Download presentation
Presentation is loading. Please wait.

1
GASTROESOPHAGEAL REFLUX DISORDER
Mahsa Khodadoostan MD

2
American College of Gastroenterology defines GERD as symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus Physiologic reflux episodes typically occur postprandially, are short-lived, asymptomatic, and rarely occur during sleep Pathologic reflux is associated with symptoms or mucosal injury, often including nocturnal episodes

3
MECHANISMS OF REFLUX Transient lower esophageal sphincter relaxations
Hypotensive lower esophageal sphincter Hiatal hernia and the diaphragmatic sphincter Obesity Pregnancy and exogenous estrogen

4
Transient lower esophageal sphincter relaxations
major differences between tLESRs and swallow-induced LES relaxation: tLESRs occur without an associated pharyngeal contraction are unaccompanied by esophageal peristalsis persist for longer periods (>10 sec) than do swallow-induced LES relaxations
 than do swallow-induced LES relaxations.")
5
Hypotensive lower esophageal sphincter
Strain-induced reflux occurs when a hypotensive LES is overcome and "blown open" by an abrupt increase of intraabdominal pressure. Manometric data suggest that stress reflux is relatively unusual unless the LES pressure is less than 4 mmHg During free reflux a fall in intraesophageal pH occurs without identifiable change in either intragastric or LES pressure. Free reflux is observed only when LES pressure is within 0 to 4 mmHg of intragastric pressure

6
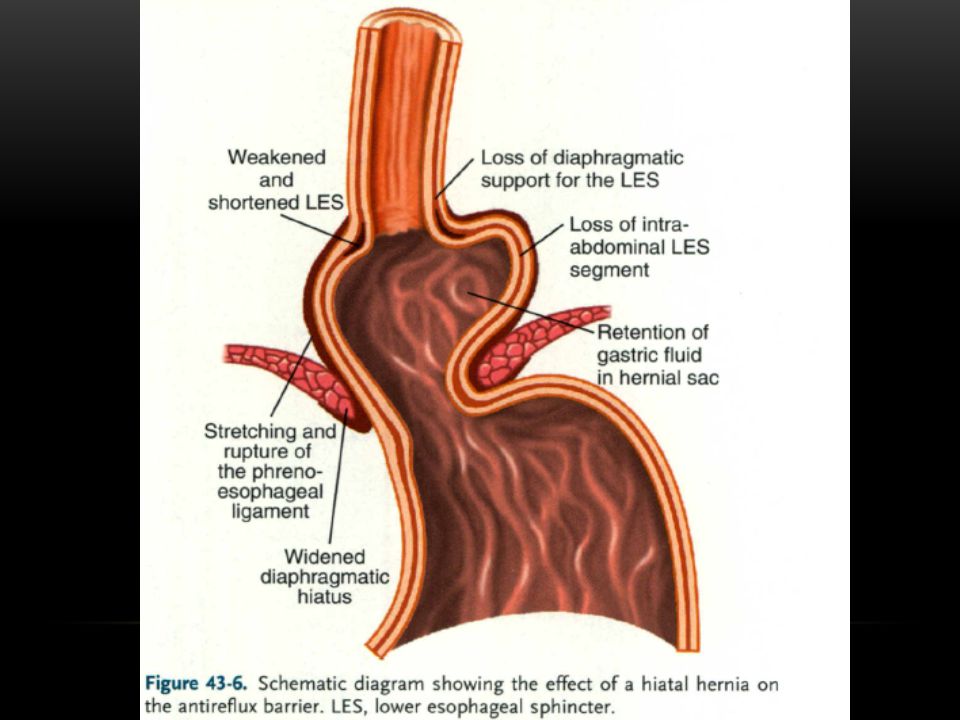
Hiatal hernia and the diaphragmatic sphincter

9
Obesity Obesity is a risk factor for GERD, erosive esophagitis, and esophageal adenocarcinoma

10
Pregnancy and exogenous estrogen
Heartburn occurs in 30 to 50 percent of pregnancies

11
ESOPHAGEAL ACID CLEARANCE
Esophageal emptying in GERD Salivary function in GERD

12
MECHANISMS OF AND DEFENSES AGAINST ESOPHAGEAL INJURY
Epithelial defense Esophageal hypersensitivity

14
CLINICAL MANIFESTATIONS
Heartburn Regurgitation Dysphagia chest pain Water brash or hypersalivation Globus sensation Odynophagia Nausea

15
The patient is a 40 years old man who comes to your office because of heartburn.
His symptoms were initiated since about 2 years ago, heartburn occur weekly No alarm sign Normal physical examination What do you do ?

