Download presentation
Presentation is loading. Please wait.

1
Rapid Sequence Intubation: drugs and concepts

2
Decision to Intubate Failure to maintain/protect airway Failure to ventilate/oxygenate Condition present or therapy required that mandates intubation Once you have decided that the patient requires tracheal integration the primary goal is to secure the airway quickly and as safely as possible to assure adequate oxygenation and ventilation

3
Rapid Sequence Intubation Definition The virtually simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to induce unconsciousness and motor paralysis for tracheal intubation.

4
Rapid Sequence Intubation Definition The virtually simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to induce unconsciousness and motor paralysis for tracheal intubation.

5
Rapid Sequence Intubation Definition The virtually simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to induce unconsciousness and motor paralysis for tracheal intubation.

6
Rapid Sequence Intubation Definition The virtually simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to induce unconsciousness and motor paralysis for tracheal intubation.

7
Rapid Sequence Intubation Definition Assumes: Patient has a full stomach No interposed ventilation Preoxygenation

10
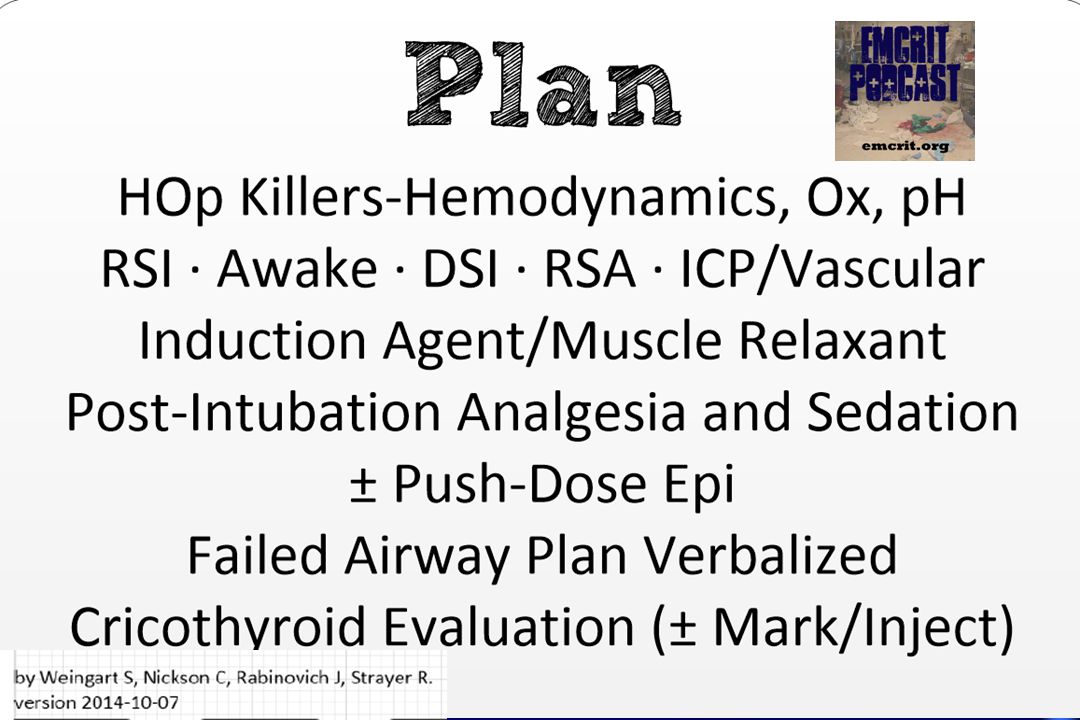
Rapid Sequence Intubation The Seven Ps of RSI P reparation P reoxygenation P retreatment P aralysis with induction P rotection P lacement P ost-Intubation Management

