Download presentation
Presentation is loading. Please wait.

1
Development and evolution of chronic lymphocytic leukemia Nicholas Chiorazzi Karches Center for CLL Research The Feinstein Institute for Medical Research North Shore – LIJ Health System Manhasset, NY, USA

2
Major messages 1. CLL develops stepwise over time, requiring accumulation of a series of genetic abnormalities. These abnormalities can complement an inherited predisposition supporting transformation. “Development” 2.Once transformation has occurred, clinical progression often results from secondary changes in protein-coding and non-protein-coding genes. “Evolution” 3.The development of primary and secondary DNA variants is facilitated by signals from the microenvironment. “Promotion” 4.Because genetic testing strategies are defining the predisposing, transforming, and progression factors, the CLL field is moving to a precise definition of patient subsets based on specific genetic changes. This will lead to unique therapies targeting defined abnormalities

3
Major messages – “Development” 1.CLL develops stepwise over time, requiring accumulation of a series of genetic abnormalities. These abnormalities can complement an inherited predisposition supporting transformation A. Evidence for an inherited predisposition to CLL B. Indications of a stepwise progression from a normal B cell to an intermediate stage to full blown CLL C. Possible acquired genetic abnormalities involved in transformation to a CLL cell

4
Evidence supporting an inherited predisposition to CLL 1.Racial associations of CLL Incidence greater in white > black > yellow populations Increased incidence after irradiation exposure Hiroshima/Nagasaki versus Chernobyl experience 2.Familial CLL Highest familial aggregation among leukemias/lymphomas Familial and sporadic CLL are clinically and molecularly similar 3.Occurrence of other cancers in patients and family members of CLL patients Higher relative risk in family members: CLL 8.5x and NHL 1.9x Increased risk in CLL patients of solid tumors, especially epithelial (skin) cancers not explainable solely by prior therapy
 cancers not explainable solely by prior therapy")
5
An inherited predisposition to CLL 4.Genetic studies of CLL patients and families Inheritance of susceptibility is likely polygenic Genome-wide association studies (GWAS) 10 single nucleotide genetic polymorphisms (SNPs) more frequently found in CLL patients LocationGeneOR 2q13BCL2L11/Bim1.39 2q37.1SP1401.41 2q37.3FARP21.39 6q25.3IRF41.54 8q24.21GRAMD1B1.26 11q24.1RFXT and NEDD41.45 15q21.3--1.36 15q23--1.37 16q24.1IRF81.22 19q13.32PRKD21.36 DiBernardo et al. Nat Genet 40: 1204-1210, 2008 Crowther-Swanepoel et al. Nat Genet 42: 132-136, 2010

6
An inherited predisposition to CLL 5. Hematopoietic stem cells (HSCs) from CLL patients appear to differ functionally from most normal adults Y. Kikushige et al. Self-renewing hematopoietic stem cell is the primary target in pathogenesis of human chronic lymphocytic leukemia. Cancer Cell 20: 246-259, 2011
 from CLL patients appear to differ functionally from most normal adults Y. Kikushige et al. Self-renewing hematopoietic stem cell is the primary target in pathogenesis of human chronic lymphocytic leukemia. Cancer Cell 20: ,")
7
An inherited predisposition to CLL Genetic studies of CD34 + CD38 - CLL cells from BM Studies carried out by injecting cells into newborn, alymphoid mice and watching their development and growth over time CD34 + cells from CLL BM gave rise to more immature and mature B cells than CD34 + cells from BM of normal subjects Kikushige et al. Cancer Cell 20: 246, 2011

8
An inherited predisposition to CLL Genetic studies of CD34 + CD38 - CLL cells from BM Both CD5 + and CD5 - B cells developed in the mice but only the CD5 + CD20 + cells were monoclonal Kikushige et al. Cancer Cell 20: 246, 2011

9
An inherited predisposition to CLL Genetic studies of CD34 + CD38 - CLL cells from BM However, the CD5 + clones that developed from CLL HSCs did not carry the IGHV-D-J rearrangement of the CLL cell donor Kikushige et al. Cancer Cell 20: 246, 2011

