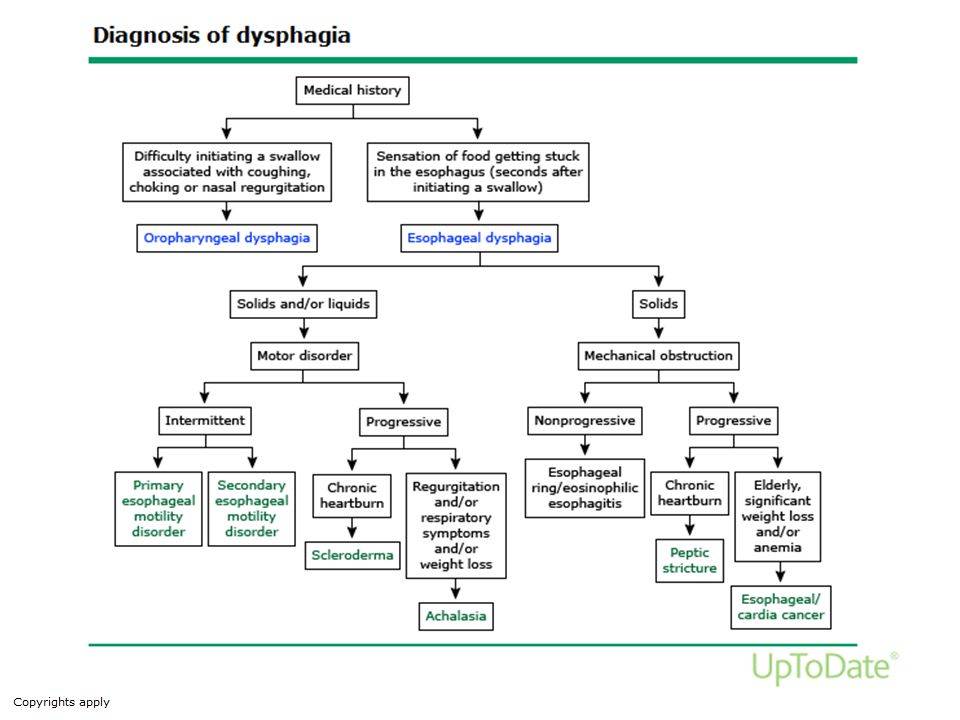
Oropharyngeal dysphagia is characterized by difficulty initiating a swallow. Swallowing may be accompanied by coughing, choking, nasopharyngeal regurgitation, aspiration, and a sensation of residual food remaining in the pharynx. It is a transfer problem caused by impaired ability to transfer food from mouth to upper esophagus impaired oral preparatory phase Clinical presentation: food sticking in the throat difficulty initiating a swallow nasal regurgitation coughing during swallowing They may also complain of dysarthria nasal speech because of associated muscle weaknesses Other Neurological clinical findings

14
Oropharyngeal Dysphagia
Neuromuscular CVA Parkinson’s disease MS Mysthania gravis Muscular dystrophy Bulbar / pseudobulbar palsy

15
Abnormalities Causing Oropharyngeal Dysphagia
Local Structural Lesions Inflammatory Pharyngitis Abscess Tuberculosis Syphilis Neoplastic Congenital webs Plummer-Vinson syndrome Extrinsic compression Thyromegaly cervical spine hyperostosis Lymphadenopathy Surgical resection of the oropharynx

16
Case Study 1 45-year old man diagnosed with ALS 18 months ago
Unable to work, on a puree diet with thin liquids, has lost 10 kg in past two months, just recovered from severe aspiration pneumonia Severe oral and pharyngeal dysphagia with aspiration What should be the treatment?

