Download presentation
Presentation is loading. Please wait.

1
Hasan AYDIN, MD Yeditepe University Hospital Endocrinology and Metabolism Hypercalcemic Disorders

2
Etiologies of Hypercalcemia Increased GI Absorption Milk-alkali syndrome Elevated calcitriol Vitamin D excess Excessive dietary intake Granulomatous diseases Elevated PTH Hypophosphatemia Increased Loss From Bone Increased net bone resorption Elevated PTH Hyperparathyroidism Malignancy Osteolytic metastases PTHrP secreting tumor Increased bone turnover Paget’s disease of bone Hyperthyroidism Decreased Bone Mineralization Elevated PTH Aluminum toxicity Decreased Urinary Excretion Thiazide diuretics Elevated calcitriol Elevated PTH

3
ETIOLOGY TThiazide, other drugs - Lithium R Rabdomyolysis AAIDS PPaget’s disease, Parental nutrition, Pheochromocytoma, Parathyroid disease VVitamins IImmobilization TThyrotoxicosis AAddison’s disease MMilk-alkali syndrome IInflammatory disorders NNeoplastic related disease SSarcoidosis Approx. 80% of all cases are caused by Malignancy or Primary Hyperpathyroidism

4
CLASSIFICATION PTH-Dependent Hypercalcemia Primary hyperparathyroidism Tertiary hyperparathyroidism Familial hypocalciuric hypercalcemia Lithium-asociated hypercalcemia

5
CLASSIFICATION Neoplasms PTHr-P dependent Other humoral syndromes Osteolytic metastases and multiple myeloma ExcessVitamin D/1,25(OH)2D Vitamin D ingestion 1,25(OH)2D intoxication Toica ş l vitamin D analogues Sarcoidosis and other granulomatous diseases Williams syndrome Hyperthyroidism Adrenal insufficiency Renal failure İ mmobilization Jansen’s metapyseal chondrodysplasia Drugs Vitamin A intoxication Milk alkali syndrome Thiazide diuretics Theophylline PTH-Independent Hypercalcemia
2D Vitamin D ingestion 1,25(OH)2D intoxication Toica ş l vitamin D analogues Sarcoidosis and other granulomatous diseases Williams syndrome Hyperthyroidism Adrenal insufficiency Renal failure İ mmobilization Jansen’s metapyseal chondrodysplasia Drugs Vitamin A intoxication Milk alkali syndrome Thiazide diuretics Theophylline PTH-Independent Hypercalcemia")
6
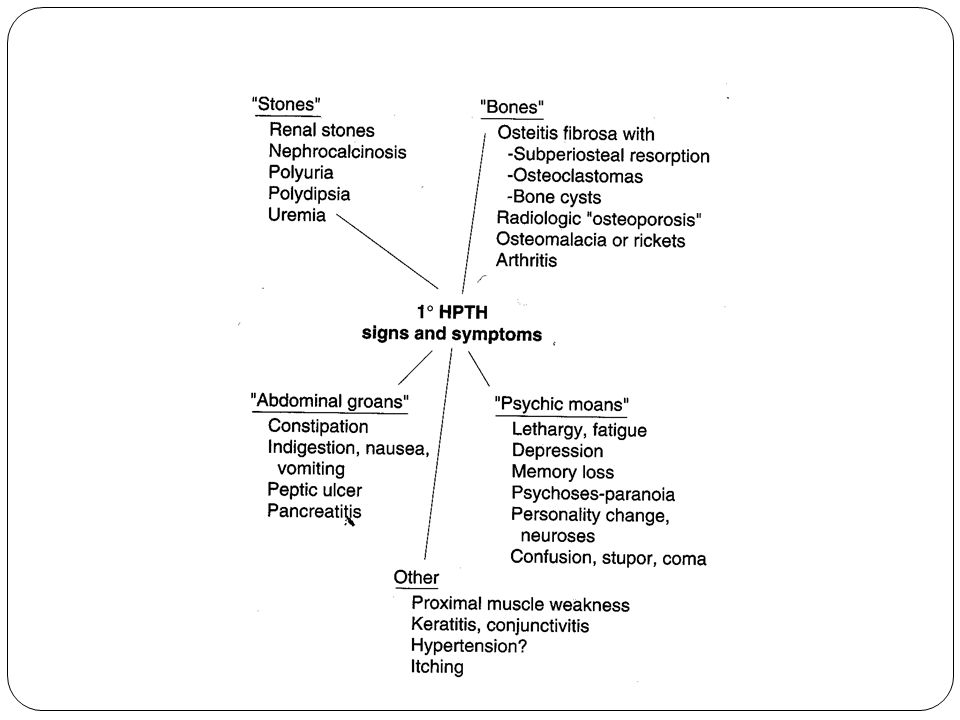
CLINICAL MANIFESTATIONS GI- Anorexia, Nausea, Vomiting, Constipation and rarely acute Pancreatitis. CVS- Hypertension, shortened QT interval RENAL- Thirst, Polyuria, Polydipsia, and occasionally Nephrocalcinosis. CNS- Cognitive difficulties, Apathy, Drowsiness, Obtundation, or even Coma. -Anxiety, Depression, Psychosis Ectopic Calcifications- Nephrocalcinosis, calcifications of blood vessels, band keratopathy