10
An inherited predisposition to CLL Genetic studies of CD34 + CD38 - CLL cells from BM Furthermore, the CD34 + cells did not exhibit the genomic abnormality of the CLL donor, e.g., del(13q) or del(11q), etc. Lastly, the mature CLL B-cell clones did not evolve into a “clinical CLL-like disease, although there was a suggestion that the IGHV-D-J rearrangements of the “pre-CLL” clones have the characteristics of CLL clones in general, i.e., specific gene family use. Thus, it appears that the CD34 + cells of CLL patients are “primed” to make more B lymphocytes, often of the CD5 subtype that are more likely to be oligo/monoclonal, but presumably environmental influences (e.g., BCR selection) are required to support further transformation. Is this monoclonal B lymphocytosis (MBL)? Kikushige et al. Cancer Cell 20: 246, 2011
 are required to support further transformation. Is this monoclonal B lymphocytosis (MBL). Kikushige et al. Cancer Cell 20: 246,")
11
Question to consider: Are these phenomena the consequences of a somatic lesion occurring in CLL patients or representations of a genetic predisposition/polymorphism inherited in the human germline?

12
Major messages – “Development” 1.CLL develops stepwise over time, requiring accumulation of a series of genetic abnormalities. These abnormalities can complement an inherited predisposition supporting transformation A. Evidence for an inherited predisposition to CLL B. Indications of a stepwise progression from a normal B cell to an intermediate stage to full blown CLL C. Possible acquired genetic abnormalities involved in transformation to a CLL cell

13
Monoclonal B lymphocytosis (MBL) CLL-like MBL Oligo/monoclonal expansion of circulating B cells that are L-chain restricted and express a CLL phenotype Found in ~3-5% of normal individuals and ~20% over the age of 65 years. ~12-15% of first-degree relatives of CLL patients Appears to be a transition from clinical MBL to CLL ~1-2% of clinical MBL patients convert to CLL yearly AC Rawstron et al. N Engl J Med 359: 575-583, 2008 D Rossi et al. Br J Haematol 146: 64-75, 2009 TD Shanafelt et al. J Clin Oncol 27: 3959-3963, 2009 Several immune, genetic, and prognostic parameters differ between clinical MBL and CLL, suggesting a transition from one to the other Tumor burden FISH-defined genomic aberrations Lymphocyte doubling time Rossi et al. Br J Haematol 146: 64–75, 2009

14
Monoclonal B lymphocytosis (MBL) CLL-like MBL Transition from clinical MBL to CLL MBL precedes CLL in the majority of instances O Landgren et al. N Engl J Med 360: 659-667, 2009 M Frezzato et al. Am J Hematol 85: 868-871, 2010 Prospective and retrospective analyses of populations followed for another purpose indicated that almost every person who happened to develop CLL had evidence for a clonal expansion in advance

15
Major messages – “Development” 1.CLL develops stepwise over time, requiring accumulation of a series of genetic abnormalities. These abnormalities can complement an inherited predisposition supporting transformation A. Evidence for an inherited predisposition to CLL B. Indications of a stepwise progression from a normal B cell to an intermediate stage to full blown CLL C. Acquired genetic abnormalities that may be involved in transformation to a CLL cell Deletion of microRNAs 15a and 16-1 Overexpression of microRNAs that function as oncogenes Overexpression/activity of TCL1

16
Key to the 13q deletion: loss of microRNAs 15a and 16-1 Deletion at 13q most common chromosomal abnormality in CLL more common among IGHV mutated CLL cases Calin, Croce, and colleagues determined that the key elements were microRNAs 15a/16.1 15a/16.1 cluster shown to control Bcl2 levels documentation that microRNAs can be tumor suppressors suggestion that loss of this microRNA cluster is a key element in the development of CLL, at least for those that develop M-CLL

17
Klein et al. The DLEU2/miR-15a/16-1 cluster controls B cell proliferation and its deletion leads to chronic lymphocytic leukemia. Cancer Cell 17: 28–40, 2010 Deleted either: only microRNAs 15a/16.1 or microRNAs 15a/16.1 and the DLeu2 gene (minimal deleted region, MDR) Mice can develop over time: CD5 + B-cell disorder of low penetrance: MDR faster and more lethal clones expressing stereotyped BCRs Targeted molecular elimination of microRNAs 15a/16.1 or these plus Leu 2 can lead to a CLL-like disease
 Mice can develop over time: CD5 + B-cell disorder of low penetrance: MDR faster and more lethal clones expressing stereotyped BCRs Targeted molecular elimination of microRNAs 15a/16.1 or these plus Leu 2 can lead to a CLL-like disease.")
18
Klein et al. Cancer Cell 17: 28–40, 2010 Mice with deletion of miR-15a/16-1 or MDR develop lymphoproliferations