11
Rapid Sequence Intubation The Sequence Zero: the time of administration of paralytic

12
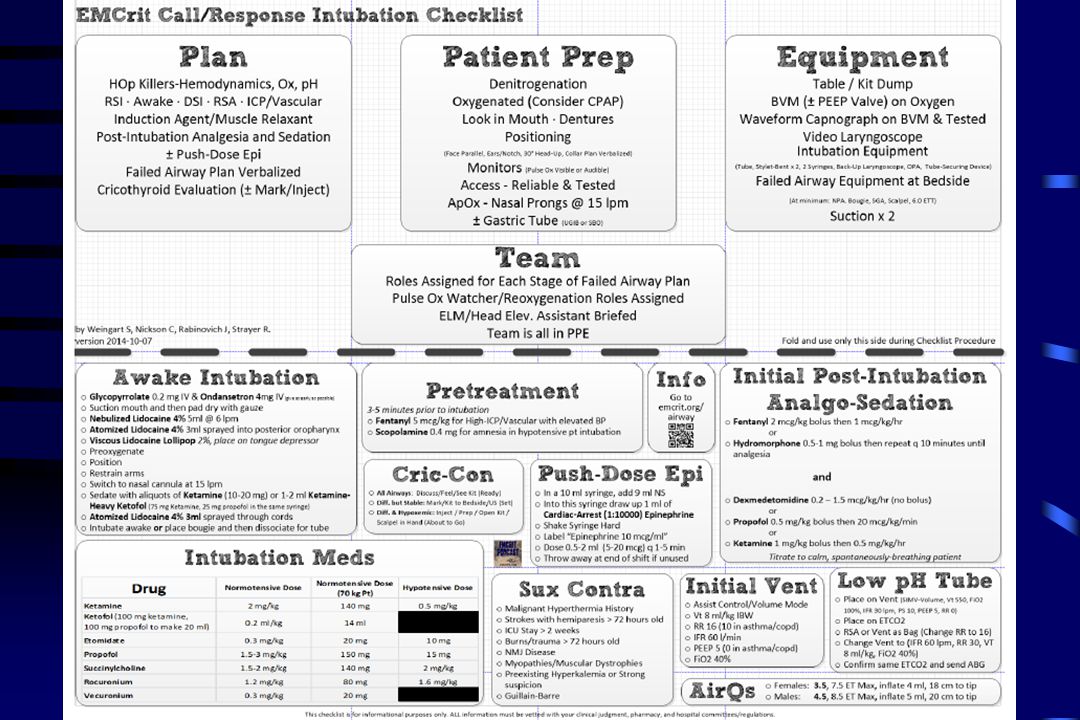
Rapid Sequence Intubation The Sequence Zero - 10 minutes Preparation Plan your approach ahead of time!! Assemble drugs and equipment Establish access, monitoring CHECKLIST!! Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