16
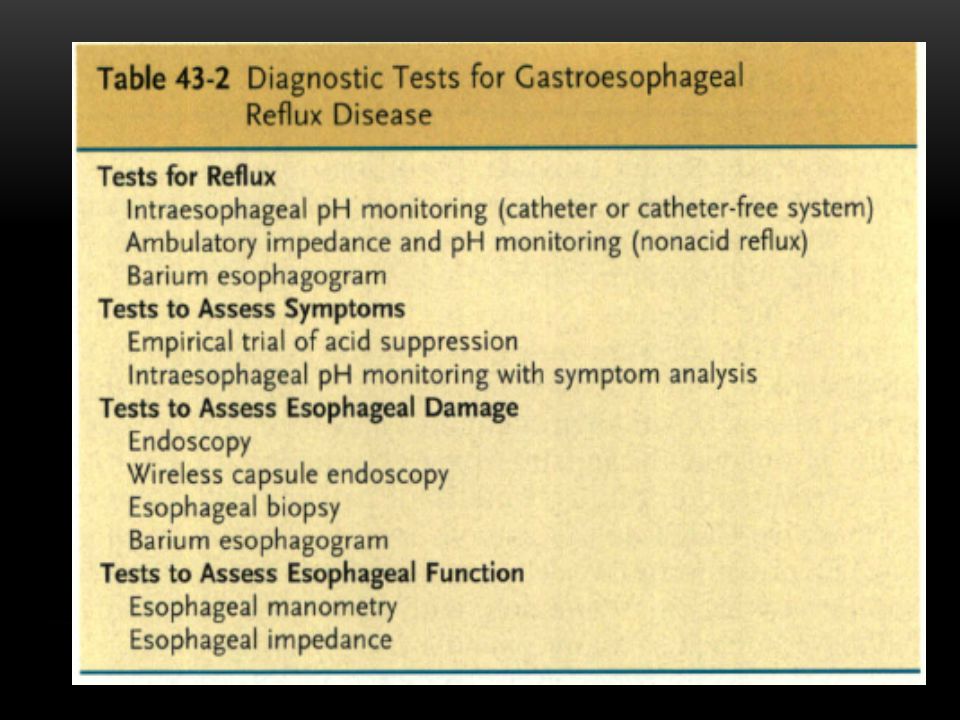
DIAGNOSTIC EVALUATION
It is neither necessary nor practical to initiate a diagnostic evaluation in every patient with heartburn In dysphagia Biopsies should target any areas of suspected metaplasia, dysplasia, or, in the absence of visual abnormalities, normal mucosa (at least five samples to evaluate for eosinophilic esophagitis) Endoscopy should also be done to evaluate patients with a suspected esophageal GERD syndrome who have not responded to an empirical trial of twice daily PPI therapy
 Endoscopy should also be done to evaluate patients with a suspected esophageal GERD syndrome who have not responded to an empirical trial of twice daily PPI therapy.")
17
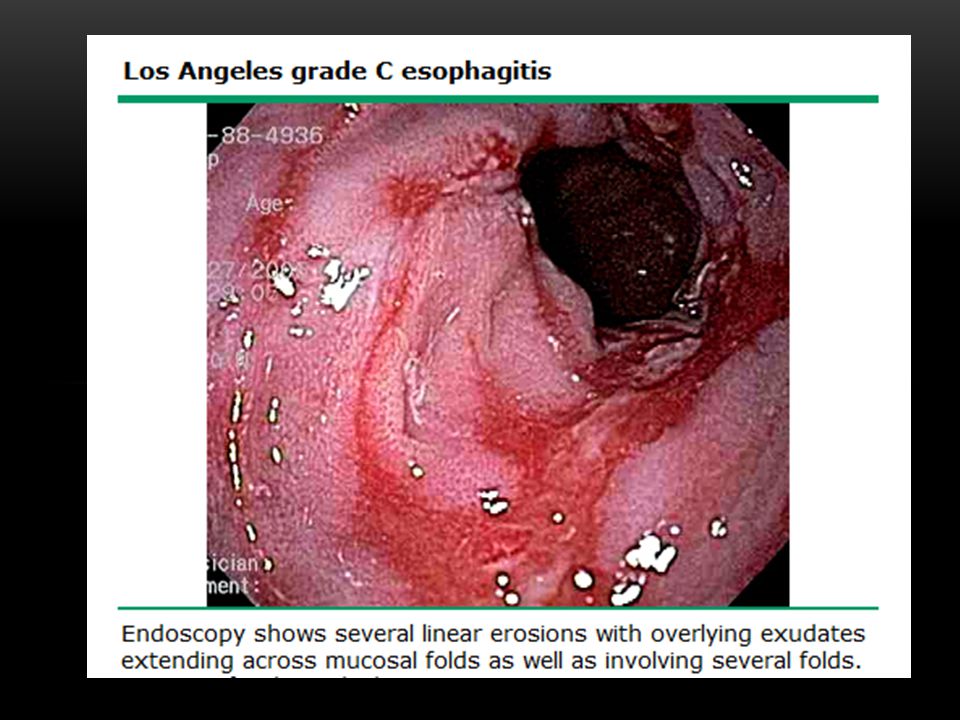
Esophagoscopy Grade A – one or more mucosal breaks each ≤5 mm in length Grade B – at least one mucosal break >5 mm long, but not continuous between the tops of adjacent mucosal folds Grade C – at least one mucosal break that is continuous between the tops of adjacent mucosal folds, but which is not circumferential Grade D – mucosal break that involves at least three-fourths of the luminal circumference