7
SYMPTOMS More than 50% of all patients with primary hyperparathyroidism are asymptomatic when hypercalcemia is first discovered.

9
COMPLICATIONS Sinus bradycardia Increase in the degree of a heart block Cardiac arrhythmia Hypertension Pancreatitis Peptic ulcer disease Nephrolithiasis Accelerated vascular calcification

10
Diagnostic Yield in Hypercalcemia InvestigationPotential Information Full Blood CountAnemia suggest non-parathyroid etiology if renal function normal ESRUsually over 80 in myeloma Plasma chlorideUpper normal in hypepararthyroidism Plasma bicarbonateLow normal in hypepararthyroidism CreatinineSignificantky raised in tertiay hyperparathyroidism of renal failure. Moderately raised in renal impairement secondary to hypercalcemia Plasma protein electrophoresisMonoclonal band suggest myeloma Urinary immunelectrophoresisPresece of light chain suggest myeloma Plasma phosphateLow normal in primary hyperparathyroidism unless renal function impaired Plasma PTHUpper normal or raised in hyperparathyroidism Suppressed with other causes of hypercalcemia Steroid suppression testSarcoid hypercalcemia alwasy suppress, hyperparathyroid never, malignanat causes occasionally 24 h urine calciumDecreased in FHH Chest X-rayNeoplasms, hilar LAP in sarcoidosis Isotope bone scan‘Hot spots’ suggest metastases X-ray handsSubperiosteal erosions suggest hyperparathyroidism

11
HYPERCALCEMIA PTH high Hyperparathroidism PTH - N or Low Malig- prim. or mets Vit high consider Sarcoidosis CXR Consider other *Hyperthyroidism *Milk-alkali syndrome *Familial hypocalciuric hypercalcemia If cause remain unclear measure Vit D Measure PTH Determine wheather hypercalcemia is real, measure ionized Ca adjust for change in serum albumin level, careful drug hx Li, Vit D or A, SERUM CALCIUM > 10.6

12
MANAGEMENT OF SYMPTOMATIC HYPERCALCEMIA General measures Saline diuresis Specific measures Glucocorticoids Phosphate infusion Bisphosphonates Calcitonin Dialysis

13
LOOP DIURETICS Facilitate urinary excretion of calcium By inhibiting calcium reabsorption in the thick ascending limb of the loop of Henle. Guard against volume overload Volume expansion must precede the administration of furosemide, because the drug’s effect depends on delivery of calcium to the ascending limb. Needs frequent measurement of lytes and water

