Download presentation
Presentation is loading. Please wait.

1
Multiple Myeloma Pamela S. Becker, MD, PhD Associate Professor Division of Hematology

2
Case I: 44 yo F 17 mo ago back pain 12 mo ago skin rash-annular then maculopapular erythematous rash that was biopsied R shoulder, then a second biopsy posterior arm. Involved face, neck, arms, chest. Occasional pruritus.

3
Case I, cont’d Sweet’s syndrome-Prescribed Prednisone 6 mo. Prior, 40 mg, then 2 mo. prior, 20 mg Sudden onset severe back pain 7/04-ambulance to hosp LABS: CBC: WBC 6.2, hemoglobin 10.6, hematocrit 31.1, platelet count 232K Urinalysis: 3-5 white cells, Leuk esterase, 1+ protein, E.Coli Chem: BUN 40, creatinine 2.0, uric acid 11.6, calcium 13.5, albumin 2.8, total bilirubin 0.18, alk phos 153, AST 35, ALT 40. TP 12.3, gamma globulin 6.2, Monoclonal protein 5.8 gm/dl IgA kappa CT scans: 3.5 x 1.5 cm mass in the post L chest, a mass in the right psoas, L1-L3, Bone marrow biopsy performed:80-90% plasma cells

4
MRIs L-spine: mass displacing right psoas muscle laterally involving L1 and L2 neural foramina on the right, with possible erosion of L2 right lateral vertebral margin. T spine: comp fx of T5, T10, L1, and L2 C spine: 3 x 3 cm mass.

5
Therapy 7-04-Chemotherapy 75 mg Doxorubicin, 1200 mg Cytoxan, 2 mg vincristine, Dexamethasone 4 mg qid, and Aredia 30 mg X 2 ANC 0.2 on day 7 Neupogen 300 mcg then 480 mcg RBC-4 units Seen on day 12-Recurrent rash, WBC 3.76, beta2 microglobulin 2.4

6
Next therapy Thalidomide/Dex began 8/04 MRI end 9/04: mass L2 to L3 vertebral region 4.6 X 3.1 x 0.8 cm. R L2 and L3 neural foramina, ? R L3 nerve root. Comp fx L3, L4, L5. L lat sacrum enhancing lesion 2.5 X 2 cm. Chest CT: cardiomegaly, mid T vertebrae sclerotic changes,comp fx, acute kyphotic deformity, possible fx through body of sternum. Monoclonal protein 5.8 (7/21) 2.6 (7/28), 0.4 8/30, 0.6 (10/14), 0.9 (2/10) Radiation to L spine Began Velcade/Doxil-monoclonal protein down to 0.8 post first cycle, now s/p 2 nd cycle
 2.6 (7/28), 0.4 8/30, 0.6 (10/14), 0.9 (2/10) Radiation to L spine Began Velcade/Doxil-monoclonal protein down to 0.8 post first cycle, now s/p 2 nd cycle.")
7
Next treatment: Tandem transplant Auto Mini allo from HLA matched sister

8
Multiple Myeloma: Incidence and Epidemiology 1% of all malignancies 10% of hematological malignancies (2 nd most common) 3-4 per 100,000 population 16,000 new cases/yr; 11,000 deaths/yr Median age: 65 yo; 3%<40 yo M>F Risk: radiation exposure
 3-4 per 100,000 population 16,000 new cases/yr; 11,000 deaths/yr Median age: 65 yo; 3%<40 yo M>F Risk: radiation exposure")
9
Myeloma: Pathogenesis

10
International Working Group Classification Monoclonal gammopathy of undetermined significance (MGUS) Asymptomatic (Smouldering) myeloma [Indolent myeloma] Symptomatic myeloma Non-secretory myeloma Solitary plasmacytoma of bone Extramedullary plasmacytoma Multiple, recurrent plasmacytomas Plasma cell leukemia
![International Working Group Classification Monoclonal gammopathy of undetermined significance (MGUS) Asymptomatic (Smouldering) myeloma [Indolent myeloma] Symptomatic myeloma Non-secretory myeloma Solitary plasmacytoma of bone Extramedullary plasmacytoma Multiple, recurrent plasmacytomas Plasma cell leukemia](http://images.slideplayer.com/19/5900264/slides/slide_10.jpg "International Working Group Classification Monoclonal gammopathy of undetermined significance (MGUS) Asymptomatic (Smouldering) myeloma [Indolent myeloma] Symptomatic myeloma Non-secretory myeloma Solitary plasmacytoma of bone Extramedullary plasmacytoma Multiple, recurrent plasmacytomas Plasma cell leukemia")
11
Multiple myeloma: Symptoms Fatigue Back pain Increased infections Hypercalcemia Renal insufficiency Hyperviscosity