22
Ambulatory esophageal pH monitoring

23
an endoscopy-negative patient being considered for surgical antireflux repair (pH study done after withholding antisecretory drug regimen for ≥ one week). To evaluate patients after antireflux surgery who are suspected to have ongoing abnormal reflux (pH study done after withholding antisecretory drug regimen for ≥ one week). to evaluate patients with either normal or equivocal endoscopic findings and reflux symptoms that are refractory to proton pump inhibitor therapy
. to evaluate patients with either normal or equivocal endoscopic findings and reflux symptoms that are refractory to proton pump inhibitor therapy.")
24
Esophageal pH recording is possibly indicated to detect refractory reflux in patients with chest pain after cardiac evaluation using a symptom reflux association scheme, preferably the symptom association probability calculation (pH study done after a trial of proton pump inhibitor therapy for at least four weeks). Esophageal pH recording is possibly indicated to evaluate a patient with suspected otolaryngologic manifestations (laryngitis, pharyngitis, chronic cough) of gastroesophageal reflux disease after symptoms have failed to respond to at least four weeks of proton pump inhibitor therapy
 of gastroesophageal reflux disease after symptoms have failed to respond to at least four weeks of proton pump inhibitor therapy.")
25
Esophageal pH recording is possibly indicated to document concomitant gastroesophageal reflux disease in an adult onset, nonallergic asthmatic suspected of having reflux-induced asthma (pH study done after withholding antisecretory drugs for ≥ one week). Note: a positive test does not prove causality! Esophageal pH recording is not indicated to detect or verify reflux esophagitis (this is an endoscopic diagnosis). Esophageal pH recording is not indicated to evaluate for "alkaline reflux."
. Esophageal pH recording is not indicated to evaluate for alkaline reflux.")
26
Esophageal manometry for the evaluation of peristaltic function before antireflux surgery to exclude major motor disorders It can also be used to ensure that ambulatory pH probes are placed correctly

27
Bernstein test determine symptom correlation with esophageal acidification in patients without endoscopic evidence of esophagitis The test is done by alternately infusing saline or 0.1N HCl at a rate of 6 to 8 mL/min into the mid-esophagus via a nasogastric tube or manometric assembly A positive test is defined as reproduction of the patient's symptoms with acid perfusion but not with saline. This test is ideal for determining acid sensitivity

