Download presentation
Presentation is loading. Please wait.

1
Elective Cesarean Delivery, Neonatal Intensive Care Unit Admission, and Neonatal Respiratory Distress 楊明智

2
Introduction GA of elective C/S vs risk of neonatal respiratory distress → guidelines recommending elective cesarean delivery at term (39 weeks or later). 4–5% of neonates will still develop signs of respiratory distress → labor before caesarean delivery is associated with a lower rate of neonatal respiratory distress. The mechanism of this effect is unknown, but it is postulated to be secondary to activation of epithelial sodium channels in the fetal lung.

3
Glucocorticoids appear to be a potent up- regulator of the expression of epithelial sodium channel genes and are secreted in increasing amounts by the fetal adrenal gland at term. Fetal hypothalamic-pituitary-adrenal axis maturation and adrenal glucocorticoid production are also felt to be possible triggers for the onset of labor at term. Adrenal production of glucocorticoids may both initiate labor and prepare the fetus for extra-uterine life.

4
It has been postulated that the rates of respiratory distress could be reduced further if elective cesarean delivery is delayed until the onset of labor or ruptured membranes. Most of the studies that reported a protective effect of labor included women who had cesarean delivery after prolonged labor and not just women having an elective repeat cesarean delivery shortly after the onset of labor. The lower rates of respiratory distress observed following cesarean delivery after the onset of labor may simply reflect that these fetuses were more likely to be truly at a term gestation. It is not clear whether the short duration of labor before elective repeat cesarean delivery is protective.