19
Summary of “Development” Development of CLL is primed by a series of incompletely defined gene variants This genetic soil is seeded further by other somatic abnormalities acquired later in the life of the transforming B cell The final “hit” in this cascade occurs in a B cell that has rearranged its IGHV, IGHD, and IGHJ genes to yield the signature rearrangement of the clone These composite genetic factors (inherited and acquired) usher a normal B cell into an intermediary stage – “MBL” – and then to full-fledged CLL Candidate acquired factors include loss (or overexpression) of microRNAs, as these can be tumor suppressors or oncogenes
 usher a normal B cell into an intermediary stage – MBL – and then to full-fledged CLL Candidate acquired factors include loss (or overexpression) of microRNAs, as these can be tumor suppressors or oncogenes")
20
Major message – “Evolution” 2. Once transformation has occurred, clinical progression often results from secondary changes in protein- coding and non-protein-coding genes - “evolution” A. Sequential analyses in patients of: FISH abnormalities microRNA abnormalities global DNA abnormalities by comparative genomic hybridization and SNP profiling B. Analyses of DNA abnormalities by next generation sequencing of CLL genomes/exomes

21
Clonal evolution A. Sequential analyses of FISH abnormalities, microRNA abnormalities, and global DNA abnormalities Take home messages: ~25% of patients develop a new genetic abnormality over time in coding or non-coding genes Occurs more frequently in: U-CLL clones and in M-CLL clones of patients that eventually require therapy CD38 + clones ZAP-70 + clones CD49d + clones Most common new lesions: del(13q) del(17p) – harbinger of accelerated disease Greater the number of clonal aberrations the shorter the time to treatment and survival
 del(17p) – harbinger of accelerated disease Greater the number of clonal aberrations the shorter the time to treatment and survival.")
22
Major messages – “Evolution” 2. Once transformation has occurred, clinical progression often results from secondary changes in protein- coding and non-protein-coding genes - “evolution” A. Sequential analyses in patients of: FISH abnormalities microRNA abnormalities global DNA abnormalities by comparative genomic hybridization and SNP profiling B. Analyses of DNA abnormalities by next generation sequencing of CLL genomes/exomes

23
Genetic abnormalities B.Analyses of DNA abnormalities by next generation sequencing of CLL genomes/exomes In 2011, three exciting studies of this type: Puente et al. Nature 475: 101-105, 2011 Fabbri et al. J Exp Med 208: 1389-1401, 2011 Wang et al. N Engl J Med 365: 2497-2506, 2011 Puente et al and Fabbri et al studied untreated patients – combined total 9 patients Wang et al studied treated and untreated patients – total 88 patients Placed under “evolution”, although, because some are found at diagnosis, may be initiating events.

24
Summary of consistent findings B.Analyses of DNA abnormalities by next generation sequencing of CLL genomes/exomes Genomic complexity exists in CLL but is less than that of solid tumors and DLCBL; similar to AML Combined 18 recurrent mutations were identified. Most common abnormality was in NOTCH1 Associations of specific mutations with other known abnormalities in CLL, such as those defined by FISH, suggest links between these Majority of mutations defined could change the structure of the encoded molecule, suggesting clonal selection and therefore functional relevance in patients

25
Associations between specific gene mutations and other characteristics Wang et al. N Engl J Med 365: 2497-2506, 2011

26
Fabbri G. et al. J Exp Med 208: 1389–1401, 2011 NOTCH1 is mutated in a large fraction of Richter’s Syndrome cases and chemorefractory CLL

27
Kaplan-Meier estimates of treatment-free survival and overall survival, according to the mutational status of NOTCH1. Fabbri G. et al. J Exp Med 208: 1389–1401, 2011