12
Multiple Myeloma: Diagnosis Bone marrow containing more than 10% plasma cells or a plasmacytoma, plus at least one of the following: 1)a monoclonal protein in the serum, usually more than 30 g/L 2)a monoclonal protein in the urine OR 3)lytic bone lesions
a monoclonal protein in the serum, usually more than 30 g/L 2)a monoclonal protein in the urine OR 3)lytic bone lesions")
13
Bone Marrow Plasma Cells

14
Bone marrow plasmacytosis

15
Serum Protein Electrophoresis (SPEP) Albumin 1 2 M-protein
 Albumin 1 2 M-protein")
16
κλκλ

17
Rouleaux on peripheral smear

18
Multiple Myeloma: Durie-Salmon Staging

19
Multiple myeloma: New staging (International Staging System) Based on Beta 2 microglobulin and albumin I.β2M <3.5 + Alb ≥ 3.5 Med surv 62 m II.In between Med surv 44 m III.β2M >5.5 Med surv 29 m
 Based on Beta 2 microglobulin and albumin I.β2M <3.5 + Alb ≥ 3.5 Med surv 62 m II.In between Med surv 44 m III.β2M >5.5 Med surv 29 m")
20
Multiple Myeloma: Indication for Treatment: CRAB Calcium (Hypercalcemia) Renal insufficiency Anemia Bone lesions
 Renal insufficiency Anemia Bone lesions")
21
Monoclonal Gammopathy of Uncertain Significance Often Benign; Over Many Years May Eventually Develop Into Myeloma or Other Lymphoproliferative Disorders; May Be Associated With Tumors –Monoclonal Gammopathy –M-component Level Igg < 3.5 G/dl Iga < 2.0 G/dl BJ Protein < 1.0 G/24 H –Bone Marrow Plasma Cells < 10% –No Bone Lesions –No Symptoms

22
Non secretory myeloma –no secretion of protein (relatively rare if serum and urine carefully studied for presence of M- protein) –prognosis same as myeloma or longer
 –prognosis same as myeloma or longer")
23
Plasmacytoma Solitary plasmacytoma of bone –Usually progress, slowly, to myeloma Extramedullary plasmacytoma –Upper respiratory tract including nasal cavity, sinuses, nasopharynx, larynx; other sites possible –some progress to myeloma

24
Plasma cell leukemia –loss of adhesion molecules that localize in marrow (CD56, VLA-5, MPC-1) –greater than 20% plasma cells in blood and > 2000/ul –more frequent: younger age, hepatosplenomegaly, lymphadenopathy, few lytic lesions, small M-protein, poor prognosis
 –greater than 20% plasma cells in blood and > 2000/ul –more frequent: younger age, hepatosplenomegaly, lymphadenopathy, few lytic lesions, small M-protein, poor prognosis")
25
Amyloidosis Amyloid: homogenous, amorphous extracellular material with fibrillar structure; made of low MW proteins that precipitate in tissues