5
Intent of the Study To estimate whether the risk of neonatal intensive care unit (NICU) admission and neonatal respiratory distress was lower in women undergoing cesarean delivery after spontaneous rupture of membranes or the onset of labor To confirm the relationship between gestational age at cesarean delivery and risk of respiratory distress
 admission and neonatal respiratory distress was lower in women undergoing cesarean delivery after spontaneous rupture of membranes or the onset of labor To confirm the relationship between gestational age at cesarean delivery and risk of respiratory distress")
6
Materials and Methods All elective cesarean deliveries done in the Calgary Health Region, Calgary, Alberta, Canada March 1, 2004, to April 30, 2005 13,360 deliveries, C/S rate: 26.4% 9 (3527) GA ≧ 37 wks, BW ≧ 2500 g, Elective C/S Maternal data: age, gravidity, parity, antepartum risks Intrapartum factors including rupture of membranes, presence of contractions, and duration of labor Antepartum or intrapartum maternal medications, postpartum complications, and length of stay Labor before cesarean delivery was defined as the presence of symptomatic contractions or rupture of membranes before cesarean delivery.
 GA ≧ 37 wks, BW ≧ 2500 g, Elective C/S Maternal data: age, gravidity, parity, antepartum risks Intrapartum factors including rupture of membranes, presence of contractions, and duration of labor Antepartum or intrapartum maternal medications, postpartum complications, and length of stay Labor before cesarean delivery was defined as the presence of symptomatic contractions or rupture of membranes before cesarean delivery.")
7
Materials and Methods Newborn data: birth weight, gender, Apgar scores, cord pH, resuscitation parameters, treatment provided if admitted to NICU, diagnoses, and length of stay. Twin A was included only (higher risk in twin B). Definition of respiratory distress: tachypnea, with respiratory rate of more than 60 breaths per minute, retractions, grunting, nasal flaring, and cyanosis in room air, or requiring treatment with any of the following: supplemental oxygen, nasal continuous positive airway pressure, endotracheal intubation, or exogenous surfactant.
. Definition of respiratory distress: tachypnea, with respiratory rate of more than 60 breaths per minute, retractions, grunting, nasal flaring, and cyanosis in room air, or requiring treatment with any of the following: supplemental oxygen, nasal continuous positive airway pressure, endotracheal intubation, or exogenous surfactant..")
8
Results 1,193 paired maternal-infant charts matched the criteria of study (≥ 36 wks GA, ≥ 2500 g). The mean (standard deviation) maternal age was 32.1±4.8 years. Spontaneous onset of labor before cesarean delivery occurred in 225 of 1,193 women (18.9%), of whom, 142 reported symptomatic contractions, and 104 had spontaneous rupture of membranes.
