Download presentation
Presentation is loading. Please wait.

1
Sam Powdrill University of Kentucky Previously at Tenwek Hospital, Kenya Eye care in the Tropics for Non- ophthalmologists

2
Tenwek Hospital

3
Objectives 1.Define blindness from a community perspective 2.Understand the burden of avoidable blindness in our world 3.Exposure to the most common causes of visual impairment and World blindness 4.Gain an understanding of current prevention of blindness efforts and methods

4
50 million blind in our world 600 people go blind every hour Half of these are blind from cataract 90% live in the developing world

5
80% of developing world blindness is avoidable 60% Treatable 20 % Preventable

6
Many in Kenya are Blind Out of 100 people 1 is blind in both eyes 3 more have significant loss of vision 2 of these could see again with surgery

7
So, How can you make a difference?

8
Start with a community assessment. How big is the problem?

9
Causes of World Blindess In millions Cataract 25 Trachoma 7 Glaucoma 5 Refractive errors 5 Diabetes 2.5 Vit A def 1 Macular deg. 1 Oncho 0.5 Injuries 0.5 Leprosy 0.25 Retinal 5 Trachoma

10
Eye Care 1 in 1000 blind 1 in 100 blind another 1% severely visually impaired United States Africa 1 eye doctor for 20,000 people 5800 cataracts done per 1 million people 1 eye doctor for 1million people 300 cataracts done per 1 million people

11
Size of the problem in the local community Immediate catchment of approximately 1,000,000 people 1% blind 1% severely visually impaired Half of these are from cataract Estimated 2000 new cases for cataract surgery annually One eye surgeon

12
Profile of Blindness in Western Kenya

13
Estimated Profile of Blindness in Maasai and Pokot areas Corneal causes are increased by trachoma

14
Pokot Kipsigis Maasai kisii Tenwek Hospital

15
The main eye care provider for 1 million rural people 9, 000 cataract operations needing to be done now 800 new cataract cases per year Only one eye surgeon on staff

16
Patient Profile Culture –Language – always pre- arrange reliable translators. Education – illiterate doesn’t mean stupid! Perception and expectations – How does the patient perceive the problem Local co-morbid considerations and risks Financial priorities of the family – is cataract surgery more important than school fees Follow up – is follow up likely or possible Seasonal considerations – planting, harvesting, rains

18
Screening for cataract surgery at an outlying center

19
Here the gift of sight is a privilege that many do not have

22
Portable Scanoptics microscope

24
Most cataracts are very dense and phaco is both difficult and costly on these lenses.

25
Frown incision allows for a suture-less extracapsular procedure to to remove the nucleus through a wide tunnel

26
Linear capsulotomy with 26 ga needle. Continuous capsulorhexis if adequate visibility

27
Nucleus delivered by hydrodissection

28
Lens in place after completion of capsulorhexis wound closed and tight without suture

29
Anterior Chamber Lens implant Aphakia Posterior capsule complications

30
old glasses

31
new glasses

32
Optical workshop

33
Anterior lens placed under visco-elastic through a clear corneal temporal incision The patient had previous intracapsular surgery without an intraocular lens

34
Large numbers of people are blind from cataract Many do not come because of: Availability Bad outcomes Cost Distance Escort Fear

35
Service to Patient Available Acceptable Appropriate Affordable Alma Atta – health for all by 2000

36
Mobile Surgery Taking eye surgery to a community that does not have a functioning static service within reach of the local people

37
Considerations in Mobile surgery Patient Profile Personnel Physical factors Procedure Price

38
Personnel A local person health provider doing screening ahead of time Translators Patient attendants Mid level eye care provider - screening Equipment person / circulator Scrub technician Surgeon

39
Physical challenges Transport – patients and surgery team Local Facility – cleanliness, water, food, power source Instrument maintenance and care