28
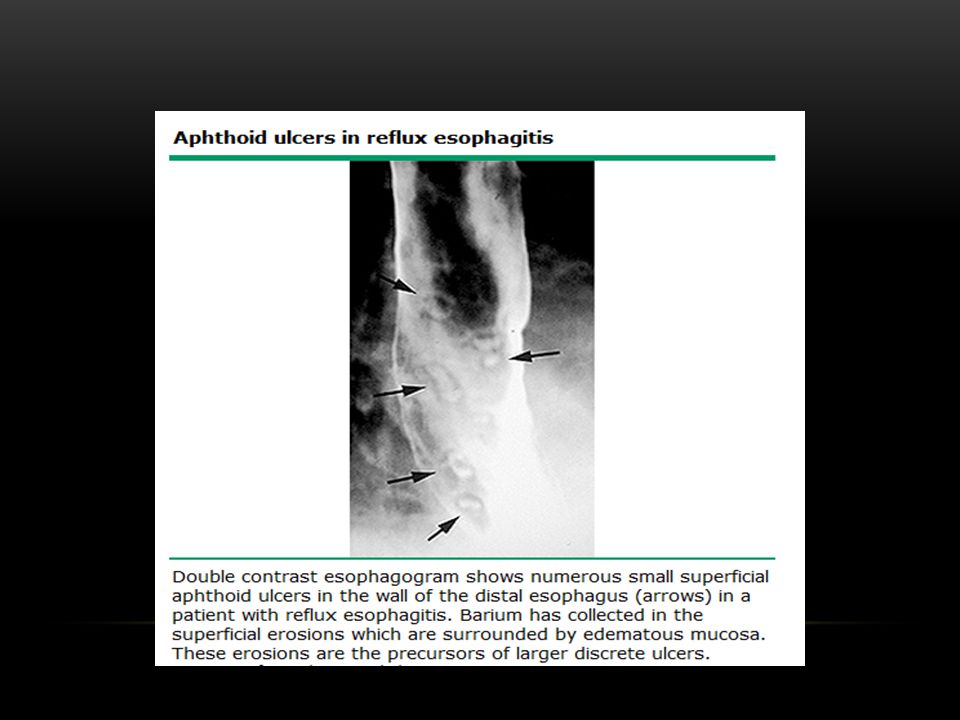
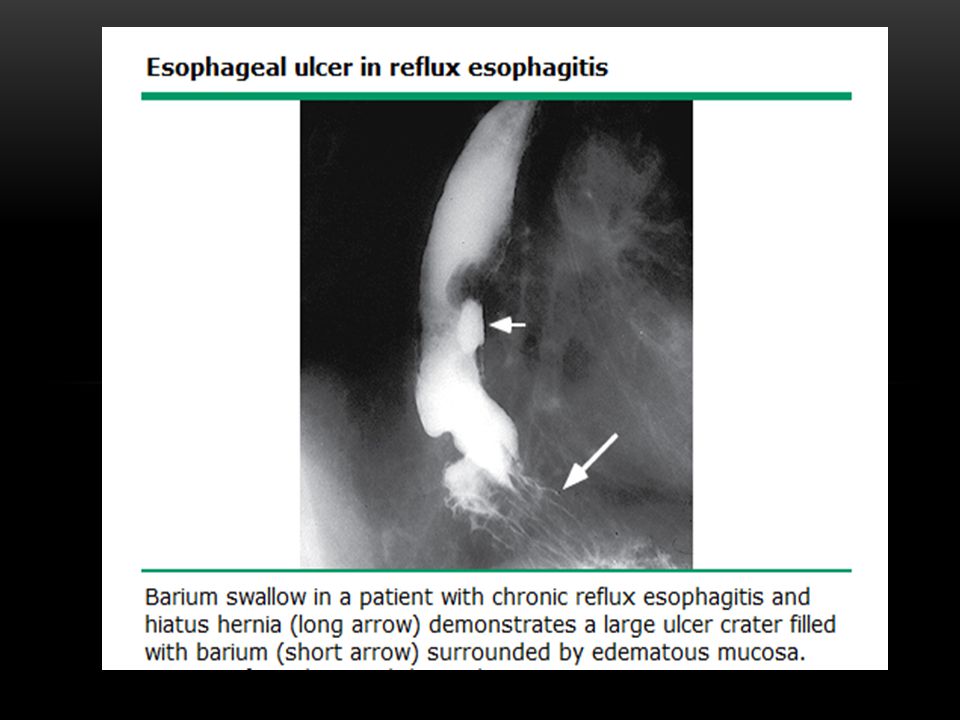
Radiologic techniques

33
treatment?

34
Mild symptomatic GERD :
lifestyle and dietary modifications along with antacids and nonprescription histamine-2 (H2) receptor antagonists Patients with debilitating symptoms usually require more pharmacologically sustained acid-suppressive therapy
 receptor antagonists. Patients with debilitating symptoms usually require more pharmacologically sustained acid-suppressive therapy.")
37
LIFESTYLE MODIFICATIONS