 maternal age was 32.1±4.8 years. Spontaneous onset of labor before cesarean delivery occurred in 225 of 1,193 women (18.9%), of whom, 142 reported symptomatic contractions, and 104 had spontaneous rupture of membranes..")
9
[Help with image viewing] [Email Jumpstart To Image]
![[Help with image viewing] [ Jumpstart To Image]](http://images.slideplayer.com/19/5866126/slides/slide_9.jpg "[Help with image viewing] [ Jumpstart To Image]")
10
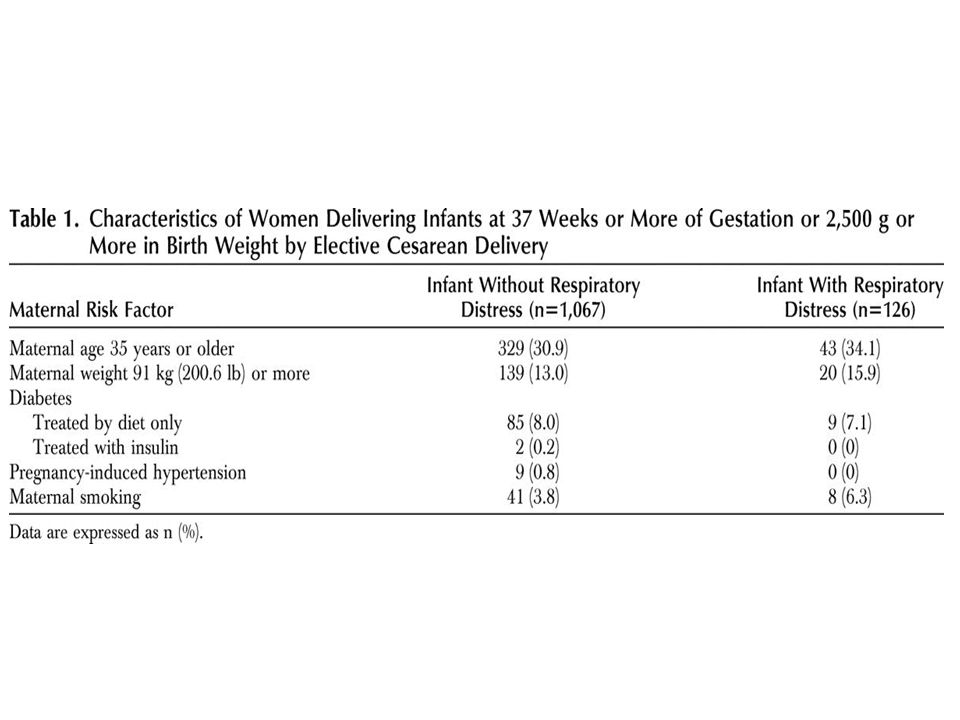
Results Previous cesarean delivery (89%) Breech (6.5%), twins (1.9%), placenta previa (1.1%), primary elective (0.8%), and previous uterine surgery (0.4%), others (0.3%) A third of the mothers were more than 35 years of age, and 13–15.9% were obese, correlating with 7.1–8.0% having diet- managed diabetes, with no difference between mothers whose infants had symptoms of respiratory distress and those who did not.
 Breech (6.5%), twins (1.9%), placenta previa (1.1%), primary elective (0.8%), and previous uterine surgery (0.4%), others (0.3%) A third of the mothers were more than 35 years of age, and 13–15.9% were obese, correlating with 7.1–8.0% having diet- managed diabetes, with no difference between mothers whose infants had symptoms of respiratory distress and those who did not.")
12
Results The mean (± standard deviation) gestational age of the infants at time of elective cesarean delivery was 271.4±6.7 days or 38 5/7 weeks. The mean birth weight was 3,397±480 g. Fifty-two percent were male infants. Twenty-three (1.9%) infants were from twin sets, and the gestational age of these infants ranged from 254 to 268 days (36 2/7 to 38 2/7 weeks). Five of these infants were at a gestational age of less than 259 days (37 0/7 weeks). From the 23 twin infants, three were admitted to NICU.
 infants were from twin sets, and the gestational age of these infants ranged from 254 to 268 days (36 2/7 to 38 2/7 weeks). Five of these infants were at a gestational age of less than 259 days (37 0/7 weeks). From the 23 twin infants, three were admitted to NICU..")
13
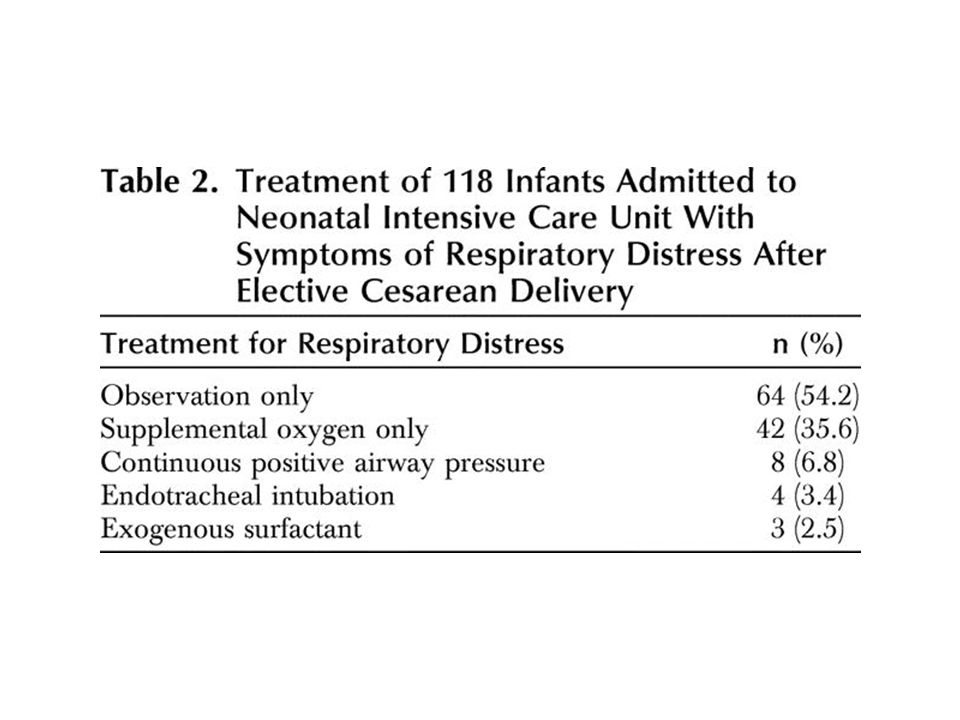
Results Overall, 156 (13.1%) infants delivered by elective cesarean were admitted to NICU. 126 infants were identified to have respiratory distress, although only 118 (9.9%) of these infants were admitted to NICU.
 of these infants were admitted to NICU..")
15
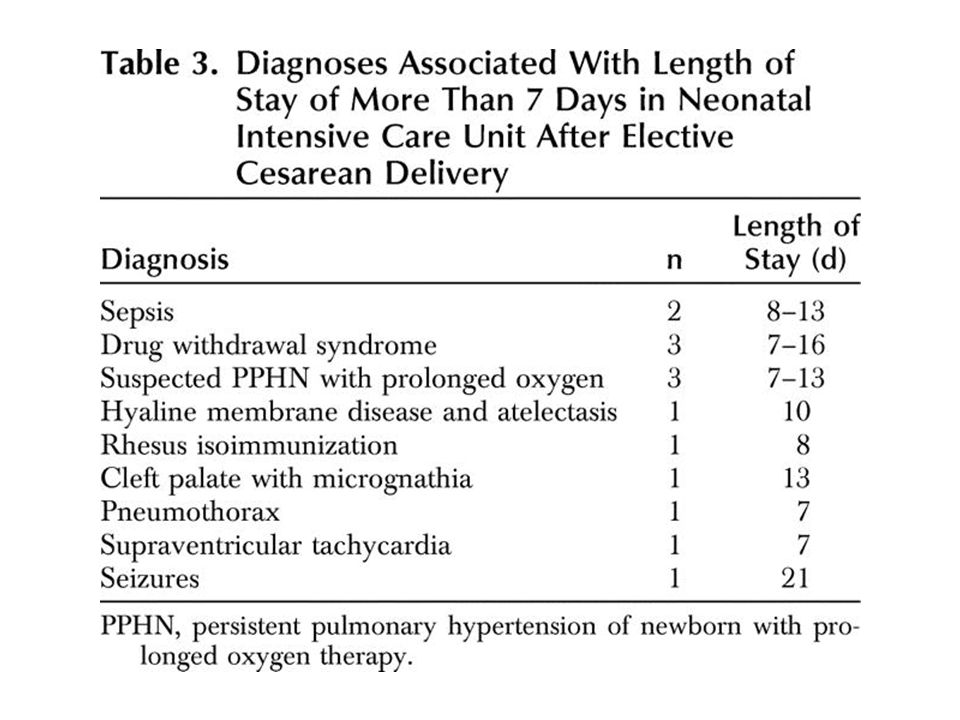
Two thirds of the infants admitted to the NICU with symptoms of respiratory distress had short stays, with a mean of 6.4 hours, but the remaining third had a mean length of stay of 1.9 days. Several infants with other diagnoses had lengths of stay beyond 7 days (Table 3).Table 3
.Table 3.")
18
Fig. 2. Smoothed fit of relationship between respiratory distress and gestational days. Points on the Y axis indicate respiratory distress=1 and no respiratory distress=0.

