Download presentation
Presentation is loading. Please wait.

1
Developing Automated Communicable Disease Reporting: Two Pragmatic Technological Solutions
Kathryn Como-Sabetti, Asa Schmidt, Dede Ouren, Kathleen Steinmann, Matt Muscha, Richard Danila Minnesota Department of Health, HealthPartners Inc., Hennepin County Medical Center

2
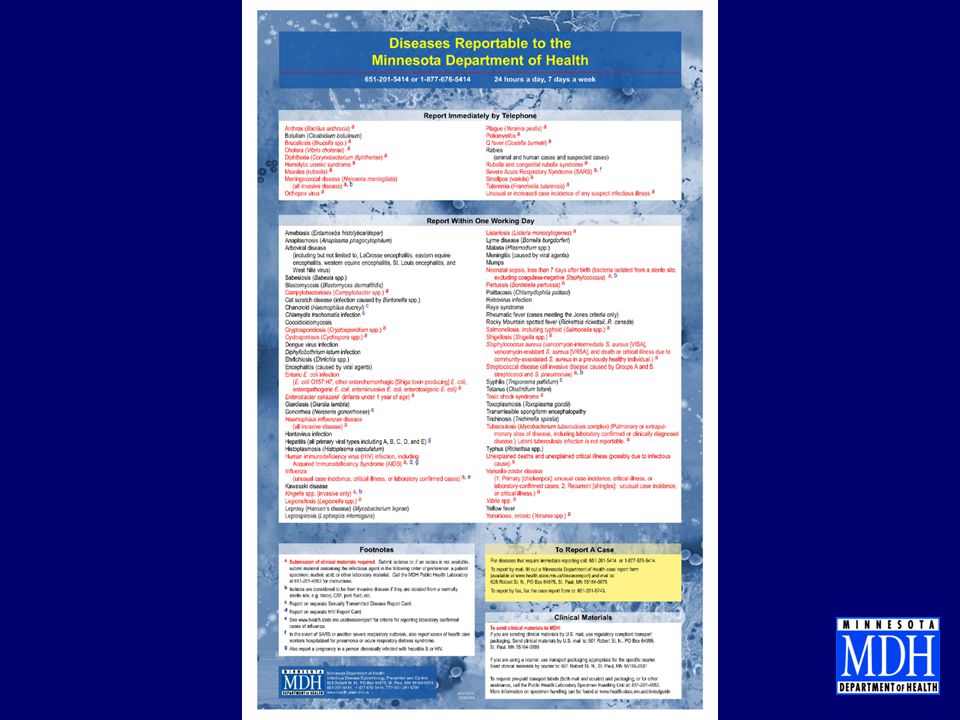
Minnesota Communicable Disease Reporting Rule
MN statute requires all licensed healthcare providers and laboratorians to report specific communicable disease 78 pathogens/syndromes are reportable 18 immediately reportable by phone 60 reportable within 1 working day Over 25,000 reportable communicable diseases received in 2010

4
Minnesota Communicable Disease Reporting Rule, cont.
Centralized communicable disease reporting Case investigation may be performed by local public health depending on pathogen and jurisdiction Minnesota is part of the Emerging Infection Program Increases the number of reportable diseases and complexity of reporting

5
Communicable Disease Reporting Process – Non Urgent Reports
IP Identifies reportable disease IP Reviews Chart and Completes CRF CRF Submitted to MDH (via fax, mail, phone or web) CRF Submitted to MDH (via fax, mail, phone or web) MDH receives CRF MDH enters information from CRF into program database MDH receives CRF Repeat multiple times per day MDH Enters Case Into Program Database IP Reviews Chart for Additional Information MDH Calls IP for additional Information (sometimes)
 CRF Submitted to MDH. (via fax, mail, phone or web) MDH receives CRF. MDH enters information from. CRF into program database. MDH receives CRF. Repeat multiple times per day. MDH Enters Case. Into Program Database. IP Reviews Chart for. Additional Information. MDH Calls IP for additional. Information (sometimes)")
6
Background Communicable disease reporting rule changed in 2004
MN-APIC/IPs expressed concern about the burden of increased reporting MDH agreed to look into ways to decrease reporting burden Fall 2006; MN-APIC authored a letter to the Commissioner of Health regarding the increasing burden of infectious disease reporting Difficult economic times force all agencies to “find efficiencies”

7
ADR vs ELR MDH has had a number of labs submitting communicable disease reports through electronic laboratory reporting (ELR). ELR had limited impact on disease reporting when ELR has very little case information. IPs still required to either complete a case report form

8
ADR vs ELR, cont. Automated disease reporting (ADR) includes demographic, contact, laboratory, and facility information Combines ELR with information from the patient’s electronic health record Decreases the number of case reports completed by IPs

