Download presentation
Presentation is loading. Please wait.

1
This lecture was conducted during the Nephrology Unit Grand Ground by Medical Student under Nephrology Division under the supervision and administration of Prof. Jamal Al Wakeel, Head of Nephrology Unit, Department of Medicine and Dr. Abdulkareem Al Suwaida, Nephrology Consultant. Nephrology Division is not responsible for the content of the presentation for it is intended for learning and /or education purpose only.

2
Hyperkalemia Dr: fatimah al-faraj

3
Potassium homeostasis
-Gastrointestinal absorption is complete, resulting in daily excess intake of about 1 mmol/kg/d this excess is (10%) through the gut (90%) excreted through the kidneys - The most important site of regulation is the distal nephron, including the distal convoluted tubule, the connecting tubule, and the cortical collecting tubule
 through the gut. (90%) excreted through the kidneys. - The most important site of regulation is the distal nephron, including the distal convoluted tubule, the connecting tubule, and the cortical collecting tubule.")
4
Excretion is increased by the following:
-Aldosterone -High sodium delivery to the distal tubule (eg, diuretics) -High urine flow (eg, osmotic diuresis) -High serum potassium level -Delivery of negatively charged ions to the distal tubule (eg, bicarbonate)
 -High urine flow (eg, osmotic diuresis) -High serum potassium level. -Delivery of negatively charged ions to the distal. tubule (eg, bicarbonate)")
5
Excretion is decreased by the following:
-Absence of aldosterone -Low sodium delivery to the distal tubule -Low urine flow -Low serum potassium level -Renal failure

6
Function of Potassium in the Body
muscle contraction regulation of the heart contractility important for the kidney to function normally

7
-The normal serum level of potassium is 3.5 to 5 mmol/L
-Daily Requirements 1-1,5 mmol/kg -Dietary sources include dried fruits; legumes; meats; poultry; fish; soy; bananas; citrus fruits; potatoes; tomatoes; broccoli; mushrooms; dark, leafy green vegetables

8
Hyperkalemia Hperkalemia is defined as a condition in which serum potassium greater than 5.3 mEq/L

9
Pseudohyperkalemia -is the term applied to the clinical situation in which in vitro lysis of cellular contents leads to the measurement of a high serum potassium level not reflective of the true in vivo level. -condition occurs most commonly with red cell hemolysis during the blood draw (tourniquet too tight or the blood left sitting too long),
,")
10
causes Excessive intake Decreased excretion
Shift from intracellular to extracellular space

11
Excessive intake - uncommon cause of hyperkalemia.
-The mechanisms for shifting potassium intracellularly and for renal excretion allow a person with normal potassium homeostatic mechanisms to ingest virtually unlimited quantities of potassium in healthy individuals. -Most often, it is caused in a patient with impaired mechanisms for the intracellular shift of potassium or for renal potassium excretion

12
Decreased excretion -is the most common cause
-The causes of decreased renal potassium excretion include: renal failure diabetes mellitus sickle cell disease medications (eg, potassium-sparing diuretics, NSAID,angiotensin-convening enzyme inhibitors)
")
13
Shift from intracellular to extracellular space
- uncommon alone -but can exacerbate hyperkalemia produced by a high intake or impaired renal excretion of potassium. -It can be the major cause of hyperkalemia in hyperosmolalit, rhabdomyolysis, tumor lysis, succinylcholine administration, insulin deficiency or acute acidosis.

14
Causes Shift from (ICF to ECF) Decreased renal excretion
Excessive intake Hyperosmolality rhabdomyolysis tumor lysis Succinylcholin insulin deficiency acute acidosis. Diabetes mellitus (esp diabetic nephropathy Renal failure Congestive heart failure SLE Sickle cell anemia NSAID ACE Inhibitor Potassium sparing Diuretics Multiple Myeloma chronic partial urinary tract obstruction Oral or IV Potassium Supplementation Salt substitute Blood transfusion

15
Symptoms weakness and fatigue(most common) frank muscle paralysis
shortness of breath palpitations

16
Physical -vital signs generally are normal except
bradycardia due to heart block or tachypnea due to respiratory muscle weakness.