17
Case Study 2 35- year-old woman presented with dysphagia
Lab: Hb 8,6 Fe: TIBC: Ferritin:

18
Plummer Vinson sd.

19
Diffuse oesophageal spasm
Esophageal Dysphagia Motility disorders Achalasia Diffuse oesophageal spasm Chaga’s disease

20
Etiology Of Esophageal Dysphagia
Neuromuscular (Motility) Disorders Most common Achalasia Scleroderma Diffuse esophageal spasm Other associated motility abnormalities Nutcracker esophagus Hypertensive lower esophageal sphincter Vigorous achalasia Nonspecific esophageal dysmotility Other secondary motility disorders Other collagen disorders Chagas disease
 Disorders. Most common. Achalasia. Scleroderma. Diffuse esophageal spasm. Other associated motility abnormalities. Nutcracker esophagus. Hypertensive lower esophageal sphincter. Vigorous achalasia. Nonspecific esophageal dysmotility. Other secondary motility disorders. Other collagen disorders. Chagas disease.")
21
Etiology Of Esophageal Dysphagia
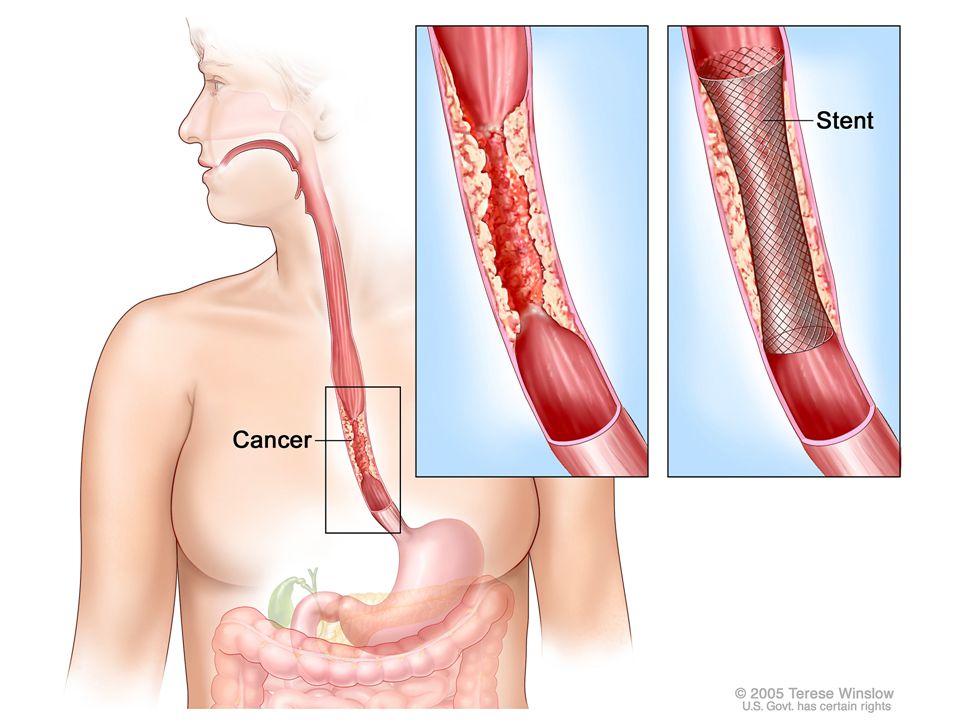
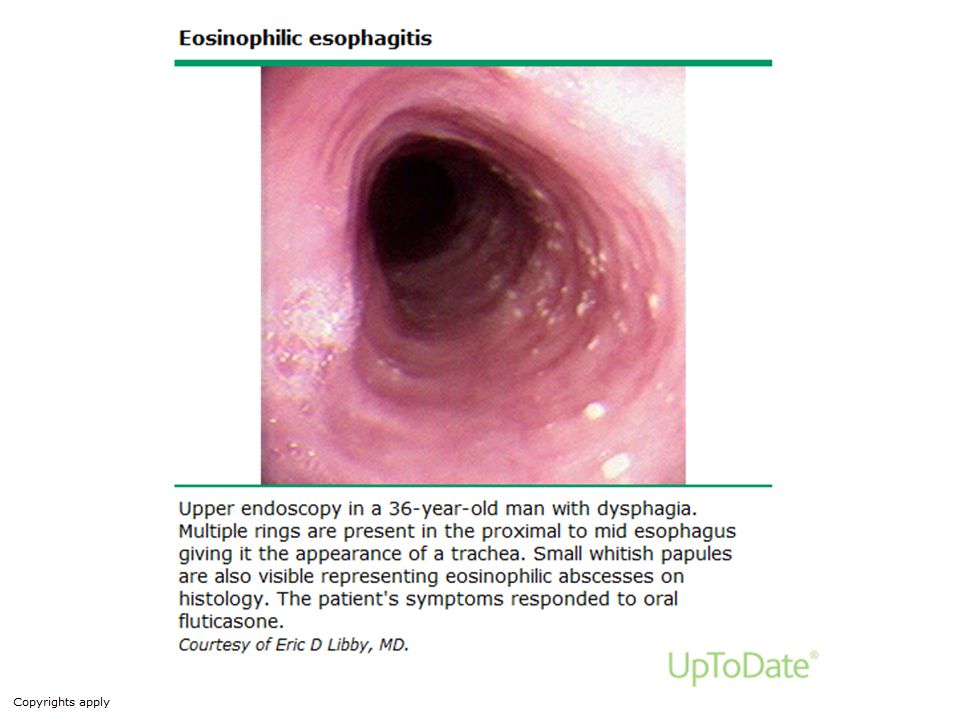
Mechanical Lesions, Intrinsic Most common Peptic stricture Lower esophageal (Schatzki) ring Carcinoma Other Esophageal webs Esophageal diverticula Benign tumors Foreign bodies
 ring. Carcinoma. Other. Esophageal webs. Esophageal diverticula. Benign tumors. Foreign bodies.")
23
Dysphagia Odynophagia Globus (pain in swallowing=odinophagia) Globus= something in my throat
 Globus= something in my throat")
24
Stable, intermittent, progressive
History Duration Stable, intermittent, progressive Speed of progression Liquids or solids