26
Amyloidosis, cont’d Reactive systemic amyloidosis: –Amyloid protein A derived from catabolism of serum amyloid A- related protein (SAA), an acute phase protein; excess production in chronic inflammatory or infectious disorders, may result in deposition in tissues Amyloid Due to an Immunologic-related Disorder –Insoluable Catabolic Product of the Variable Region of a Light Chain, Lambda; –May Occur As a Result of Myeloma or Waldenstrom’s Macroglobulinemia Primary Amyloidosis –Deposits in Joint Capsules, Ligaments, Tongue, Heart (CHF), GI Tract (Diarrhea), Peripheral Nerves (Paresthesias, Weakness, Orthostatic Hypotension), Small Vessel Fragility From Amyloid in Walls (Purpura), Factor X Deficiency Due to Its Binding in the Extracellular Tissues
, an acute phase protein; excess production in chronic inflammatory or infectious disorders, may result in deposition in tissues Amyloid Due to an Immunologic-related Disorder –Insoluable Catabolic Product of the Variable Region of a Light Chain, Lambda; –May Occur As a Result of Myeloma or Waldenstrom’s Macroglobulinemia Primary Amyloidosis –Deposits in Joint Capsules, Ligaments, Tongue, Heart (CHF), GI Tract (Diarrhea), Peripheral Nerves (Paresthesias, Weakness, Orthostatic Hypotension), Small Vessel Fragility From Amyloid in Walls (Purpura), Factor X Deficiency Due to Its Binding in the Extracellular Tissues")
27
Organ involvement by amyloidosis

28
POEMS (polyneuropathy, organomegaly, endocrinopathy, M-protein, skin changes) –Peripheral neuropathy usually first sign –Papilledema, hyperpigmentation, organomegaly –< 5% plasma cells in marrow –Association with Castleman’s disease –Anemia, rare; usually Hct normal or polycythemia, thrombocytosis –Single lytic lesions improved with radiation; may have neurologic improvement as well –Gynecomastia, atrophic testes, clubbing
 –Peripheral neuropathy usually first sign –Papilledema, hyperpigmentation, organomegaly –< 5% plasma cells in marrow –Association with Castleman’s disease –Anemia, rare; usually Hct normal or polycythemia, thrombocytosis –Single lytic lesions improved with radiation; may have neurologic improvement as well –Gynecomastia, atrophic testes, clubbing")
29
Case 2-57 yo F Referred for eval of leukopenia (WBC 3) WBC 5.27, hgb 12.8, platelets 231K ANA neg SPEP 0.3 g/dl monoclonal IgG lambda Quantitative Bence Jones: Negative Skeletal survey: Negative Bone marrow: Lambda restricted plasma cells 0.6% by flow; 6% by morphology with rare multinucleated plasma cells and some with prominent nucleoli DIAGNOSIS: ___________ Follow-Up: 18 months later: SPEP: 0.4 g/dl
 WBC 5.27, hgb 12.8, platelets 231K ANA neg SPEP 0.3 g/dl monoclonal IgG lambda Quantitative Bence Jones: Negative Skeletal survey: Negative Bone marrow: Lambda restricted plasma cells 0.6% by flow; 6% by morphology with rare multinucleated plasma cells and some with prominent nucleoli DIAGNOSIS: ___________ Follow-Up: 18 months later: SPEP: 0.4 g/dl")
30
Case 3-48 yo Hisp M Right femur fracture on Orthopaedics Flow from OR specimen: 2.9% clonal plasma cells SPEP 1.3 g/dl monoclonal IgG kappa, also IgA lambda two bands UPEP: same as above, and faint kappa light chains Bone marrow: 47% plasma cells

31
Case 3 cont’d Enrolled on Southwest Oncology Group Trial of Lenalidomide vs. Placebo + Dexamethasone Follow up studies at 3 months: SPEP: progressive decline, down to 0.8 g/dl. Bone marrow plasmacytosis: 15-20% plasma cells 10 months: 0.5 g/dl 11 months: 0.7 g/dl

32
Case 4: 51 yo M Running track, developed back pain, difficulty walking CT scan: L1 lytic lesion 1.9 X 2.3 cm Needle biopsy: Clonal plasma cells SPEP negative, UPEP negative Bone marrow survey by MRI negative PET scan negative DIAGNOSIS: ____________ Treatment: Radiation Therapy Future: 80% of vertebral plasmacytomas myeloma