38
LIFESTYLE MODIFICATIONS
Head of bed elevation(important for individuals with nocturnal or laryngeal symptoms ) Dietary modification : a core group of reflux-inducing foods (fatty foods, chocolate, peppermint, and excessive alcohol, which may reduce lower esophageal sphincter pressure) and then to suggest that the patient selectively avoid foods known to cause symptoms Refraining from assuming a supine position after meals and avoidance of meals before bedtime Avoidance of tight fitting garments Wt loss Promotion of salivation by chewing gum Restriction of alcohol use and elimination of smoking
 Dietary modification : a core group of reflux-inducing foods (fatty foods, chocolate, peppermint, and excessive alcohol, which may reduce lower esophageal sphincter pressure) and then to suggest that the patient selectively avoid foods known to cause symptoms. Refraining from assuming a supine position after meals and avoidance of meals before bedtime. Avoidance of tight fitting garments. Wt loss. Promotion of salivation by chewing gum. Restriction of alcohol use and elimination of smoking.")
39
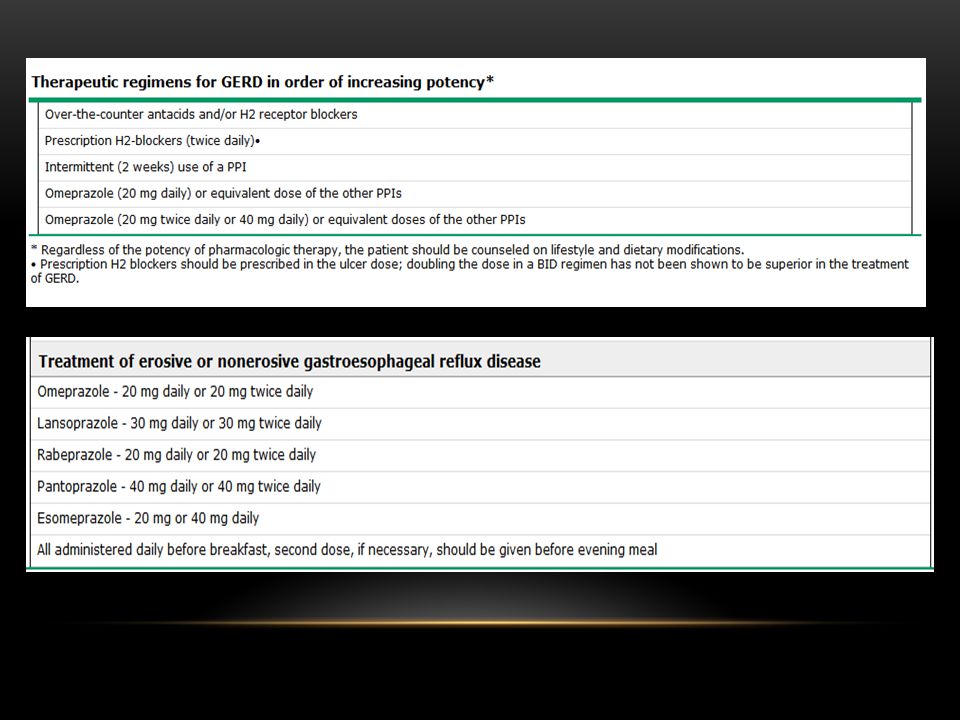
ACID-SUPPRESSIVE MEDICATIONS
H2 receptor antagonists offer a therapeutic gain of 10 to 24 percent relative to the placebo The different H2 receptor antagonist have equivalent efficacy if drug dose is adjusted for potency An increased dose or prolonged course of an H2 antagonist is unlikely to produce relief for patients who continue to have heartburn after six weeks of treatment with a standard dose of an H2 antagonist The proton pump inhibitors are more effective in healing esophagitis than the H2 receptor antagonists, with a therapeutic gain of 57 to 74 percent relative to placebo proton pump inhibitors lead to more rapid healing and symptom relief than H2 receptor antagonists

40
Nonerosive gastroesophageal reflux disease
patients with typical symptoms of GERD do not have esophagitis hypersensitivity to physiologic degrees of acid reflux patients have abnormal acid exposure but have not developed overt mucosal injury others have heartburn not attributable to acid reflux, sometimes referred to as "functional heartburn“ The first two groups, but not the third group of patients, may respond to antisecretory therapy

41
ADJUNCTIVE THERAPY Prokinetic agents Reflux inhibitors
TREATMENT OF HELICOBACTER PYLORI INFECTION

44
UNDERLYING MECHANISMS OF PPI FAILURE

45
Esophageal hypersensitivity and functional heartburn
Proper dosing Compliance Nocturnal acid breakthrough? Reduced bioavailability Differences in metabolism Helicobacter pylori status Drug resistance Delayed healing Weakly acidic or alkaline reflux Residual acid reflux Bile acid reflux Psychological comorbidity

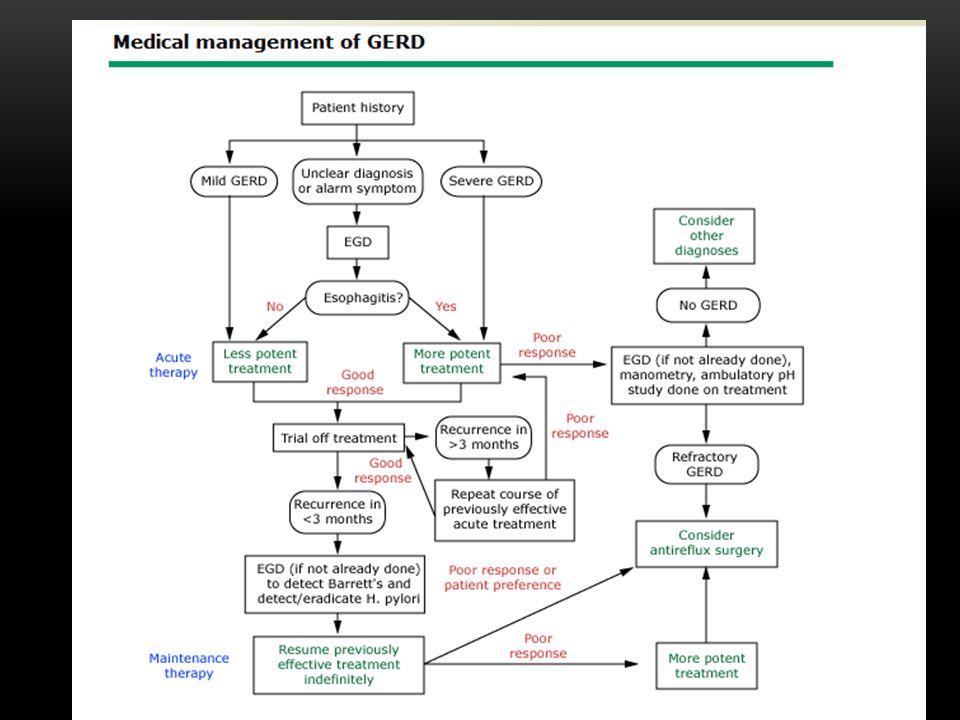
46
MANAGEMENT Optimizing therapy Upper endoscopy Esophageal pH testing
Esophageal manometry Lifestyle modifications Treatment of residual acid reflux : Changing PPIs versus doubling the dose Bedtime H2 receptor antagonist Treatments aimed at reducing reflux Treatment of esophageal hypersensitivity Treatment of delayed gastric emptying Fundoplication