25
Alendronate (for Osteoporosis)
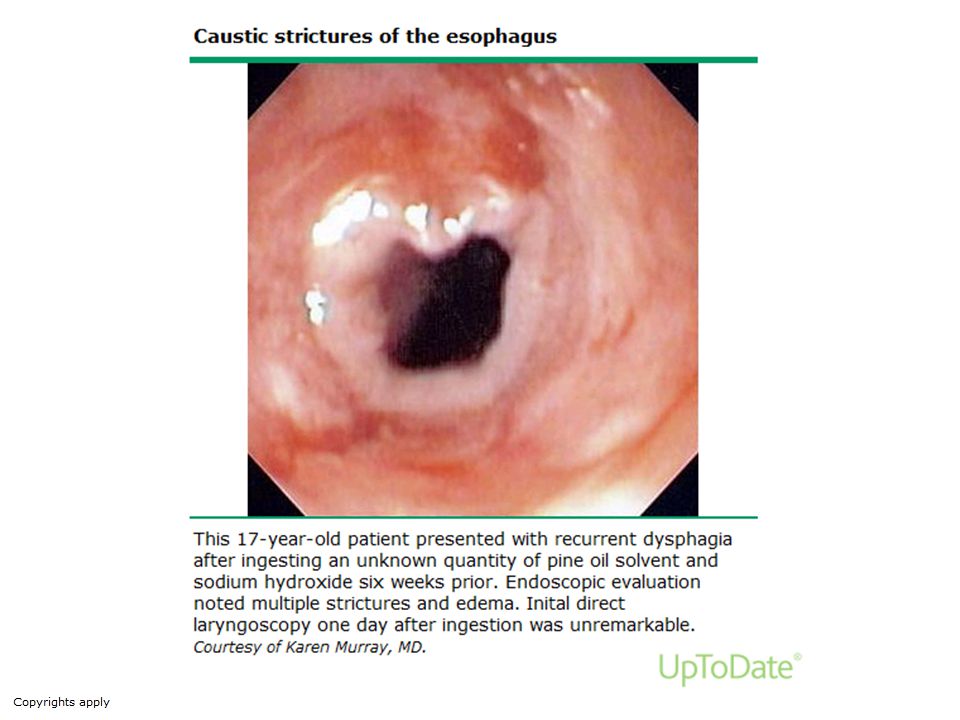
History Hx of drugs Tetracycline Alendronate (for Osteoporosis) Kostic injury
 Kostic injury.")
26
Diagnostic laparoscopy
Investigations Diagnostic Endoscopy Barium swallow Manometry Staging CT Diagnostic laparoscopy EUS