14
CALCITONIN Not as effective as bisphosphonate, tachyphylaxis quickly occurs and limits therapeutic efficacy MITHRAMYCIN Toxic effect limits it’s use, reserved for difficult cases of hypercalcemia that are related to malignancy GALLIUM NITRATE Need to infuse it over 5 days, nephrotoxity limits it’s use, not used frequently CORTICOSTEROIDS For myeloma, lymphoma, Sarcoidosis, or vit D toxicity decrease GI absorption, 200- 300mg hydrocort for upto 5 days, slow response limits it’s use HEMODIALYSIS Zero or low calcium bath, In selected condition, eg-hypercalcemia complicated by renal failure

15
BISPHOSPHONATES Structurally related to pyrophosphate. P-C-P bound is a back bone that renders them resistant to phosphates. They bind to hydroxyapatite in bone and inhibit the dessolution of crystals. Their great affinity for bone and their resistance to degradation account for their extremely long half life in bone. Poor GI absorption- <10% ETIDRONATEPAMIDRONATECLODRONATE

16
CHOICE OF AGENT Mild (<12 mg/dl)-Hydration with saline. Moderate(>15mg/dl) with moderate symptoms- Bisphosphonate. Severe life threatening( >15mg/dl) - Saline + Calcitonin + mithramycin, alternatively bisphosphonate, if steroids sensitive + steroids. Hypercalcemia secondary to malignancy- survival after the appearance of hypercalcemia is very poor - median of 3 months.
 with moderate symptoms- Bisphosphonate. Severe life threatening( >15mg/dl) - Saline + Calcitonin + mithramycin, alternatively bisphosphonate, if steroids sensitive + steroids. Hypercalcemia secondary to malignancy- survival after the appearance of hypercalcemia is very poor - median of 3 months..")
17
SPECIFIC CAUSES OF HYPERCALCEMIA

18
FAMILIAL HYPOCALCIURIC HYPERCALCEMIA Autosomal dominant Inactivating mutation of calcium sensing receptor Shift in the set point for suppression of PTH Starts at birth Serum Ca mild/moderately elevated Urinary calcium excretion low/normal Urinary C Ca /C Cr <0,1 PTH normal/Slightly elevated Multiple, slightly enlarged, policlonal glands Usually asymptomatic Surgery not effective

19
Lithium Toxicity 5% of cases Due to: Increse in the set-point for PTH secretion Increase in tubular reabsorption of calcium After years of treatment Elevation in calcium and PTH Enlargement of parathyroids After withdrawal, Ca and PTH returns normal within several months

20
Hypercalcemia of Malignancy Most common cause in hospitalized patients Most common in Sq. Cell Ca., Breast. Renal Bladder Ca, MM, Lymphoma Uncommon in colon and prostate ca. Occurs in the late course of malignancy Dehydration, immobilization and treatment with certain drugs contribute to or potentiate development of hypercalcemia

21
Hypercalcemia of Malignancy Specific causes of hypercalcemia Direct invasion of bone (local osteolysis)-20-40% Tumor production of circulating factors (PTHrP) that osteoclastic resorption of bone (humoral hypercalcemia of malignancy)-40-50% Ectopic production of 1,25 (OH) 2 D3 (lymphomas) Ectopic production of PTH (Lung, Ovary, Thyroid) Concomitant malignancy and PHP or granulomatous disease Treatment with estrogen and antiestrogen (tamoxifen)
-20-40% Tumor production of circulating factors (PTHrP) that osteoclastic resorption of bone (humoral hypercalcemia of malignancy)-40-50% Ectopic production of 1,25 (OH) 2 D3 (lymphomas) Ectopic production of PTH (Lung, Ovary, Thyroid) Concomitant malignancy and PHP or granulomatous disease Treatment with estrogen and antiestrogen (tamoxifen)")
22
Vitamin D Intoxication >100,000 units/day 25(OH)D level 5-10x high despite N/slightly elevated 1,25(OH) 2 D3 Hypercalcemia and hypercalciuria N/V, weakness, altered consciousness Persist for weeks to months after discontinuation of medication Use of steroids (prednisone 40-60 mg/day)
D level 5-10x high despite N/slightly elevated 1,25(OH) 2 D3 Hypercalcemia and hypercalciuria N/V, weakness, altered consciousness Persist for weeks to months after discontinuation of medication Use of steroids (prednisone mg/day)")
23
Granulomatous Diseases Hypercalcemia in 10%, hypercalciuria 50% of sarcoidosis Correlate with degree of severity and level of ACE Causes High level of 1,25(OH) 2 D3 Overproduction of bone resorbing cytokines Production of PTHrP Treatment with steroids (prednisone 40-60 mg/d)
 2 D3 Overproduction of bone resorbing cytokines Production of PTHrP Treatment with steroids (prednisone mg/d)")
24
Hyperthyroidism 15-50% of cases By direct stimulation of ostoclastic bone resorption Ca levels rarely exceed 11 mg/dL Low PTH, Low 1,25(OH) 2 D3, Hypercalciuria Β -Blockers (propronalol 20-40 qid)
 2 D3, Hypercalciuria Β -Blockers (propronalol qid)")
25
Vitamin A Intoxication >50,000 IU/day Treatment with cis-retinoic acid or all-transretinoic acid Dry skin, pruritus, headache, bone pain By direct stimulation of bone resorption Treatment with hydration and steroids

