Download presentation
Presentation is loading. Please wait.

1
PERIPHERAL NERVE INJURYIES
MHD BASHAR ALBOSHI

2
Microscopic anatomy

4
INTERNAL TOPOGRAPHY OF PERIPHERAL NERVES

6
NEURONAL DEGENERATION AND REGENERATION:
Phagocytosis Secondary or wallerian degeneration Primary or retrograde egeneration

7
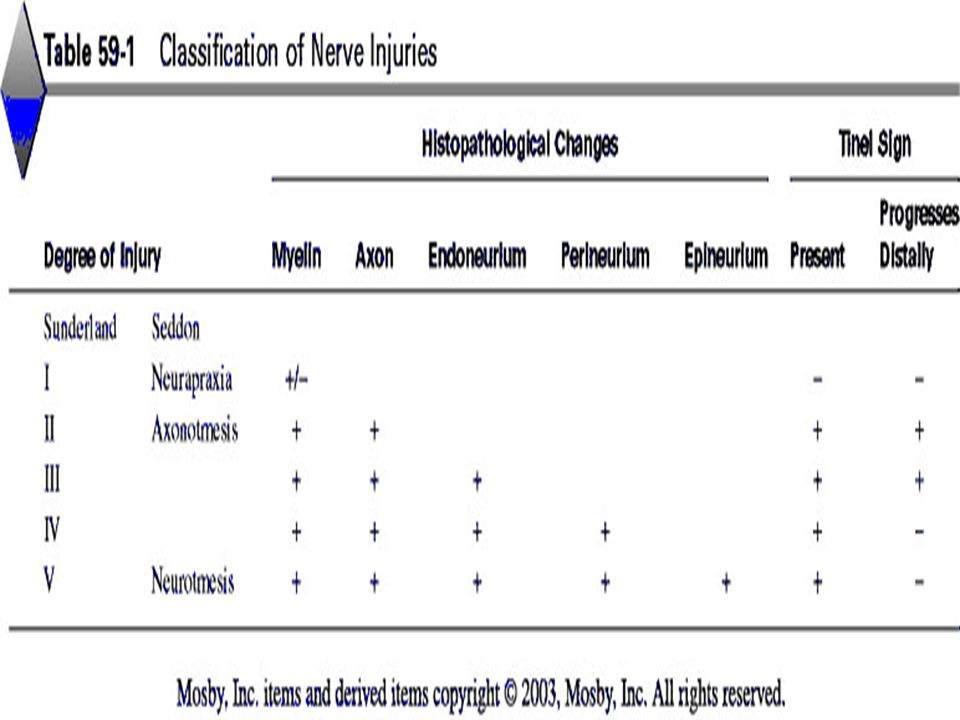
CLASSIFICATION OF NERVE INJURIES: ( Seddon1943):
Neurapraxia Axonotmesis neurotmesis (Sunderland 1951) classification
 classification.")
13
Etiology of peripheral nerve injuries:
- Metabolic or collagen diseases - Malignancies -Endogenous or exogenous toxins -Thermal -Chemical -Mechanical trauma

15
3- muscle contraction against gravity.
Clinical diagnosis of nerve injuries: Highet Scale: 0 – total paralysis. 1- muscle flicker. 2-muscle contraction. 3- muscle contraction against gravity. 4- muscle contraction against gravity and resistance. 5-normal muscle contraction .

16
Diagnostic tests: Electrodiagnostic studies provide the clinician with a base of knowledge as follows:: 1-Documentation of injury Location of insult 2 - 3-Severity of injury 4-Recovery pattern 5-Prognosis 6-Objective data for impairment documentation 7-Pathology 8-Selection of optimal muscles for tendon transfer 9-procedures

17
The most common electrodiagnostic methods used for the study of peripheral nerve injuries are :
@- nerve conduction studies and @-electromyography (EMG)
")
19
Fig Diagram of EMG tracing depicting normal insertion activity, which also may be present immediately after denervation.

20
Fig A, Diagram of EMG tracing demonstrating positive sharp wave consistent with denervation 10 to 14 days after injury. Rhythm is regular, amplitude is 100 to 400 uV, duration is 5 to 150 msec, and rate is 2 to 40 Hz. B, Diagram of EMG tracing demonstrating spontaneous denervation fibrillation potentials present within 14 to 18 days after injury. Rhythm is regular, amplitude is 50 to 1000 uV, duration is 0.5 to 2 msec, and rate is 2 to 30 Hz.