27
Biopsies Dilatation Stenting / laser ablation

31
Investigations for Staging
CT or MRI EUS Staging laparoscopy

32
Manometry -patients with no structural abnormality on endoscopy

33
Normal Swallow

34
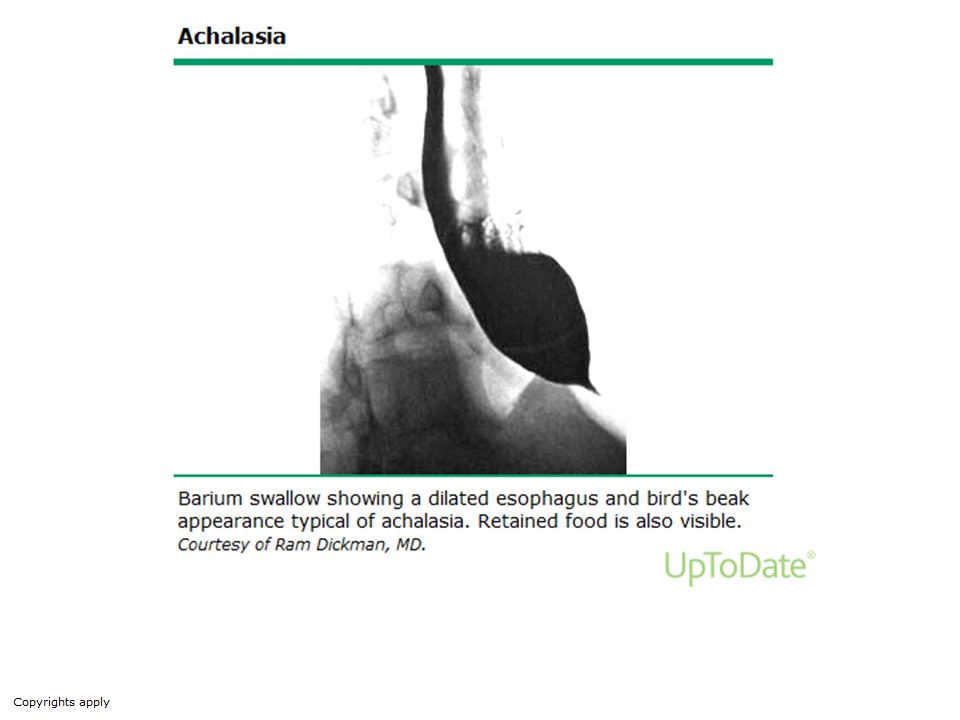
Oesophageal Motility Disorders Achalasia-Aetiology
Idiopathic- 98 % Primary Secondary Familial Associated with other congenital defects Associated with degenerative neurological disease

35
Oesophageal Motility Disorders Achalasia - Symptoms
Dysphagia – usually slowly progressive Regurgitation Chest pain and dysphagia Reflux symptoms

36
Oesophageal Motility Disorders Achalasia-Manometric features
Normal to raised LOS resting pressures LOS fails to relax to gastric baseline Raised residual pressures Raised oesophageal baseline pressures Absent or chaotic low amplitude simultaneous peristalsis