41
tonometry on a church bench

50
LOKORI

54
Loupes are used for cataract surgery to reduce equipment weight

56
This man has just had his bandage removed and is seeing his hand clearly after being blind for several years

57
Thrilled to see again and dancing This blind lady walked for five days through the bush to get cataract surgery

59
Which is better ? One or two

60
Trachoma

62
Trachoma folicles with inflammation

63
Trachoma inflammation and scar

64
Blind eye from entopion and corneal scarring

65
Epidemiological assessment of Trachoma (EAT) 20% of children 1 – 5 years old have either trachoma TF or TI 1 adult in 100 has trachoma trichiasis If either of these is true then the community has endemic trachoma
 20% of children 1 – 5 years old have either trachoma TF or TI 1 adult in 100 has trachoma trichiasis If either of these is true then the community has endemic trachoma")
66
Community 1 TF or TI 45% of 1-5 year old children Examined 200 adults and found one with TT Community with endemic trachoma which is new to the area.

67
Community 2 TF or TI 5% of 1-5 year old children Examined 100 adults and found 4 with TT Community with endemic trachoma which is diminishing.

68
Community 3 TF or TI 45% of 1-5 year old children Examined 100 adults and found three with TT Community with endemic trachoma which is unchecked and longstanding.

69
Treatment Active disease - tetracycline eye ointment b.I.d X 6 weeks OR Azithromycin one tablet stat Trichiasis – tarsal plate rotation surgery

70
Prevention Daily face washing No livestock in or near the living area Improved pit latrines Efficient use of water Smaller familes with less crowding Education