21
Tinel sign : A positive Tinel sign is presumptive evidence that regenerating axonal sprouts that have not obtained complete myelinization are progressing along the endoneurial tube. @- neuropraxia(sunderland1) negative Tinel sign. @- axonotmesis (sunderland2,3) positive Tinel sign. (sunderland negative Tinel sign ) @- neurotmesis (sunderland 5) negative Tinel sign. Other diagnostic test: Sweat test.,skin resistance test, electrical stimulation
 negative Tinel axonotmesis (sunderland2,3) positive Tinel sign. (sunderland negative Tinel sign neurotmesis (sunderland 5) negative Tinel sign. Other diagnostic test: Sweat test.,skin resistance test, electrical stimulation.")
22
2-Gap Between Nerve Ends 3-Delay Between Time of Injury and Repair
GENERAL CONSIDERATIONS OF TREATMENT. FACTORS THAT INFLUENCE REGENERATION AFTER NEURORRHAPHY : 1-Age 2-Gap Between Nerve Ends 3-Delay Between Time of Injury and Repair 4-Level of Injury 5-Condition of Nerve Ends

23
TECHNIQUE OF NERVE REPAIR:
Endoneurolysis (Internal Neurolysis Partial Neurorrhaphy Neurorrhaphy and Nerve Grafting

24
Methods of Closing Gaps Between Nerve Ends:
Mobilization Positioning of Extremity Transposition Bone Resection Nerve Stretching and Bulb Suture Nerve Grafting

25
Techniques of Neurorrhaphy:
Epineurial Neurorrhaphy

26
Perineurial (Fascicular) Neurorrhaphy
 Neurorrhaphy")
27
Interfascicular Nerve Grafting

28
Brachial Plexus

31
ETIOLOGY AND CLASSIFICATION OF BRACHIAL PLEXUS INJURIES :
-birth, -missiles, - stab wounds, - traction applied to the plexus during falls, -vehicular accidents, - sports activities, -as well as radiation.

32
Rupture of the axillary or subclavian artery occurs in 20% of patients.
Common associated injuries include: @fractures of the proximal humerus, the scapula, the ribs, the clavicle, and the transverse processes of the cervical vertebrae @dislocation of the shoulder, the acromioclavicular, and the sternoclavicular joints. @ A torn rotator cuff also has been described in conjunction with brachial plexus injury.

33
Upper plexus injury (Erb)
involves the segments innervated by the C5 and C6 nerve roots with or without dysfunction of the C7 root. -Typically the limb is extended at the elbow(the biceps, brachialis, and brachioradialis muscles) -flaccid at the side of the trunk, -Adducted (deltoid and supraspinatus muscles) -internally rotated (infraspinatus and teres minor muscles, supinator muscle)
 -flaccid at the side of the trunk, -Adducted (deltoid and supraspinatus muscles) -internally rotated (infraspinatus and teres minor muscles, supinator muscle)")
35
Lower plexus injury (Klumpke)
can be diagnosed by finding segmental sensory and motor deficits involving C8 and T1 with or without C7 dysfunction. @ The primary dysfunction is apparent in : -the intrinsic musculature of the hand along with paralysis of the wrist and finger flexors. - The sensory deficit is along the medial aspect of the arm, forearm, and hand. @Associated Horner syndrome should alert the examiner to the possibility of an avulsing injury of the lower plexus, .

37
Injuries to the upper or lower trunks
produce essentially the same sensory and motor deficits as do injuries to their respective rami, except for preservation of function of the long thoracic and dorsal scapular nerves in the upper trunks and absence of Horner syndrome in the lower trunks.

