Download presentation
Presentation is loading. Please wait.

1
EnableNSW September 2009 Insights into the Artificial Limb Service

2
Recent activities at the ALS

3
Rigid Dressings project Continued encouragement of the implementation of the Rigid Dressing application for new TTAs Instructional DVD produced –Being used as incentive to attend practical training –Plan to make available via website and You Tube by end of the year Written resources produced and available from EnableNSW website

4
Rigid Dressings project Training offered to all metropolitan AHS Accepted by 3 AHS, declined by 1 Completed in 1 AHS Planning continues in other 2 AHS

5
Amputee Volunteer Peer Support Program Developed and published a training manual Used for “train the trainer” courses for people leading training in peer support volunteering Training being conducted by the Amputee Association

6
Component additions Components recently added: –Seattle Kinetic Foot –Otto Bock 3R106 variable cadence knee –Otto Bock 3R41 safety knee

7
Fact Sheets Fact sheets for amputees have been created on the following topics: –Caring for your residual and intact limb –How to avoid a fall after your amputation –Managing Pain –How to obtain your artificial limb –Driving after amputation –Caring for your prosthetic upper limb –Caring for your prosthetic lower limb Translated into six languages most commonly spoken in NSW Download from the EnableNSW website or by phoning 1800 362 253

8
Promoting NSW to prosthetists Liaising with LaTrobe University regarding ways to bring Prosthetic graduates to NSW Sponsoring bursaries to assist with accommodation costs for 4 th year students

9
Some Questions Answered

10
RRDs Who is fitting them? –Varies across the state –Of the 19 hospitals that avg >5 amps/yr: –31.6%using RRDs or RDs –10.5%trialling RRDs –10.5%unknown Why aren’t some centres fitting RRDs? –Depends a lot upon the surgeon’s preference –Some see them as a potential hazard for wound healing What is the timeframe to fit RRDs? –Recommended within 0-48hrs of surgery

11
Interim Prostheses A tender for services will be released soon Tender covers metropolitan AHSs Interim = <12 weeks since amputation, predicting 3 months of volume fluctuation, prosthesis must be fit within 3 days of cast taken, client is generally an inpatient at casting/initial fitting Definitive = >12 weeks since amputation, assumption that volume managed and stable by this time, client is generally an outpatient at prescription stage

12
Interim Prostheses Interims in rural areas are not funded currently (exception Rankin Park) due to high variance in level of service provision PD 2008_015-Amputee Care Standards in NSW 6.2 A mechanical interim prosthesis manufactured by a prosthetist is to be made available to all amputees assessed as suitable for prosthetic rehabilitation. This is not required for amputees who are only suitable for a cosmetic prosthesis. Funding of interim prostheses is the responsibility of the acute facility

13
Interim Prostheses Turnaround times –Interim script sent to ALS – approved and sent back within 24hrs –Expectation that prosthetists will cast and fit prosthesis within 3 days

14
Interim Prosthesis Adjustments Some prosthetists allow physiotherapists to independently adjust the alignment on the prosthesis This is an individual agreement between the prosthetist and physiotherapist From a TGA perspective, if you make adjustments to a prosthesis then you make yourself the manufacturer of that prosthesis and subject to the same legislation as prosthetists. This involves a lot of work to comply with the essential principles of TGA

15
Interim Prosthesis Adjustments The Rural Alignment Working Party has not met since April as the ALS is still waiting on a response from the NSW Health legal branch regarding the implications of this practice The need to define the service provision goals of interim services in rural areas will require more work This will be investigated following the implementation of the interim tender in metropolitan Sydney

16
Interim Prosthesis Adjustments The ALS does not currently have any plans to: –introduce accreditation of physiotherapists –Develop training in prosthetic fitting and adjustment/alignment

17
Interim Prosthesis- covers Interim prostheses are supplied without covers to enable ease of adjustment while gait training commences When a cover is required for the definitive socket the patient may –Arrange an appt with the prosthetic manufacturer that it may be completed ‘while they wait’ or be posted back to them –Arrange for use of a wheelchair/frame/crutches while the cover is being made –Make alternate arrangements for care while the cover is being made –All clients should have an alternative mobility aid in case their prosthesis cannot be worn