33
Multiple Myeloma: Therapy Melphalan/Prednisone VAD (now DVD) Thalidomide/Dexamethasone Lenalidomide/Dexamethasone Bortezomib and combinations Autologous Stem Cell Transplant Minimal myeloablative Allogeneic Transplant Tandem Transplants
 Thalidomide/Dexamethasone Lenalidomide/Dexamethasone Bortezomib and combinations Autologous Stem Cell Transplant Minimal myeloablative Allogeneic Transplant Tandem Transplants")
34
ECOG E1A00: phase 3, randomized, controlled trial Newly diagnosed, untreated symptomatic MM (N = 207) Thal/Dex arm Thalidomide 200 mg/day PO + Dexamethasone 40 mg/day on Days 1-4, 9-12, 17-20 (n = 103) Dex alone arm Dexamethasone 40 mg/day on Days 1-4, 9-12, 17-20 (n = 104) Repeated monthly for 4 mos Stem-cell transplant or continue therapy at physician’s discretion Stop therapy Rajkumar V, et al. ASH 2004. Abstract 205. Note: Use of prophylactic anticoagulant not required. Use of Dexamethasone With or Without Thalidomide in Frontline Therapy CR/PR/ Stable Any progression

35
Use of Dexamethasone With or Without Thalidomide in Frontline Therapy 0 10 20 30 40 50 60 70 80 90 100 Response* ThaI/Dex (n = 99) Dex alone (n = 100) Patients (%) Corrected Response † Complete Response 4% 0% 41% 50% 63% 73% P =.002 * ↓ in serum M protein and urine M protein † ↓ in serum M protein (no available urine M protein) Response after 4 cycles DVT Gr > 3 Neuropathy Gr > 3 All Gr > 4 toxicity Grade 3 or 4 toxicity Deaths ThaI/Dex (n = 102) Dex alone (n = 102) 0 10 20 30 40 50 60 70 80 90 100 17% 3% 7% 4% 34% 18% 7% 11% Patients (%) Rajkumar V, et al. ASH 2004. Abstract 205.

36
MPT arm Oral melphalan 4 mg/m 2 (7 days/mo) Prednisone 40 mg/m 2 (7 days/mo) Thalidomide 100 mg/day (continuously) (n = 89) Newly diagnosed elderly myeloma patients Median age, 72 yrs (60-85) (N = 177 ) MP arm Oral melphalan 4 mg/m 2 (7 days/mo) Prednisone 40 mg/m 2 (7 days/mo) (n = 88 ) 6 mos Palumbo A, et al. ASH 2004. Abstract 207. Use of Melphalan Plus Prednisone With or Without Thalidomide in Frontline Therapy Interim analysis of prospective, randomized trial

37
Use of Melphalan Plus Prednisone With or Without Thalidomide in Frontline Therapy 0 10 20 30 40 50 60 70 80 90 100 Response (%) Progression No response (0-50*) MPTMP Partial response (50-99*) 27.7% PR (75-99*) 33.8% PR (50-74*) 15.6% 14.5% 8.4% PR (75-99*) 13.3% PR (50-74*) 28% 25.3% 28% 77.1% 41.3% Palumbo A, et al. ASH 2004. Abstract 207. * % reduction in baseline M protein 49.4% CR+nCR 5.4%

38
New Agents: Lenalidomide New agents needed to address concerns regarding high rate of nonhematologic toxicity seen with thalidomide CC-5013 (lenalidomide) is a potent analogue of thalidomide –Promising results in relapsed or refractory MM –Significantly fewer nonhematologic toxicities Less peripheral neuropathy, constipation, sedation –However, associated with neutropenia and thrombocytopenia Thalidomide CC-5013 (Lenalidomide)
 is a potent analogue of thalidomide –Promising results in relapsed or refractory MM –Significantly fewer nonhematologic toxicities Less peripheral neuropathy, constipation, sedation –However, associated with neutropenia and thrombocytopenia Thalidomide CC-5013 (Lenalidomide)")
39
Bortezomib With and Without Dexamethasone in Frontline Therapy Phase 2 study evaluated use of bortezomib later supplemented with dexamethasone to boost response in newly diagnosed patients with MM Treatment schedule –Bortezomib (1.3 mg/m 2, twice weekly for 2 wks) Administered every 3 wks for up to 6 cycles Given alone for first 2 cycles –Dexamethasone (40 mg/day) on day of and day after bortezomib Added after 2 cycles if < partial response Added after 4 cycles if < complete response Jagannath S, et al. ASH 2004. Abstract 333.