15
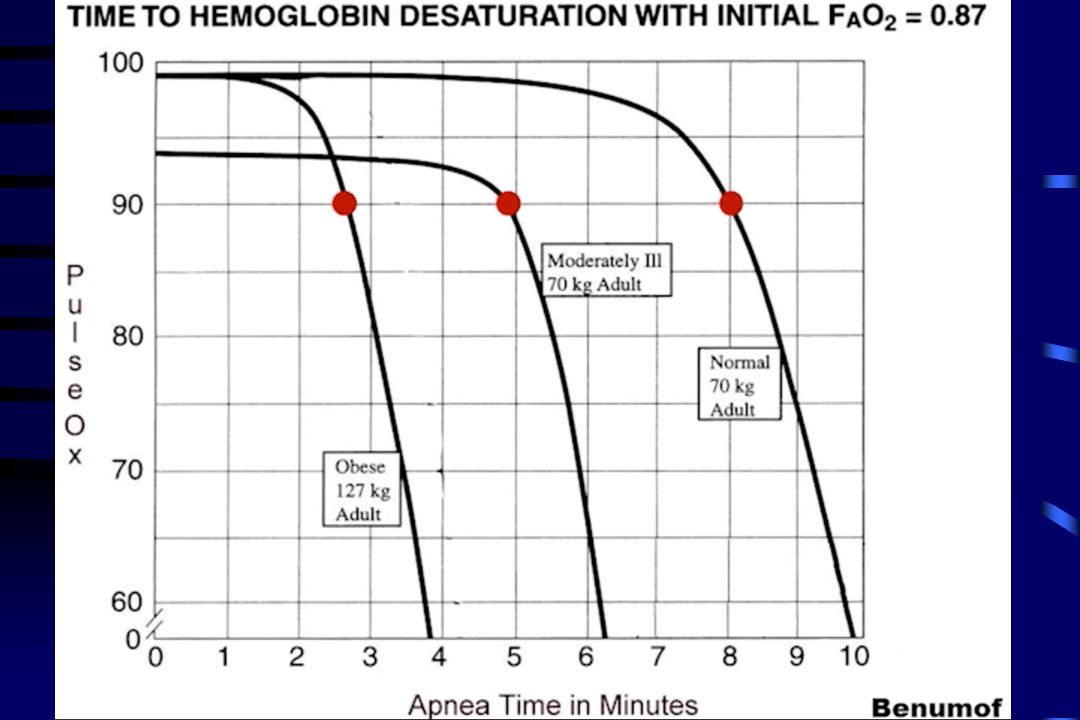
Rapid Sequence Intubation Zero - 5 minutes Preoxygenation De-Nitrogenate patient’s lungs- 8 VC BREATHS or 3 minutes Provides essential apnea time Apnea time varies NO DESAT- 15L nasal cannula 15L NRB If sats BVM with 15cmH20 PEEP The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

17
Rapid Sequence Intubation Zero - 5 minutes Preoxygenation De-Nitrogenate patient’s lungs Provides essential apnea time Apnea time varies NO DESAT-maintain airway open/HOB 30°NO DESAT 15L nasal cannula 15L NRB If sats BVM with 15cmH20 CPAP/PEEP The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation “Rule of 15s”

19
Rapid Sequence Intubation Zero - 5 minutes Preoxygenation De-Nitrogenate patient’s lungs Provides essential apnea time Apnea time varies NO DESAT 15L nasal cannula 15L NRB If sats BVM/PEEPval/CPAP @ 15cmH20 The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation Rule of 15s

21
DSI: Delayed Sequence Intubation

22
The Basics: “A procedural sedation, where the procedure is pre-oxygenation” * From EMCrit.org

24
Ph kills Pseudo- NIV with vent (not biPAP)- RR0 Give RSI meds Give breaths (RR12) during apnea time for 1 minute –slow,controlled breaths with jaw thrust Intubate, set vent to RR 30
- RR0 Give RSI meds Give breaths (RR12) during apnea time for 1 minute –slow,controlled breaths with jaw thrust Intubate, set vent to RR 30")
25
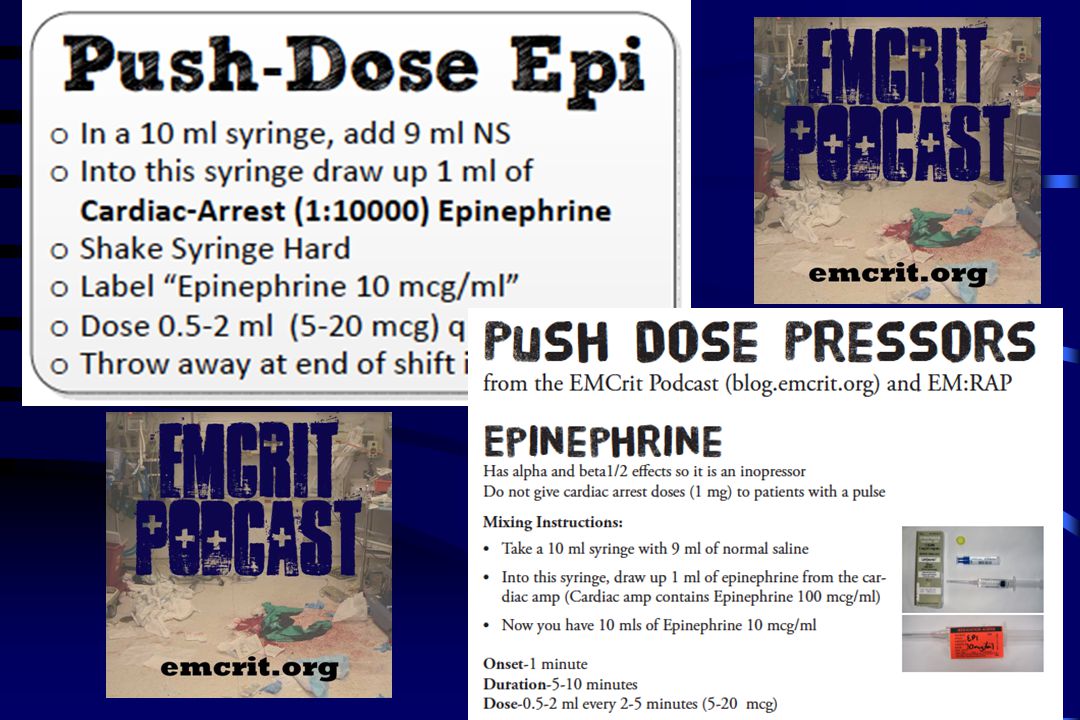
Rapid Sequence Intubation Zero - 3 minutes Pretreatment Fentanyl 5 mcg/kg for high ICP/Vascular with elevated BP Scopolamine 0.4 mg for amnesia in hypotensive patient intubation INOPRESSOR /IVFS- PDPS/Norepi gtt The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