51
efficacy of lifestyle modifications for GERD?

52
Grade B: I. Weight loss should be advised for overweight or obese patients with esophageal GERD syndromes. II. Elevation of the head of the bed for selected patients who are troubled with heartburn or regurgitation when recumbent. Grade Insuff: I. Broadly advocating lifestyle changes for all (as opposed to selected) patients with GERD.
 patients with GERD.")
53
How do antisecretory therapies compare in efficacy and under what circumstances might one be preferable to another?

54
Grade A: I. proton pump inhibitors (PPIs) are more effective than histamine2 receptor antagonists (H2RAs), which are more effective than placebo. Grade B: I. Twice-daily PPI therapy for patients with an esophageal syndrome with an inadequate symptom response to once-daily PPI therapy. II. A short course or as-needed use of antisecretory drugs in patients with a symptomatic esophageal syndrome without esophagitis when symptom control is the primary objective. For a short course of therapy, PPIs are more effective than H2RAs, which are more effective than placebo. Grade D: I. Metoclopramide as monotherapy or adjunctive therapy in patients with esophageal or suspected extraesophageal GERD syndromes.

55
What is the role and priority of diagnostic tests in the evaluation of patients with suspected esophageal GERD syndromes?

56
Grade B: I. Endoscopy with biopsy for patients with an esophageal GERD syndrome with troublesome dysphagia. II. Endoscopy to evaluate patients with a suspected esophageal GERD syndrome who have not responded to an empirical trial of twice-daily PPI therapy

57
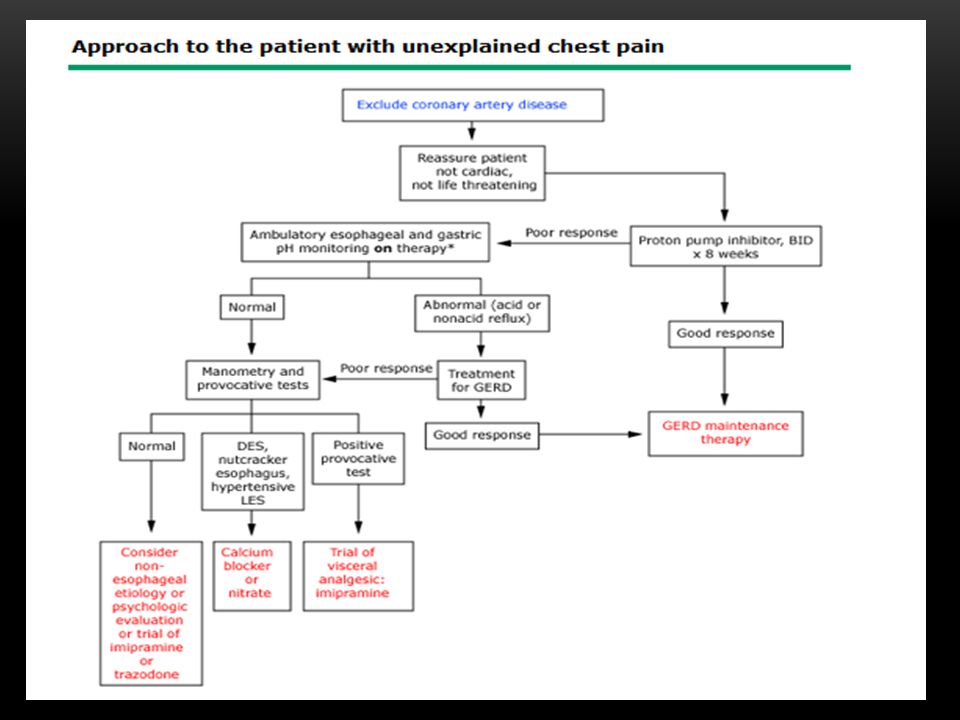
What are the unique management considerations in patients with suspected reflux chest pain syndrome?
Grade A: I. Twice-daily PPI therapy as an empirical trial for patients with suspected reflux chest pain syndrome after a cardiac etiology has been carefully considered.