71
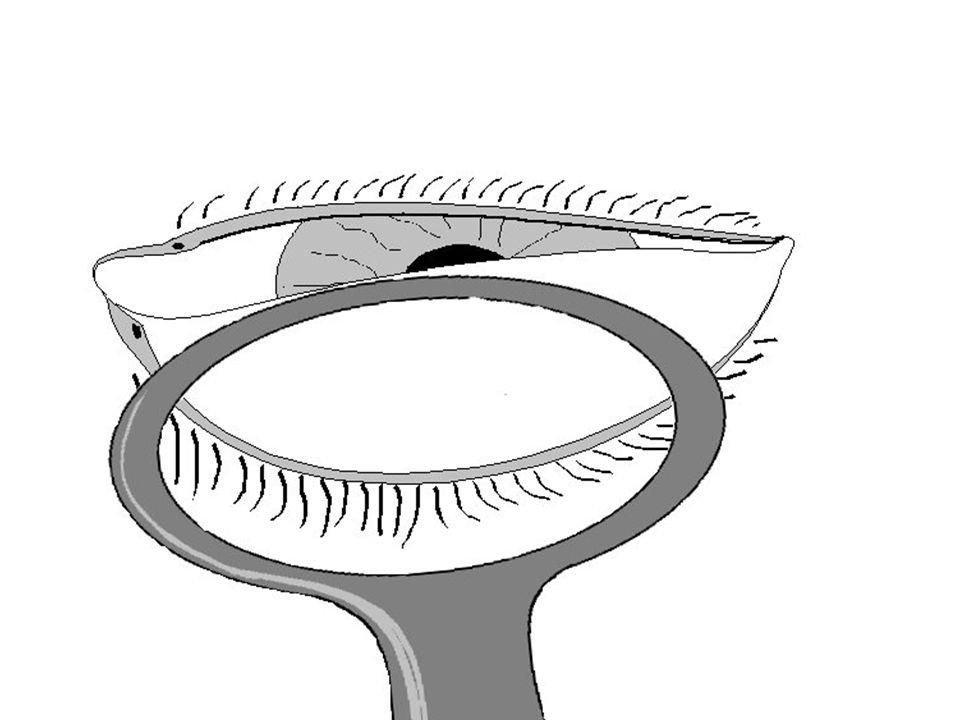
Eye Lid surgery

72
screening

73
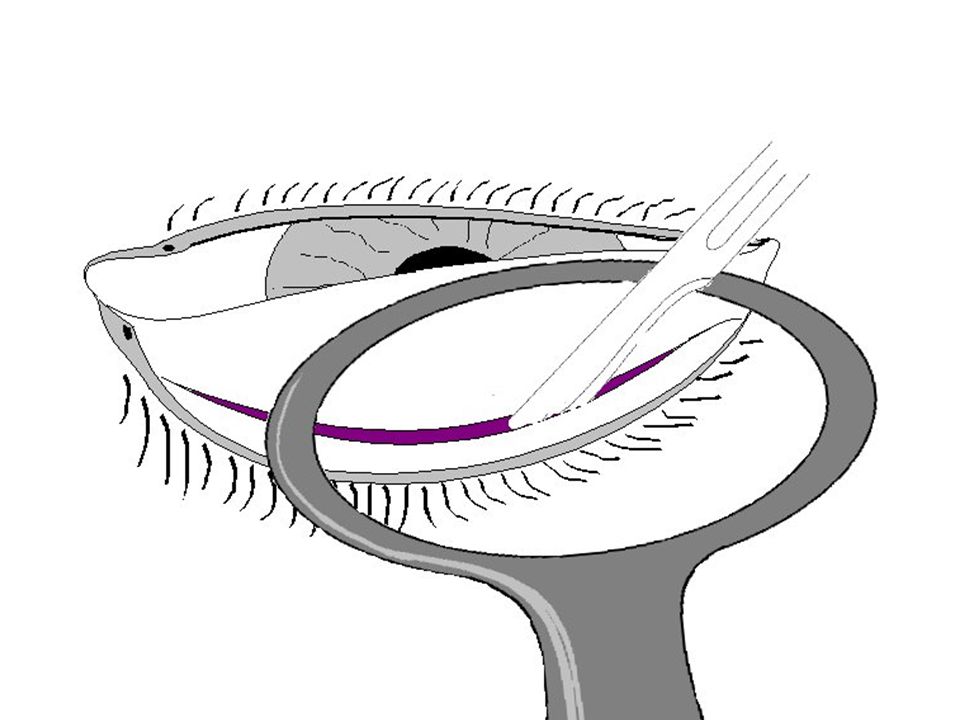
Upper eyelid entropion surgery for trachoma

76
Eye lid incision

79
Undermining and advancement of tarsus

80
6-0 vicryl rotating sutures

81
Post op review Bleeding Under correction Over correction Corneal damage

82
S A F E S – surgery A – antibiotics F – face washing E - environment

83
Tarsal plate rotation surgery Training a local nurse to do the surgery in rural areas

84
Follow up Do things right the first time many patients never return for follow up. Promote cataract and trachoma surgery Don’t build a program on glaucoma control

85
Refractive errors Nearsighted – myopia Farsighted – hyperopia Astigmatism Presbyopia

86
Glaucoma Acute angle closure Chronic open angle Other glaucomas

87
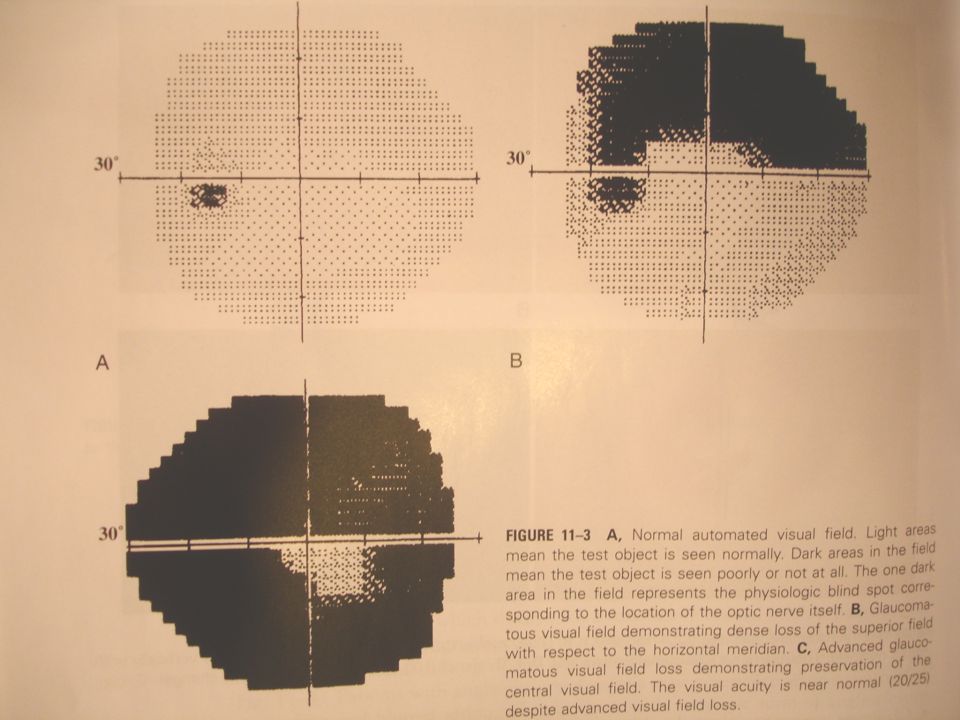
Chronic glaucoma Intraocular pressure Cup disc ratio Visual field