27
Rapid Sequence Intubation Zero!! Paralysis with induction Induction agent Ketamine 2 mg/kg Etomidate 0.3 mg/kg Propofol 1.5-3 mg/kg Paralytic agent Rocuronium 1.2 mg/kg Succinylcholine 1.5-2.0 mg/kg The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

28
Ketamine

29
Dissociative sedative and analgesic Dissociates the CNS from outside stimuli by “disconnecting” thalamocortical and limbic systems Produces trancelike cataleptic state Maintain protective airway reflexes Very rapid onset - first pass effect low dose gives analgesia 0.2 mg/kg Moderate dose give analgesia and anxiolysis 0.5 mg/kg IV High Doses give amnesia and disassociation IV dose 1.5- 2 mg/kg IV)
")
30
Ketamine- Cautions Central adrenergic release, premedication with depressants (benzos) or fentanyl will probably blunt this response. MAP increased ~25 mmHg Probably has neuroprotective effect by NDMA antagonism, so no issues with elevated ICP patients-stroke and head injury True laryngospasm is exceedingly rare, probably just tongue obstruction. Inevitably resolves with airway positioning. The intraocular pressure increase has only been reported in animals Avoid in hyperthyroid states due to catecholamine release

31
Etomidate ultra–short-acting nonbarbiturate hypnotic No analgesic effect Dose: 0.2-0.3 mg/kg IV –Onset: > 1min –Duration: 3-5 mins

32
Etomidate it causes adrenal suppression which may be linked to increased mortality in septic patients (though many argue that etomidate is safe) it is unreliable as an induction agent in reduced doses (even in shocked patients) Good hemodynamic profile
 it is unreliable as an induction agent in reduced doses (even in shocked patients) Good hemodynamic profile")
33
Propofol potent, ultra–short-acting sedation and anesthesia It is a phenolic compound, and its mechanism of action is unknown, but it is thought to mediate GABA activity Propofol has no analgesic properties It is associated with rapid deepening of a sedation level to that of general anesthesia

34
Propofol Dose 0.5-1 mg/kg IV loading dose ; repeat 0.5 mg/kg q3-5 mins until desired depth of sedation Onset: < 1 min Duration 3-10 mins