9
MINNESOTA DEPARTMENT OF HEALTH COMMUNICABLE DISEASE REPORTING FORM
Disease Name: ________________________ Onset date:____/____/____ Report date:____/____/____ DEMOGRAPHIC INFORMATION LABORATORY AND FACILITY INFORMATION Name Last: ___________________________ First: ______________ MI: _________ Reporter Name: _______________________________ Phone: _____________________ DOB:____/____/____ Age:_____ Days Months Years Gender: Male Female Transgender Unknown Medical record #: ___________________________________________ Preferred language: English Other:________________________ Country of birth: U.S Other:______________ Unknown Address:___________________________________________________ Unknown Homeless City:______________________ State:____ Zip:_____ County:________________ Phone 1st:___________________ Phone 2nd:_____________________ Occupation:_______________ Parent/Guardian:_______________ Institution/Clinic: ______________________________ City: _________________________________________ Ordering provider:_____________________________ Phone:_______________________________________ Primary care provider: _________________________ Lab Name:_____________________________________ Phone:_________________________________________ MDH contact if additional information needed (choose at least one): Reporter Primary care provider Ordering provider Lab Other:_______________________________________________________ Was the patient hospitalized? Yes No Unknown Hospital name: _________________________________________________ Admit date: ____/____/____ Discharge date: ____/____/____ Died? Yes No Unknown If yes, date of death: ____/____/____ Ethnicity: Hispanic/Latino Non-Hispanic/ Non-Latino Unknown Race (check all that apply): American Indian/Alaskan Native Asian Black/African American White Native Hawaiian/Pacific Islander Unknown Other:______________________________ Specimen collection date: _____/_____/_____ Specimen source :______________________________________ Pregnant (if applicable): Yes No Unknown IF YES, due date: _____/_____/_____ Highlighted fields were identified as those in electronic medical records that could be pulled though an automated process. Revised 6/10
: Reporter Primary care provider Ordering provider Lab. Other:_______________________________________________________. Was the patient hospitalized Yes No Unknown. Hospital name: _________________________________________________. Admit date: ____/____/____ Discharge date: ____/____/____. Died Yes No Unknown If yes, date of death: ____/____/____. Ethnicity: Hispanic/Latino. Non-Hispanic/ Non-Latino. Unknown. Race (check all that apply): American Indian/Alaskan Native Asian. Black/African American White. Native Hawaiian/Pacific Islander Unknown. Other:______________________________. Specimen collection date: _____/_____/_____. Specimen source :______________________________________. Pregnant (if applicable): Yes No Unknown. IF YES, due date: _____/_____/_____. Highlighted fields were identified as those in electronic medical records that could be pulled though. an automated process. Revised 6/10.")
10
Solution #1 - Background
August 2007 RFA released by MDH for data mining systems to develop automated reporting to MDH 2 awards approximately $24,000 each No applications April 2009 RFA released by MDH for health systems to develop automated reporting to MDH 1 award up to $92,000 Awarded to HealthPartners/Region’s Hospital

11
Grant Objectives Automate the pull of demographic information from an electronic medical record and send an electronic case reports to MDH HealthPartners opted to automate the identification of reportable diseases Develop a roadmap for other institutions to develop ADR

12
Solution #1 - Process Teams were formed at HealthPartners and MDH and included experts from the Laboratory, Epidemiology, Infection Prevention, and Information Technology (IT) IT experts included: project management, message format, message transport, translation, and laboratory information systems Kick off meeting Monthly project conference calls
 IT experts included: project management, message format, message transport, translation, and laboratory information systems. Kick off meeting. Monthly project conference calls.")
13
Solution #1 – Implementation
681 tags of laboratory test/result combinations identified reportable diseases Once tagged, case reports were generated using Clarity extracting from the patient’s medical record (EPIC) Well Folks, it has been a long time coming but today is an exciting day. A big milestone in our process of automated disease reporting. We have just sent the first test/sample file to the state. This test file processed through all steps of the new process from rules evaluation, flagging, tagging, Clarity extracting, HL7 formatting to secure data transmission. I am just waiting for confirmation back from the state that the file has arrived. Our next big focus is to validate the readiness for test/result codes to be automated. To that end we have a detailed testing session setup on Friday September 10th with specific focus on test codes / result evaluation. This is to determine which of our test codes will be ready (approved) for actual activation on the automated process. This brings us to the threshold of seeing this become reality. Amazing what a small group of people can do! Thank you all! -Matt
 Well Folks, it has been a long time coming but today is an exciting day. A big milestone in our process of automated disease reporting. We have just sent the first test/sample file to the state. This test file processed through all steps of the new process from rules evaluation, flagging, tagging, Clarity extracting, HL7 formatting to secure data transmission. I am just waiting for confirmation back from the state that the file has arrived. Our next big focus is to validate the readiness for test/result codes to be automated. To that end we have a detailed testing session setup on Friday September 10th with specific focus on test codes / result evaluation. This is to determine which of our test codes will be ready (approved) for actual activation on the automated process. This brings us to the threshold of seeing this become reality. Amazing what a small group of people can do! Thank you all! -Matt.")
14
Solution #1 – Implementation
Sunquest 1. Lab results in LIMS (sunquest) triggers the feed EPIC 2. Information is passed on to the HER (EPIC), for case information HL7 3. HL7 message is created PHIN-MS 4. Transfer of file to MDH Rhapsody 5. Upload of data into MEDSS 6. IP staff at regions have access to add additional information manually
 triggers the feed. EPIC. 2. Information is passed on to the HER (EPIC), for case information. HL7. 3. HL7 message is created. PHIN-MS. 4. Transfer of file to MDH. Rhapsody. 5. Upload of data into MEDSS. 6. IP staff at regions have access to add additional information manually.")
15
DEPARTMENT Infection Prevention Microbiology LIS IT TASK
format HL7 results from LIS to EHR system confirm the English Text Code tag interpretation confirm reportable flag confirm extracted data is formatted in the proper sequence HL7 format has data elements mapped into agreed locations confirm standard encrypted EDI transmission from RH to MDH data communication is functional DEPARTMENT Infection Prevention Microbiology LIS IT