17
Lab Assess renal function.
Check serum BUN and creatinine levels to determine whether renal insufficiency is present Check 24-hour urine for creatinine clearance Estimate the glomerular filtration rate (GFR)
")
18
Measure complete blood count.
-A low hemoglobin and hematocrit or abnormal red cell morphology may suggest hemolysis. -Severe leukocytosis or thrombocytosis raises the possibility of pseudohyperkalemia.

19
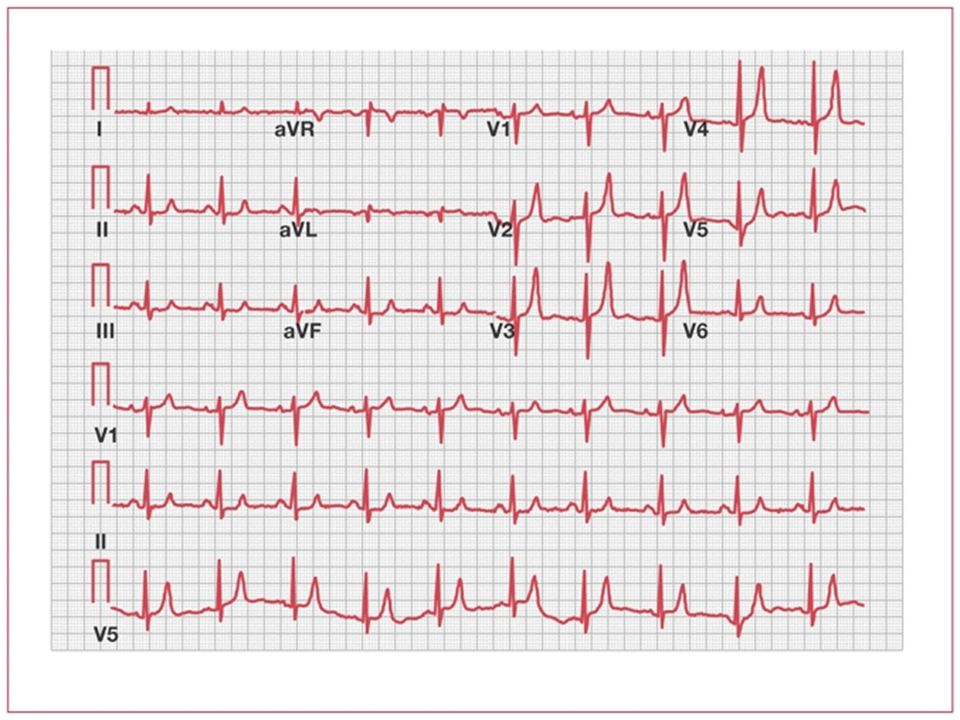
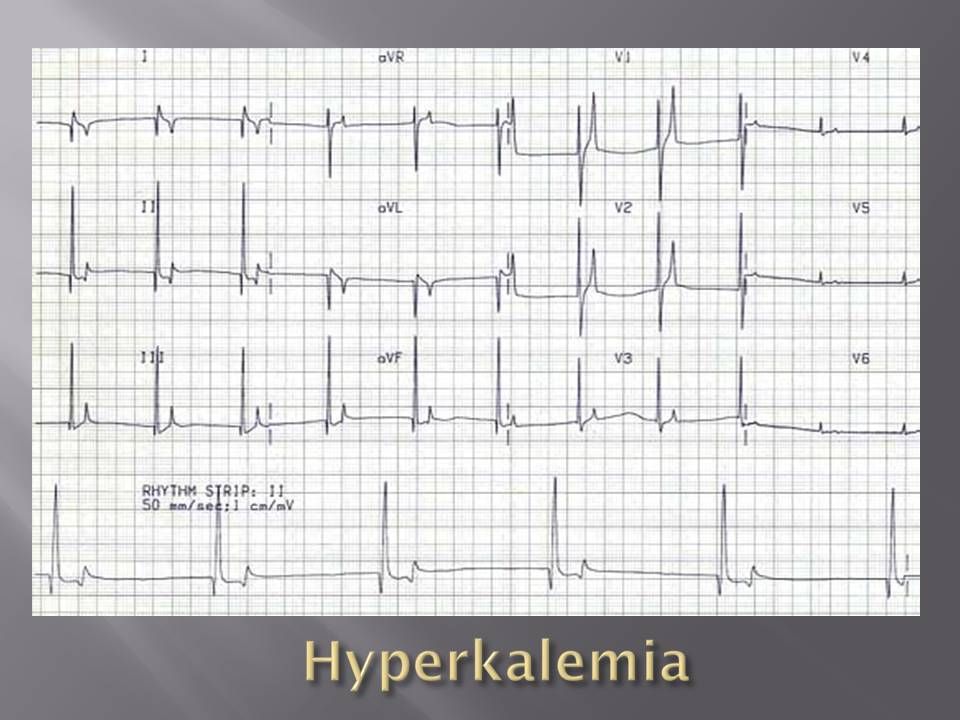
ECG Changes occur when Serum Potassium >6.0 mmol /L A-Initial
T Waves peaked or Tented B-Next ST depression loss of P Wave QRS widening C-Final Biphasic wave (sine wave) QRS and T fusion
 QRS and T fusion.")
23
Measure complete metabolic profile
-Low bicarbonate may suggest hyperkalemia due to metabolic acidosis. -Hyperglycemia suggests diabetes mellitus.