28
Summary of “Evolution” ~25% of CLL clones develop new DNA aberrations over time These are more likely to occur in patients with the more ominous prognostic markers However, new DNA aberrations can occur without treatment, suggesting that clonal diversification is occurring continuously The genetic changes that are recurrent among patients presumably indicate pathways that drive CLL progression, if not development Patients that develop new abnormalities often have shorter times to treatment and survival Therefore, halting clonal evolution by targeting specific subsets of cells within CLL clones may be a therapeutic opportunity

29
Major messages – “Promotion” 3. The development of primary and secondary DNA variants is facilitated by signals from the microenvironment Novel DNA lesions occur when cells are duplicating their DNA. Therefore those signals from the microenvironment that promote cell division are most likely to promote DNA variants, e.g., those through the BCR, CD40, TLRs, etc. Simplistically, whatever leads to DNA duplication leads to DNA mistakes. What mechanisms within dividing cells might promote the development of new DNA? Activation-induced deaminase (AID)? Responsible for IGHV mutations and for IG class switch recombination.
. Responsible for IGHV mutations and for IG class switch recombination..")
30
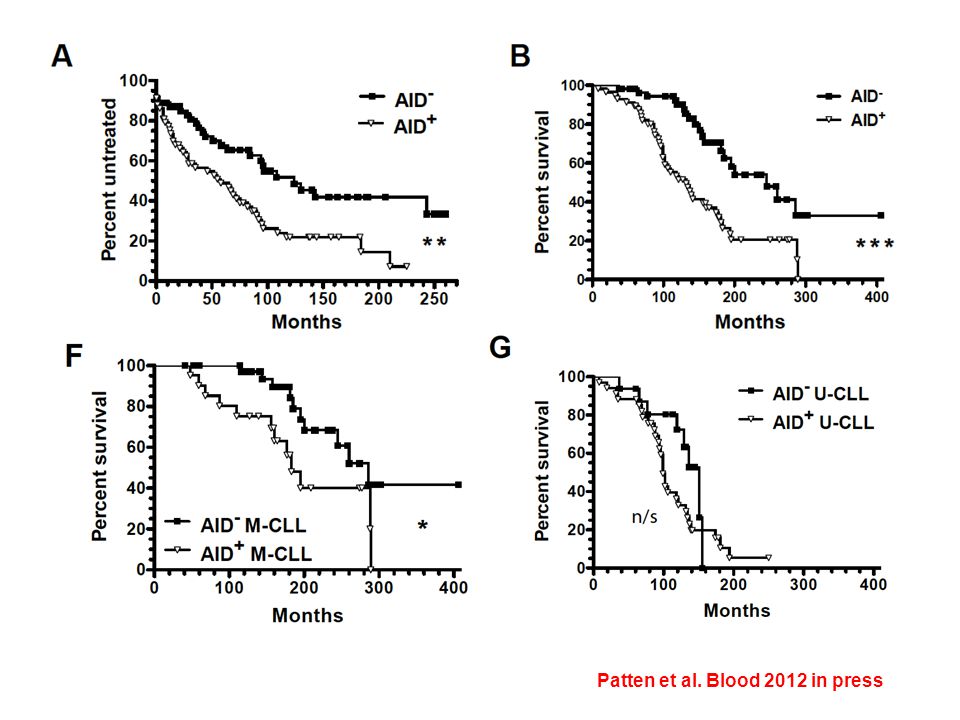
AID is expressed in tissue bound and circulating CLL cells that recently or are dividing Patten et al. Blood 2012 in press

32
Summary of “Promotion” Developing and completely transformed CLL cells owe their fate and ability to evolve to receptor-ligand interactions. Most important appear to be those delivered through the BCR, CD40, and TLRs. Critical are the surroundings within which these signals are delivered – “the microenvironment”. Kinase inhibitors that block stimulatory signals through the BCR and that expel CLL cells from the trophic microenvironment highlight this. Although survival of new cellular variants is essential, the creation of DNA lesions that induce and accelerate clonal growth and progression depends on cell division. Therefore, halting or eliminating dividing cells would block clonal evolution and possibly disease progression

Similar presentations



 gene, one of the most common gene mutations (25%-30%) in AML NPM1 mut co-occurs.>")











. A closer look at the E2A gene... Other names: TCF3, ITF1, and Factors E12/E47 Located on chromosome 19 Encodes.>")



 are a class of small RNA molecules, about ~21 nucleotide (nt) long. MicroRNA are small non coding RNAs (ncRNAs) that regulate.>")