58
What is the best initial management for patients with suspected extraesophageal reflux syNDROM?
Grade B: I. Acute or maintenance therapy with once- or twice-daily PPIs (or H2RAs) for patients with a suspected extraesophageal GERD syndrome (laryngitis, asthma) with a concomitant esophageal GERD syndrome. Grade D: I. Once- or twice-daily PPIs (or H2RAs) for acute treatment of patients with potential extraesophageal GERD syndromes (laryngitis, asthma) in the absence of a concomitant esophageal GERD syndrome. Grade Insuff: I. Once- or twice-daily PPIs for patients with suspected reflux cough syndrome.
 for patients with a suspected extraesophageal GERD syndrome (laryngitis, asthma) with a concomitant esophageal GERD syndrome. Grade D: I. Once- or twice-daily PPIs (or H2RAs) for acute treatment of patients with potential extraesophageal GERD syndromes (laryngitis, asthma) in the absence of a concomitant esophageal GERD syndrome. Grade Insuff: I. Once- or twice-daily PPIs for patients with suspected reflux cough syndrome.")
59
Does GERD progress in severity?
Grade D: I. Routine endoscopy in subjects with erosive or nonerosive reflux disease to assess for disease progression.

60
What maintenance therapy is indicated for patients with the typical esophageal reflux syndrome?
Grade A: I. Long-term use of PPIs for the treatment of patients with esophagitis once they have proven clinically effective. Long-term therapy should be titrated down to the lowest effective dose based on symptom control. Grade D: I. Less than daily dosing of PPI therapy as maintenance therapy in patients with an esophageal syndrome who previously had erosive esophagitis.

61
What maintenance therapy is indicated for patients with suspected extraesophageal reflux syndromes?
Grade B: I. Acute or maintenance therapy with once- or twice-daily PPIs (or H2RAs) for patients with a suspected extraesophageal GERD syndrome (laryngitis, asthma) with a concomitant esophageal GERD syndrome. Grade Insuff: I. Maintenance therapy with once- or twice-daily PPIs (or H2RAs) for patients with potential extraesophageal GERD syndromes (laryngitis, asthma) in the absence of a concomitant esophageal GERD syndrome. II. Once- or twice-daily PPIs for patients with suspected reflux cough syndrome.
 for patients with a suspected extraesophageal GERD syndrome (laryngitis, asthma) with a concomitant esophageal GERD syndrome. Grade Insuff: I. Maintenance therapy with once- or twice-daily PPIs (or H2RAs) for patients with potential extraesophageal GERD syndromes (laryngitis, asthma) in the absence of a concomitant esophageal GERD syndrome. II. Once- or twice-daily PPIs for patients with suspected reflux cough syndrome.")
62
What are the clinical consequences of chronic potent acid inhibition?
Grade Insuff: I. Advocating bone density studies, calcium supplementation, H pylori screening, or any other routine precaution because of PPI use

63
What is the role of endoscopy in long-term management of patients with GERD?
Grade B: I. Endoscopy with biopsy for patients with an esophageal GERD syndrome with troublesome dysphagia. Grade Insuff: I. Routine upper endoscopy in the setting of chronic GERD symptoms to diminish the risk of death from esophageal cancer. II. Endoscopic screening for Barrett's esophagus and dysplasia in adults 50 years or older with >5-10 years of heartburn to reduce mortality from esophageal adenocarcinoma.

64
What are indications for antireflux surgery, and what is the efficacy of this therapy?
Grade A: I. When antireflux surgery and PPI therapy are judged to offer similar efficacy in a patient with an esophageal GERD syndrome, PPI therapy should be recommended as initial therapy because of superior safety. II. When a patient with an esophageal GERD syndrome is responsive to, but intolerant of, acid suppressive therapy, antireflux surgery should be recommended as an alternative. Grade B: I. Antireflux surgery for patients with an esophageal GERD syndrome with persistent troublesome symptoms, especially troublesome regurgitation, despite PPI therapy.