24
-A creatine kinase (CK) elevation suggests rhabdomyolysis.
-Elevated lactic dehydrogenase (LDH), uric acid, phosphate, and alanine aminotransferase (ALT) may suggest tissue breakdown, as occurs in hemolysis, rhabdomyolysis, or tumor lysis.
, uric acid, phosphate, and alanine aminotransferase (ALT) may suggest tissue breakdown, as occurs in hemolysis, rhabdomyolysis, or. tumor lysis.")
25
Treatment The first step -determine life-threatening toxicity.
By Perform an ECG to look for cardiotoxicity. - if present Administer Iv Calcium Gluconate to ameliorate cardiac toxicity. -Initial dose: 10 ml over 2-5 minutes Second dose after 5 minutes if no response -Effect occurs in minutes and lasts for minutes Anticipate EKG improvement within 3 minutes

26
The second step -is to identify and remove sources of potassium intake -Change the diet to a low-potassium diet.

27
The third step -Potassium shift from intravascular to intracellular
-Glucose and Insulin Infusion Insulin Regular 10 units IV 50 ml 50% of dextrose Every mints -Measure glucose and potassium every 2 hours -Correct metabolic acidosis with sodium bicarbonate. 50ml 50% bolus

28
-is to increase potassium excretion from the body
The fourth step -is to increase potassium excretion from the body -in normal kidney function by the administration of parenteral saline accompanied by a loop diuretic, such as furosemide Dose: mg IV.

29
-Discontinue potassium-sparing diuretics, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and other drugs that inhibit renal potassium excretion. Monitor volume status and aim to maintain euvolemia. -in patients with hyporeninemia or hypoaldosteronism Renal excretion can be enhanced by administration of an aldosterone analogue, such as 9-alpha fluorohydrocortisone acetate (Florinef).
.")
30
Emergency dialysis is a final recourse for unresponsive hyperkalemia with renal failure.

32
thanks

Similar presentations








 Major determinant of resting membrane potential. (arrhythmia’s etc) Long term =>")

What are the adverse medical implications of this condition.>")