40
Combination Bortezomib, Thalidomide, Plus Dexamethasone (VTD) in Frontline Therapy Phase 1/2 trial of frontline bortezomib combined with thalidomide + dex 30 previously untreated patients with MM received –Thalidomide (100-200 mg/day) –Dexamethasone (20 mg/m 2 ) PO Days 1-4, 9-12, 17-20 –Bortezomib (1.0, 1.3, 1.5, 1.7, 1.9 mg/m 2 ) Days 1, 4, 8, 11 –Every 4 wks for 2-3 cycles Alexanian R, et al. ASH 2004. Abstract 210. 0 20 40 60 80 100 TD alone † All doses ≤ 1.3≥ 1.5 Response Rate*, % VTD P =.18 P =.04 68% 80% 64% 94% † Historical controls from nonrandomized study * Stringent response criteria: ≥ 75% reduction in serum M protein ≥ 95% reduction in Bence Jones protein

41
Pulsed Melphalan, Dexamethasone, and Thalidomide in Frontline Therapy Multicenter, phase 2 study of pulsed melphalan, dexamethasone, and thalidomide in 50 elderly patients with untreated, symptomatic MM –≥ 75 yrs of age –Poor performance status (58% had PS ≥ 2) –Advanced-stage disease (58% had ISS 3) Treatment schedule (3 courses every 5 wks, all oral) –Melphalan (8 mg/m 2 ) Days 1-4 –Dexamethasone (12 mg/m 2 ) Days 1-4 and 14-18 Intensity less than half that of standard high-dose dexamethasone –Thalidomide (300 mg) Days 1-4 and 14-18 Intermittent dosing used Dimopoulos MA, et al. ASH 2004. Abstract 1482.

42
Pulsed Melphalan, Dexamethasone, and Thalidomide in Frontline Therapy 68.2% of patients responded –Partial response, 61.4% –Complete response, 6.8% –Median time to response, 2 mos (range 0.5-14.0) Generally well tolerated –25 infectious episodes 1 fatality Other adverse events –Gr 3/4 neutropenia (15%) –Gr 3/4 thrombocytopenia (10%) –Somnolence (35%) –Constipation (30%) –Tremors (25%) –Xerostomia (15%) –Headaches (10%) –DVT (10%) –Peripheral neuropathy (10%) Dimopoulos MA, et al. ASH 2004. Abstract 1482.

43
Treatment of Relapsed/Refractory Multiple Myeloma

44
Bortezomib vs Dexamethasone in Relapsed/Refractory Multiple Myeloma Patients with relapsed or refractory MM (N = 669) Stratified by: No. of prior therapies Refractory disease B-2 microglobulin Bortezomib Arm Induction: 1.3 mg/m 2 IV Days 1, 4, 8, 11 q3 wks for 8 cycles Maintenance: 1.3 mg/m 2 IV Days 1, 8, 15, 22 q5 wks for 3 cycles (n = 333) Dexamethasone Arm Induction: 40 mg PO Days 1-4, 9-12, 17-20 q5 wks for 4 cycles Maintenance: 40 mg PO Days 1-4 q4 wks for 5 cycles (n = 336) Richardson P, et al. ASH 2004. Abstract 336.5. APEX: international, phase 3, randomized trial Total days on therapy: 278 for bortezomib and 280 for dexamethasone Trial halted 1 year early by data monitoring committee due to superiority of bortezomib arm
 Dexamethasone Arm Induction: 40 mg PO Days 1-4, 9-12, q5 wks for 4 cycles Maintenance: 40 mg PO Days 1-4 q4 wks for 5 cycles (n = 336) Richardson P, et al. ASH Abstract APEX: international, phase 3, randomized trial Total days on therapy: 278 for bortezomib and 280 for dexamethasone Trial halted 1 year early by data monitoring committee due to superiority of bortezomib arm.")
45
Bortezomib vs Dexamethasone in Relapsed/Refractory Multiple Myeloma 78% improvement in median time to progression (TTP) with bortezomib Time (days) P =.0001 Proportion of patients 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 306090120150180210240270300330360390420450 Median TTP Bortezomib Dexamethasone Bortezomib Dexamethasone 0 All PtsPts 1 relapse* 6.2 mos 3.5 mos 7.0 mos 5.6 mos Richardson P, et al. ASH 2004. Abstract 336.5. * Patients treated as secondline, after first relapse