88
Cup disc ratio slides

89
Normal retina

90
measurement 0.5 0.7

91
0.8 0.9 0.7

92
0.8 0.3 0.6

93
Comparison of ACG and Uveitis

94
Aqueous flow in the eye & filtering mechanism

95
Iris position in angle closure glaucoma

96
Angle closure glaucoma

97
Glaucoma Acute angle closure Sudden onset Painful Sudden loss of vision Red eye Very high pressure Closed angle Fair complexion Chronic Open Angle Gradual onset Painless Gradual visual loss Eye not red Medium pressure rise Open angle Dark complexion

98
Angle Closure Glaucoma Note: irregular light reflex, mid-sized pupil

99
Glaucoma Acute Angle Closure Glaucoma – This is the only common type of glaucoma with a significant red eye – Unilateral pain, redness, decreased vision, “halos” around lights before the peak of signs and symptoms – Cloudy cornea (scattered light reflex); fixed, mid- dilated pupil; red eye with ciliary flush, shallow anterior chamber with iris shadow. Treatment – Lower Intraocular pressure (pilocarpine drops and acetazolamide orally) and referral for laser or surgical peripheral iridotomy if medical treatment fails
 and referral for laser or surgical peripheral iridotomy if medical treatment fails.")
102
Chronic glaucoma treatment Prevent with early screening at age 40 and older Timolol and / or Xalatan eye drops For high pressures – acetazolamide orally If pressures remain high on treatment – then surgical intervention is needed.

103
Macular Degeneration age related gradual loss of central vision Loss of vision is permanent but peripheral vision remains intact. No treatment – need to encourage use of visual aids

105
Red Eye: overview Allergic Conjunctivitis Infectious Conjunctivitis Infectious Keratitis Orbital cellulitis Measles Vitamin A deficiency Inflammatory causes Tumors Traumatic causes Glaucoma Contact Lens complications Eyelid Margin disease infectious inflammatory nutritional neoplastic mechanical allergic

106
blinding or non-blinding If both eyes are red treat them If one eye is red and painful refer

107
Use extreme caution with steroids in a red eye You should probably consult an Ophthalmologist first

108
Never use a topical anesthetic to treat pain in an eye cyclopentolate drops topically give relief for a painful eye if necessary anesthetic drops can be used when examining the eye

109
Allergic Conjunctivitis Atopic – Associated with asthma & eczema Allergic – Associated with sinus congestion & pain, runny nose, and itching Drug allergy – Atropine, neomycin, and also lotions, and contact allergies – History will help with the diagnosis

110
Allergic conjunctivitis Note: whitish papillae are seen on the upper lid conjunctiva

111
Allergic conjunctivitis Limbal irritationCobblestone papillae and shield ulcer

112
Cold water rinse Cold compresses Zinc sulphate drops or artificial tears NSAID drops or Mast cell inhibitor drops or anti-histamines Severe disease with papillae need aggressive treatment with steroid drops and short courses of oral steroids. Allergic conjunctivitis treatment

113
Pterygium This is a growth of fibrovascular tissue onto the conjunctiva and cornea Associated with sun, wind, and dust exposure Treatment – Usually unnecessary – If inflamed, topical NSAIDs or steroids – If obscuring the visual axis, refer for surgical removal

114
Pterygium Note: triangular shape of pterygium, with parallel vessels

Similar presentations







































 and associated interneurones and sensory neurones. BiologyMad.com.>")