16
Solution #2 - Background
Hennepin County Medical Center (HCMC) contracted with Premier to implement SafetySurveillor for healthcare associated infection surveillance Included in the contract was a provision that SafetySurveillor would develop reports identifying reportable communicable diseases
 contracted with Premier to implement SafetySurveillor for healthcare associated infection surveillance. Included in the contract was a provision that SafetySurveillor would develop reports identifying reportable communicable diseases.")
17
Solution #2 - Process 4 reports were developed by HCMC and Premier to identify cases: Communicable disease report to identify cases by pathogen only Communicable disease report to identify cases by pathogen and specimen source Neonatal sepsis report (pathogen and patient DOB) Invasive MRSA report
 Invasive MRSA report.")
18
Solution #2 – Process, cont.
Paper reporting by healthcare providers for STDs continues with ADR reporting to audit Process to identify treatment is not automated but necessary for STD reports MDH approved message format Message includes demographic, contact, laboratory, hospitalization and provider information

19
Solution #2 – Process, cont.
Team was not formed Facility IP coordinated development of SafetySurveillor reports IP coordinated IT assistance as needed at the facility

20
Solution #2 – Implementation
Premier 1. Reports run by HCMC staff in the Premier system .csv 3. Flat file is created PHIN-MS 4. Transfer of file to MDH Rhapsody 5. Upload of data into MEDSS 6. IP staff at HCMC have access to add additional information manually

21
Current Status Solution #1
MDH receives files daily from HP Implementation is going through a validation step to confirm all data is correct Upload into MEDSS will create new disease events in the system De-duplication will try to match to existing persons and events. Disease events will be listed on daily workflows for epis (routing is based on disease) IPs at HP are being trained on MEDSS
 IPs at HP are being trained on MEDSS.")
22
Current Status Solution #2
MDH receives files twice a week from HCMC MDH staff time saved for reviewing HCMC charts Files are manually routed to disease program staff MEDSS team is currently working on mapping the message into MEDSS Approximate 20% of chlamydia and gonorrhea was not reported by providers

23
Lessons learned ADR improved disease reporting at HCMC
Manual process of running ADR reports resulted in reports not being sent daily ADR decreases the burden of infectious disease reporting on healthcare facility staff Once in MEDSS we expect ADR will decrease MDH staff time spent entering records

24
Lessons learned, cont. There is no standard. Rules for the what tests/results to send are unique Early discussions about when to send data is essential Lab/IP staff provide the knowledge IT/Lab/IP/EPI partnership essential Team approach lead to smoother implementation IP provides clinical interpretation

25
Lessons learned, cont. Creating the ADR message was complicated without a standard to fall back on, we ended up modifying the HL7 message for ELR reporting Standardized coding of tests and results would make it easier to route to the correct program areas/epis When data is sent from one system to another information gets lost Example: Coded test/results in LIMS were passed on as text to the EHR system, forcing us to translate them back after we received it.

26
Lessons learned, cont. A practical focus made it possible
What data elements can we rely on? If we can’t trust the data don’t try to get it if its complicated What is our goal? If we want things to be easier for the IPs and we manage to do an automated transfer of 80% of the cases, can’t they then do the rest manually if we give them the tools? If we maintain the process of ‘report immediately by telephone’ for the conditions that needs this we got our EPIs to be more confident in the process

27
Questions and Contact Information Asa Schmidt, Project Manager Kathryn Como-Sabetti, Epidemiologist

Similar presentations

 Chronic Diseases, Outpatient Flow Patient, Provider/Physician, Laboratory, PH.>")
 Maven configurability (15 min) ELR and De-duplication, overview.>")
 How it works.>")
-384-1608>")