65
Grade C: I. Patients with an extraesophageal GERD syndrome with persistent troublesome symptoms despite PPI therapy should be considered for antireflux surgery Grade D: I. Antireflux surgery for patients with an esophageal syndrome with or without tissue damage who are symptomatically well controlled on medical therapy. II. Antireflux surgery as an antineoplastic measure in patients with Barrett's metaplasia

66
Patient is a 45 y/o man who comes to your office because of chest pain
His chest pain is retrosternal , radiates to neck ,has no association with exercise ,antiacid relifes the pain

68
complications Esophagitis, which can be associated with a variety of symptoms, including heartburn, regurgitation, and dysphagia Consequences of the reparative process of esophagitis (peptic stricture and Barrett's metaplasia) Extraesophageal manifestations of reflux, such as asthma, laryngitis, and cough
 Extraesophageal manifestations of reflux, such as asthma, laryngitis, and cough.")
69
Barrett's esophagus is the condition in which an abnormal columnar epithelium that is predisposed to malignancy replaces the stratified squamous epithelium that normally lines the distal esophagus.! The columnar-lined esophagus causes no symptoms, and the condition has clinical importance only because it is a risk factor for esophageal adenocarcinoma

70
MANAGEMENT TREATMENT OF GASTROESOPHAGEAL REFLUX DISEASE
is very similar to that recommended for patients who have GERD without Barrett's esophagus initial and maintenance therapy with a proton pump inhibitor (PPI) for patients with Barrett's esophagus, irrespective of symptoms and signs of esophagitis antireflux surgery should not be performed solely for cancer prevention in patients with Barrett's esophagus
 for patients with Barrett s esophagus, irrespective of symptoms and signs of esophagitis. antireflux surgery should not be performed solely for cancer prevention in patients with Barrett s esophagus.")
71
AGA RECOMMENDATIONS Screening for Barrett's esophagus is suggested in patients with multiple risk factors associated with esophageal adenocarcinoma (age 50 years or older, male sex, white race, chronic GERD, hiatal hernia, elevated body mass index, or intra- abdominal distribution of body fat) The AGA recommends against screening the general population with GERD for Barrett's esophagus
 The AGA recommends against screening the general population with GERD for Barrett s esophagus.")
72
For patients with Barrett's esophagus, GERD therapy with medication effective to treat GERD symptoms and to heal reflux esophagitis is clearly indicated, as it is for patients without Barrett's esophagus The diagnosis of dysplasia in Barrett's esophagus should be confirmed by at least one additional pathologist, preferably one who is an expert in esophageal histopathology

73
Endoscopic surveillance is suggested for patients with Barrett's esophagus using the following surveillance intervals: No dysplasia: 3 to 5 years Low-grade dysplasia: 6 to 12 months High-grade dysplasia in the absence of eradication therapy: 3 months The AGA recommends against the use of molecular biomarkers to confirm the histologic diagnosis of dysplasia or as a method of risk stratification for patients with Barrett's esophagus

74
Evidence to support the use of acid-reducing agents, specifically PPIs, in patients with Barrett's esophagus solely to reduce the risk of progression to dysplasia or cancer is indirect and has not been proven in a long-term controlled trial

75
For patients with Barrett's esophagus who are undergoing surveillance, the AGA recommends:
Endoscopic evaluation using white light endoscopy Four-quadrant biopsy specimens be taken every 2 cm Specific biopsy specimens of any mucosal irregularities be submitted separately to the pathologist Four-quadrant biopsy specimens be obtained every 1 cm in patients with known or suspected dysplasia

76
The AGA suggests against requiring chromoendoscopy or advanced imaging techniques for the routine surveillance of patients with Barrett's esophagus The AGA recommends against attempts to eliminate esophageal acid exposure for the prevention of esophageal adenocarcinoma. Such attempts include proton pump inhibitor (PPI) administration in doses greater than once daily, esophageal pH monitoring to titrate PPI dosing, and antireflux surgery
 administration in doses greater than once daily, esophageal pH monitoring to titrate PPI dosing, and antireflux surgery.")
77
The AGA suggests against the use of aspirin solely to prevent esophageal adenocarcinoma in the absence of other indications. However, it recommends screening patients to identify cardiovascular risk factors for which aspirin therapy is indicated

78
Endoscopic eradication therapy with radiofrequency ablation, photodynamic therapy, or endoscopic mucosal resection (EMR) rather than surveillance is recommended for treatment of patients with confirmed high-grade dysplasia within Barrett's esophagus EMR is recommended for patients who have dysplasia in Barrett's esophagus associated with a visible mucosal irregularity to determine the T stage of the neoplasia

79
PEPTIC STRICTURE

82
Treatment of strictures
conservative management of benign strictures by dilation surgery

83
COMPLICATIONS OF EXTRAESOPHAGEAL REFLUX
Asthma posterior laryngitis chronic cough dental erosions chronic sinusitis recurrent pneumonitis nocturnal choking chronic hoarseness Pharyngitis subglottic stenosis laryngeal cancer

84
Reflux-induced asthma
Two major mechanisms of reflux-induced asthma have been proposed: Aspiration of gastric contents into the lung with consequent bronchospasm Reflux-induced activation of a vago-vagal reflex arc from the esophagus to the lung causing bronchoconstriction

85
Otolaryngologic manifestations
Laryngitis Laryngeal and tracheal stenosis Laryngeal cancer

86
THE END

Similar presentations














 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")






 Rory Loveland Paramedic class ’08-’09.>")




>")