26
Adrenal Insufficiency Causes Volume depletion with hemoconcentration Increased tubular reabsorption of calcium, Increased skeletal release of calcium Treatment Correction of volume depletion Steroids

27
Thiazide Diuretics Rarely cause hypercalcemia by themselves Causes ↑ renal tubular reabsorption of Ca ↑ bone resorption activity Diuretic-induced volume depletion

28
Milk Alkali Syndrome Ingestion of excessive amounts of milk (calcium supplements) or soluble alkali (antacids) Acute form Triad of hypercalcemia, metabolic alkalosis, renal failure Treatment with rehydration and if necessary dialysis Chronic form (Burnett syndrome) Soft tissue calcifications in kidney and nephrocalcinosis Progressive renal insufficiency
 or soluble alkali (antacids) Acute form Triad of hypercalcemia, metabolic alkalosis, renal failure Treatment with rehydration and if necessary dialysis Chronic form (Burnett syndrome) Soft tissue calcifications in kidney and nephrocalcinosis Progressive renal insufficiency")
29
Immobilization Increased bone resorption Hypercalciuria, ↓ PTH and 1,25(OH) 2 D3 Bisphosphonates ± Calcitonin
 2 D3 Bisphosphonates ± Calcitonin")
30
Williams Syndrome Supravalvular aortic stenosis, elfin facies, mental retardation Hypercalcemia in infancy ( ↑ 1,25(OH) 2 D3) Jansen’s Metaphyseal Chondrodisplasia Short stature, hypercalcemia Similar to PHP PTH-R activating mutation
 2 D3) Jansen’s Metaphyseal Chondrodisplasia Short stature, hypercalcemia Similar to PHP PTH-R activating mutation")
31
HEREDITARY PRIMARY HYPERPARATHYROIDISM SYNDROMES MEN 1 Familial Hypocalciuric Hypercalcemia Neonatal Severe Hyperparathyroidism MEN 2a Hyperparathyroidism-Jaw Tumor Syndrome

32
MEN 1 Parathyroid, enteropancreatic, pituitary and other tumors (85 % HP, 35 % Z-E, 25 % Prolactinoma) Otosomal dominant Inactivating MEN 1 gene germ-line mutation Starting age : 25 Urinary calcium excretion normal-high High PTH Multiple abnormal glands 90 % cure after PTX
 Otosomal dominant Inactivating MEN 1 gene germ-line mutation Starting age : 25 Urinary calcium excretion normal-high High PTH Multiple abnormal glands 90 % cure after PTX")
33
MEN 2A Pheochromocytoma, medullary thyroid CA, mild hyperparathyroidism Activating mutation of the RET proto-oncogene Otosomal dominant

Similar presentations



![Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.](/15/4762424/big_thumb.jpg "Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.>")