38
Achalasia Tracing

39
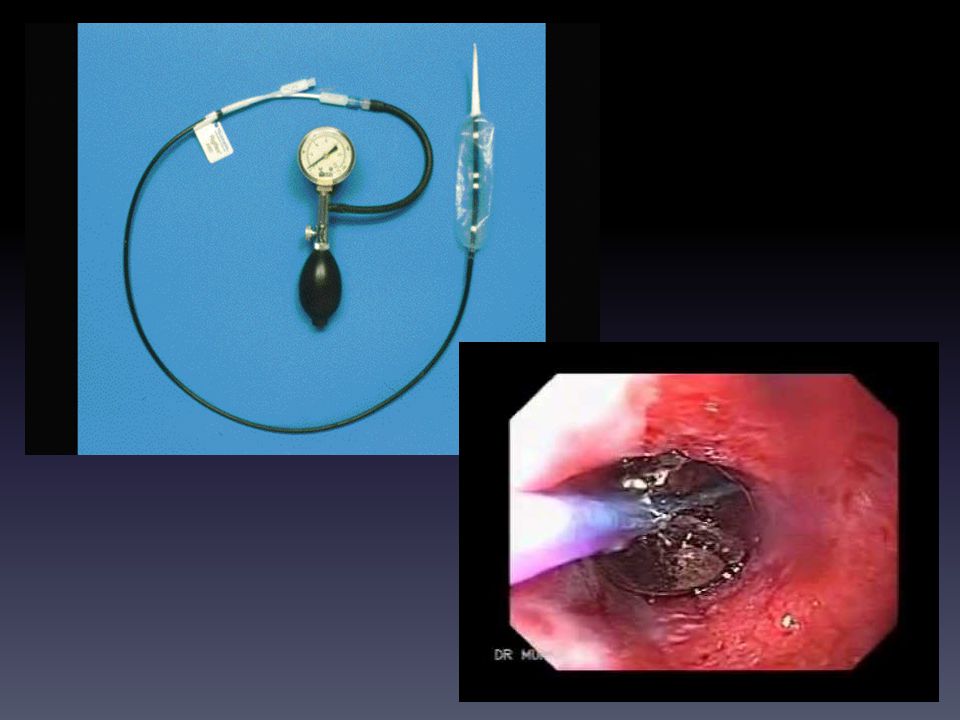
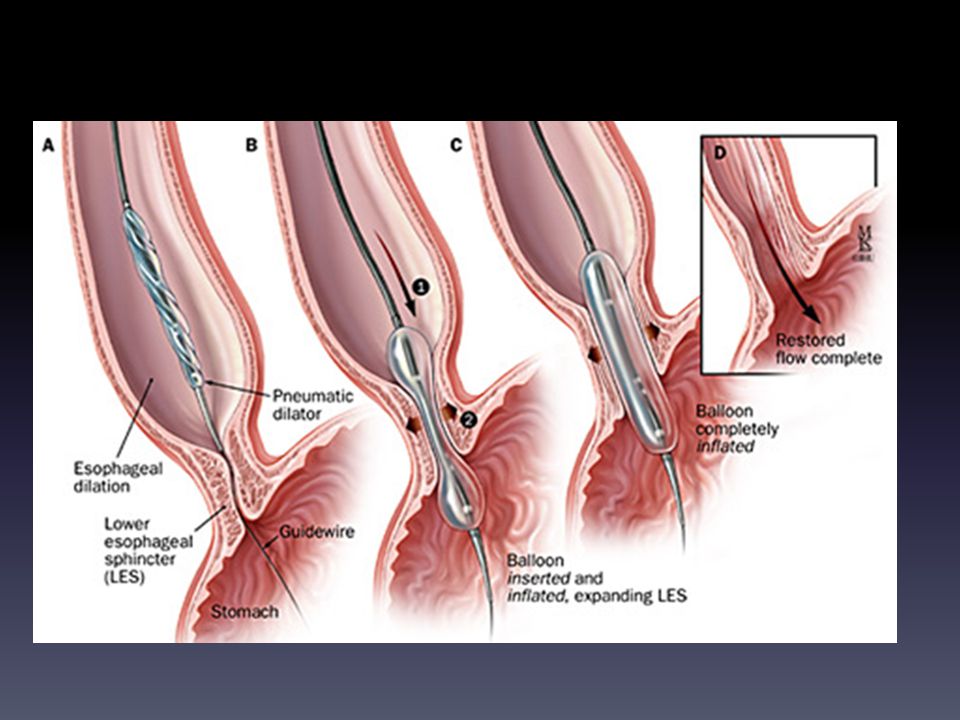
Oesophageal Motility disorders Achalasia-Treatment
Pneumatic dilatatation Risks Patient selection Botox injection Surgery Gastro-oesophageal reflux a significant complication

42
OESOPHAGEAL MOTILITY DISORDERS NUTCRACKER OESOPHAGUS
Most common cause of NCCP in those patients with an oesophageal motility disorder. Average distal pressures > 180 mm Hg. Peristalsis is normal so Ba studies usually normal. 90% present with chest pain.

43
Normal Swallow

44
Nutcracker Oesophagus

45
OESOPHAGEAL MOTILITY DISORDERS DIFFUSE ESOPHAGEAL SPASM
Intermittent dysphagia with occasional chest pain 90% present with chest pain. (Corkscrew esop) DES is characterized by the findings of simultaneous contractions greater than 30% of water swallows, with the presence of normal peristalsis. Other associated manometric findings may include repetitive contractions (>2 peaks), Prolonged contractions (>6 s), High-amplitude contractions (>180 mm Hg), Spontaneous contractions
 DES is characterized by the findings of simultaneous contractions greater than 30% of water swallows, with the presence of normal peristalsis. Other associated manometric findings may include repetitive contractions (>2 peaks), Prolonged contractions (>6 s), High-amplitude contractions (>180 mm Hg), Spontaneous contractions.")
51
DYSPHAGIA CONCLUSIONS
The symptom of dysphagia does not always indicate a physical obstruction Oesophageal motility disorders account for the majority of cases of dysphagia A normal endoscopy or Ba study does not exclude a motility disorder - role of oesophageal manometry Importance of mucosal biopsies of macroscopically normal mucosa

Similar presentations











 833-2090 www. med-speech.com.>")








; PGD (BIOETHICS)>")