35
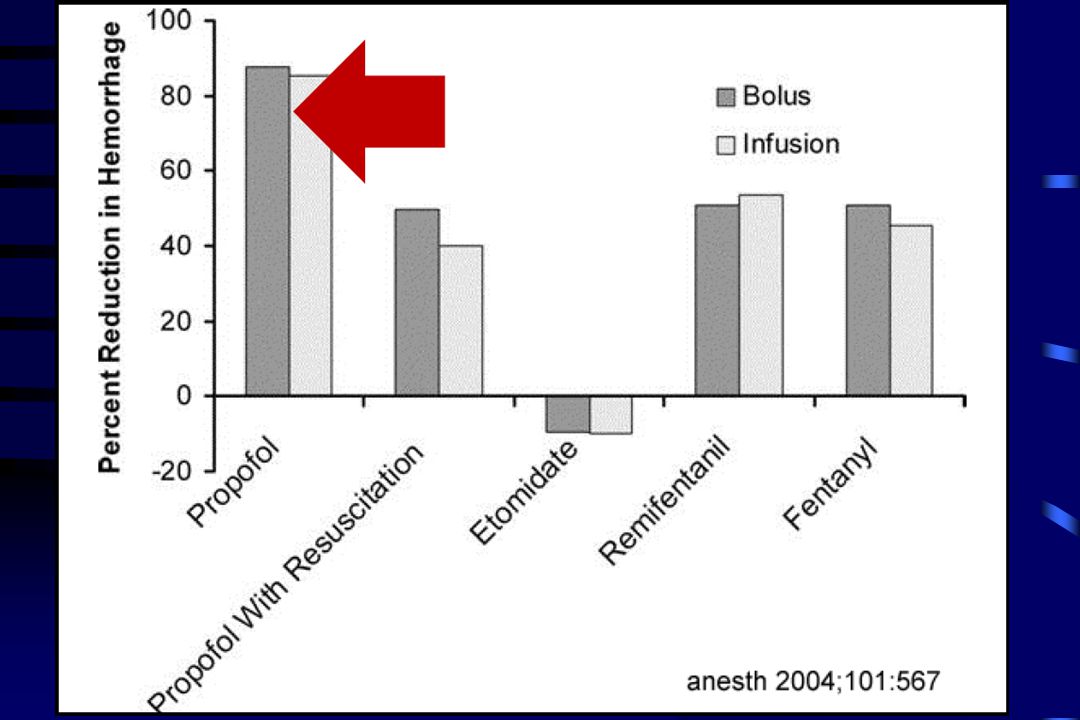
Adverse effects Hypoventilation/apnea- preO2!!, ETCO2!! Cardiovascular collapse/hypotension –Exacerbated in patients who are volume depleted Give IVFs up front

36
Ketofol Best of both worlds ! Deep sedation of propofol ( HR BP) + Dissociation, analgesia, maintenance of airway reflexes and sympathomimetic effects of ketamine = Hemodynamically balanced sedation agent
 + Dissociation, analgesia, maintenance of airway reflexes and sympathomimetic effects of ketamine = Hemodynamically balanced sedation agent .")
42
TBW IBW TBW

43
Rapid Sequence Intubation Zero + 30 seconds Protection Position patient- ear to sternal notch, face parallel Do not bag unless S p O 2 < 90% The Sequence Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

44
Rapid Sequence Intubation Zero + 45 seconds Placement The Sequence Intubate, remove stylet Confirm tube placement - ETCO 2 Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

45
Rapid Sequence Intubation Zero + 90 seconds Post-intubation Management The Sequence Secure tube Fentanyl push then drip OR Dilaudid pushes Sedation if necessary- propofol, ketamine or midazolam Establish ventilator parameters Preparation Preoxygenation Pretreatment Paralysis Protection Placement Post-Intubation

46
NEUROMUSCULAR BLOCKING AGENTS

47
Depolarizing - succinylcholine Competitive (nondepolarizing) eg rocuronium, vecuronium
 eg rocuronium, vecuronium")
48
Succinylcholine is a universally safe drug. No-one is too sick to get succinylcholine………

49
Succinylcholine has one very, very lethal side effect… Fatal Hyperkalemia

50
Succinylcholine Hyperkalemia Motor endplate proliferation burns, crush injuries stroke spinal cord injury MS, ALS, other denervations Myopathies Muscular dystrophy Mortality 11% Mortality 30%