20
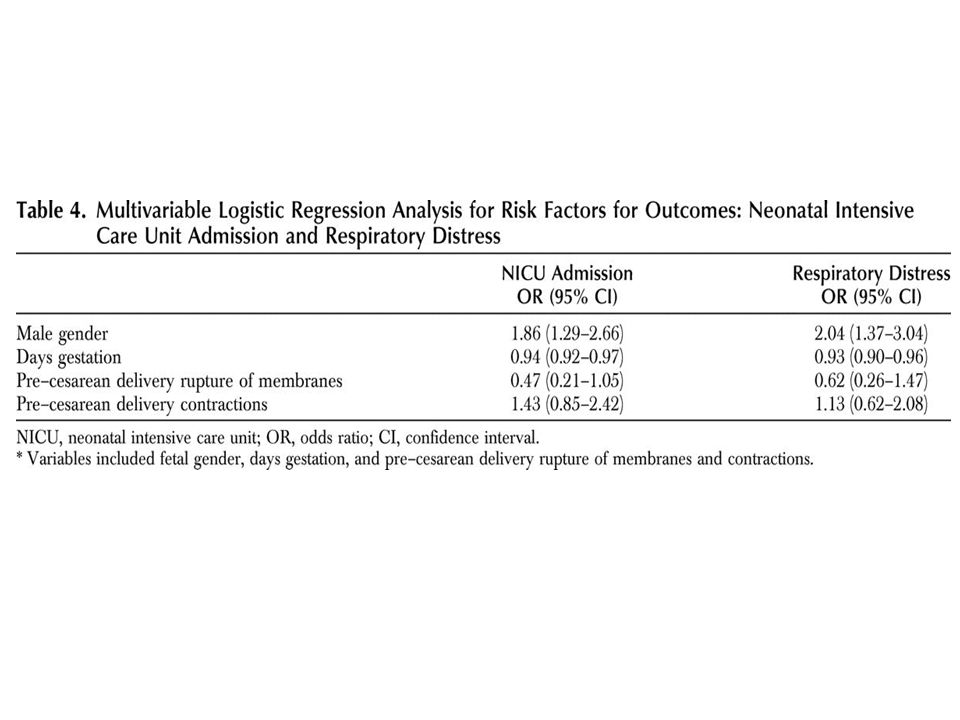
Discussion In this study, the risk for admission to NICU and development of neonatal respiratory distress were significantly associated with gestational age at time of elective cesarean delivery and male gender. In this population studied, if elective cesarean delivery were planned for beyond 270 days (38 4/7 weeks) of gestation, the risk of respiratory distress could be reduced by 50%, and NICU admission could be reduced by approximately 40% in these neonates.
 of gestation, the risk of respiratory distress could be reduced by 50%, and NICU admission could be reduced by approximately 40% in these neonates..")
21
It was anticipated that not all cases will be appropriate for delay of delivery until 38 4/7 weeks and that the risk of respiratory distress and neonatal admission will be one of the factors in considering the optimal time of delivery.