46
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Bortezomib vs Dexamethasone in Relapsed/Refractory Multiple Myeloma 41% decreased risk of death with bortezomib P =.005 0306090120150180210240270300330360 Proportion of patients Bortezomib Dexamethasone Time (days) 1-yr survival Bortezomib Dexamethasone All PtsPts 1 relapse* 80% 66% 89% 72% Richardson P, et al. ASH 2004. Abstract 336.5. * Patients treated as secondline, after first relapse

47
MYELOMA: STEM CELL TRANSPLANT

48
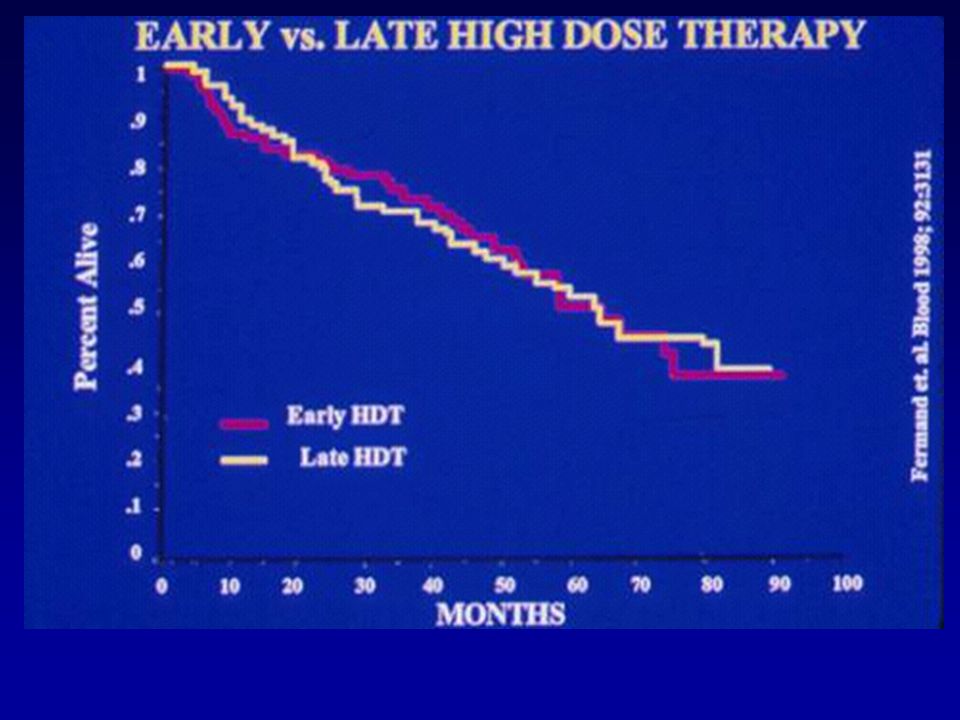
Conventional Dose Chemo vs. Auto Transplant in Multiple Myeloma

50
Tandem Auto Transplant

51
Copyright ©2003 American Society of Hematology. Copyright restrictions may apply. Maloney, D. G. et al. Blood 2003;102:3447-3454 Figure 4. Kaplan-Meier estimates of overall survival and progression-free survival following nonmyeloablative allografts for myeloma Auto then mini Allo

52
BMT Clinical Trials Network Tandem Auto VS Auto then mini-Allo (if have an HLA- identical sibling)
")
Similar presentations



 Idiopathic Associated with other diseases (autoimmune, infectious, non-heme.>")








 Is Highly Active and Offers a Neuropathy Sparing Approach for Proteasome-Inhibitor Based Therapy in Waldenstrom’s.>")
 with Newly Diagnosed Multiple Myeloma (NDMM) Receiving Lenalidomide and Low-Dose Dexamethasone.>")


 Induces High Rates.>")
 for Newly Diagnosed Multiple Myeloma (MM) Patients: Initial Results of a Multicenter, Open Label.>")