51
Does Sux SUCK ? or Does Roc ROCK?

52
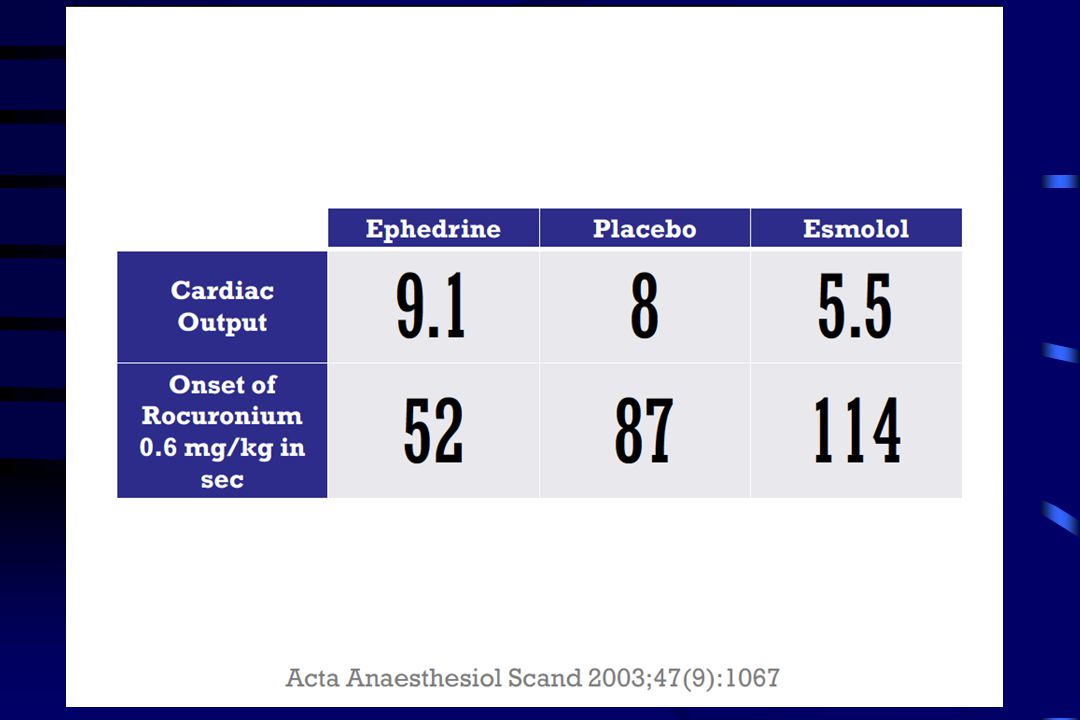
Sux vs Roc Succinylcholine –Used in 82% ED RSI –Faster onset to ETI conditions? –Onset = 60 sec –Duration = 3-15 min –Benefit:Stat epilepticus;ICH/stroke evals –Adverse effects K- do we know pts at risk? rhabdo ICP and IOP Masseter spasm Malignant hyperthermia Rocuronium –Onset = 45-60 sec (at 1.2 mg/kg) –Duration 30-90 min –Longer duration of safe apnea vs. sux (preox!) –Reversal in 2mins with Suggamadex? –Adverse effects None Prolonged paralysis? What if I can’t intubate? What if I can’t ventilate?
 –Duration min –Longer duration of safe apnea vs. sux (preox!) –Reversal in 2mins with Suggamadex. –Adverse effects None Prolonged paralysis. What if I can’t intubate. What if I can’t ventilate .")
54
Rapid Sequence Intubation The Seven Ps of RSI P reparation P reoxygenation P retreatment P aralysis with induction P rotection P lacement P ost-Intubation Management Summary

55
Review……. Plan Ahead Use checklist

57
Denitrogenate Preoxygenate Apneic oxygenation

58
pretreat

59
Dose smart

62
QUESTIONS??

Similar presentations






, FAAP(PEM)>")




>")






>")