22
Numerous studies have identified similar relationships between respiratory morbidity, need for NICU admission, and gestational age. The recommendation from these studies is that cesarean delivery at 39 weeks or later significantly reduces the risk of respiratory morbidity. These recommendations are stated in the American College of Obstetricians and Gynecologists (ACOG) Committee Opinion 98, published in 1991.
 Committee Opinion 98, published in")
23
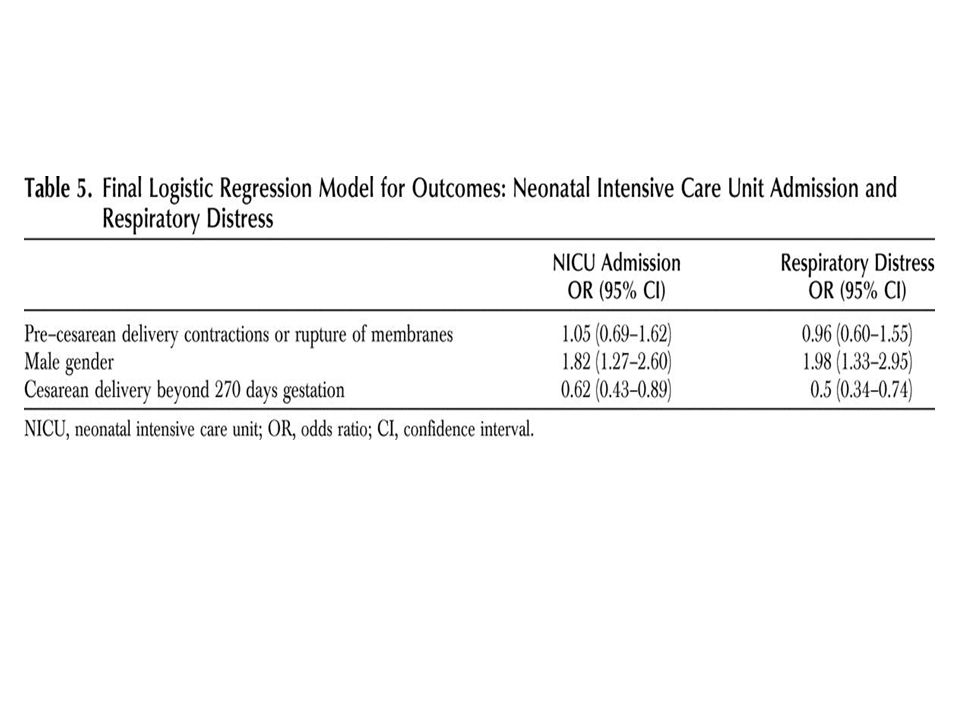
Conclusion In the final model, elective cesarean occurring beyond 270 days of gestation (38 4/7 weeks) significantly reduced the risk of NICU admission and the risk of respiratory distress, but again the presence of pre–cesarean delivery contractions or rupture of membranes did not further reduce this risk.
 significantly reduced the risk of NICU admission and the risk of respiratory distress, but again the presence of pre–cesarean delivery contractions or rupture of membranes did not further reduce this risk.")
24
Many Thanks for Your Attention!

Similar presentations






 Core Measure Set Celeste Milton, MPH, BSN, RN Associate Project Director Department of Quality Measurement.>")

 Guidelines ( )>")


, a common medical complication of pregnancy, is defined as “any degree of glucose intolerance with onset or first.>")