18
Interim Prostheses for the unlikely user Where available, interims are offered to all potential prosthetic users This is a team decision- not an ALS decision If your amputee team think it is unlikely that the patient will be a long term prosthetic user but feels that they deserve a chance to prove them wrong, then they can prescribe an interim prosthesis Your combined skills in the amp team allow you to accurately predict the patient’s potential K-level and corresponding components they will require 6mths down the track

19
Shrinkers Shrinker socks are considered acute management of oedema and are therefore the funding responsibility of the patient or treating facility Long-term use of shrinker socks indicate an underlying volume issue that needs medical attention Even if considered for long-term use due to lymphoedema and therefore eligible for PADP, they are a low-cost item (<$100) and would not be funded.
 and would not be funded.")
20
Silicone/Gel interface systems Silicone/gel suspension systems funded when clinical need is justified –Inability to suspend using conventional methods, eg. Significant adherent scarring, ileostomy bag, obese patient –Evidence provided that conventional methods have been trialled or considered –Safety issues relating to work ALS funds up to $550 TT liner, $700 TF liner, $330 locking system

21
Components Component lists are provided to Manufacturers and updated twice a year There are 3592 entries on this list, they are not all rated according to K-level as this is not always possible (eg. Valves, etc) Feet and Knees are rated according to K-level Decisions regarding specific component choice is made by the team with direction from the prosthetist The best way to become familiar is to visit a prosthetist’s facility and go through some common components with them
 Feet and Knees are rated according to K-level Decisions regarding specific component choice is made by the team with direction from the prosthetist The best way to become familiar is to visit a prosthetist’s facility and go through some common components with them.")
22
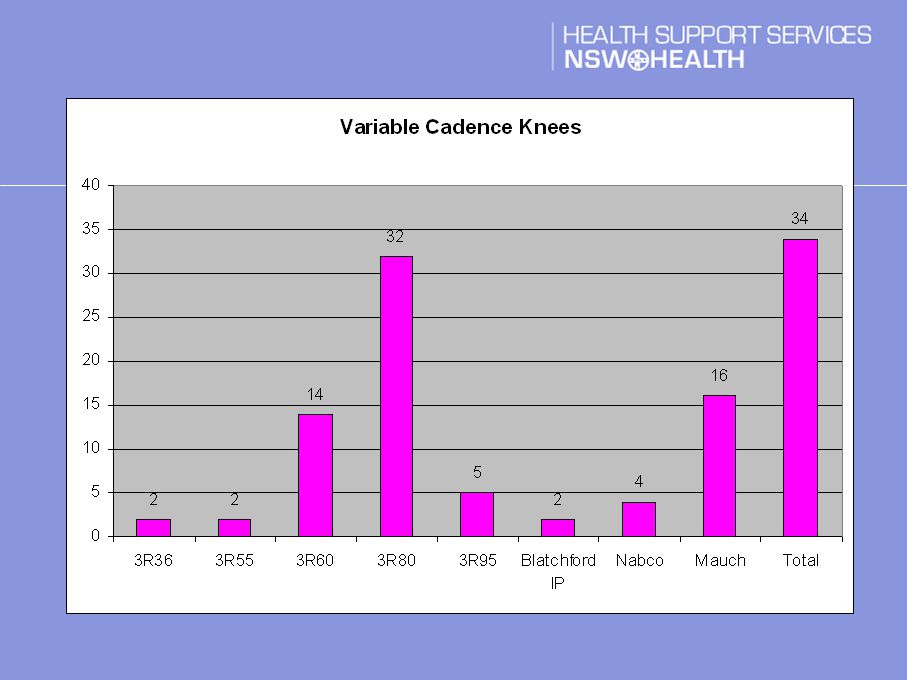
Components

23
Variable cadence knee trial Fitted 111 variable cadence knee joints at a cost of approx $450K Response rate for return of outcome forms has been variable Preference for most common knees – see graph Trial extended for now- possible limitation if outcome forms not returned, or reduction in number of knees available

25
Lack of prescribers Some areas are experiencing an absence of accredited prescribers Options accredited locum attend nearest clinic

26
Questions? Further information: www.enable.health.nsw.gov.au Ph. 1800 362 253

Similar presentations