38
Injuries of the lateral cord
deficits in the distribution of: -musculocutaneous nerve (paralysis of the biceps). -lateral root of the median nerve (paralysis of the flexor carpi radialis and pronator teres). -lateral pectoral nerve (clavicular head of the pectoralis major). @Glenohumeral subluxation may result. This may be prevented by an aggressive program of rehabilitation of the remaining intact musculature. @Sensory deficit can be detected over the anterolateral aspect of the forearm in the relatively small autonomous zone of the musculocutaneous nerve.
. -lateral root of the median nerve (paralysis of the flexor carpi radialis and pronator teres). -lateral pectoral nerve (clavicular head of the pectoralis subluxation may result. This may be prevented by an aggressive program of rehabilitation of the remaining intact deficit can be detected over the anterolateral aspect of the forearm in the relatively small autonomous zone of the musculocutaneous nerve.")
39
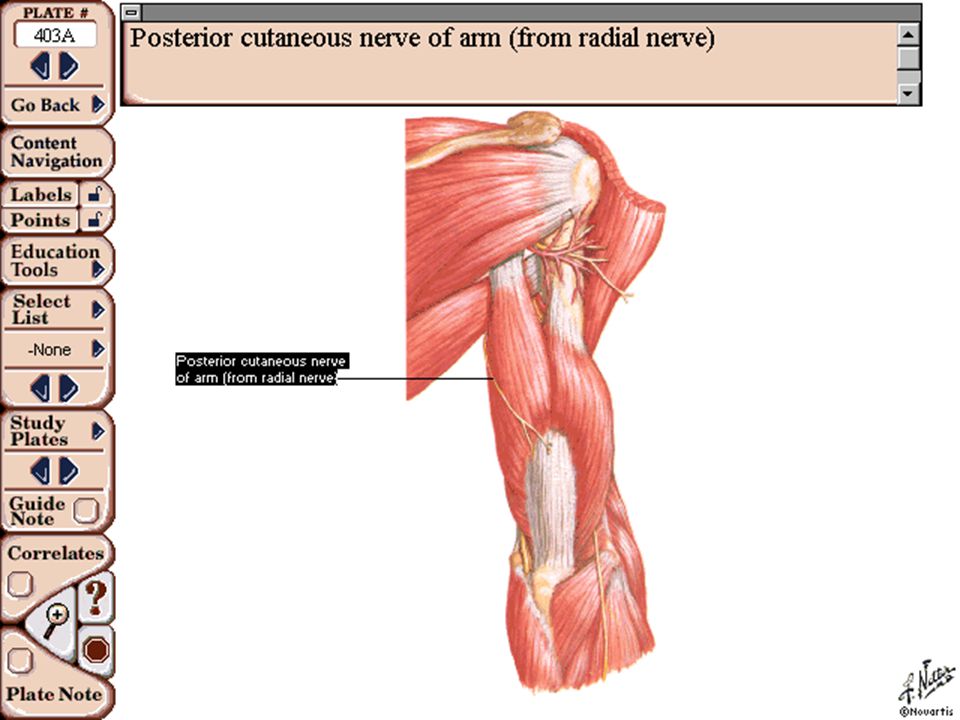
Injuries of the posterior cord
deficits in the distribution of the following nerves: -subscapular (paralysis of the subscapularis and teres major), -thoracodorsal (paralysis of the latissimus dorsi). - axillary (paralysis of the deltoid and teres minor), -radial nerve (paralysis of extension of the elbow, wrist, and fingers). @The disability consists mainly of inability to internally rotate the shoulder, elevate the limb, and extend the forearm and hand. @ Sensory loss most often is apparent only in the autonomous zone of the axillary nerve overlying the deltoid muscle..
, -thoracodorsal (paralysis of the latissimus dorsi). - axillary (paralysis of the deltoid and teres minor), -radial nerve (paralysis of extension of the elbow, wrist, and disability consists mainly of inability to internally rotate the shoulder, elevate the limb, and extend the forearm and Sensory loss most often is apparent only in the autonomous zone of the axillary nerve overlying the deltoid muscle..")
40
Injuries of the medial cord
produce the motor deficit of: - a combined ulnar and median nerve lesion (except for the flexor carpi radialis and pronator teres) and - extensive sensory loss along the medial aspect of the arm and hand
 and. - extensive sensory loss along the medial aspect of the arm and hand.")
41
TREATMENT OF BRACHIAL PLEXUS INJURIES
Open injuries: exploration and primary repair can be attempted. Usually, however, injuries to adjacent vessels or to the mediastinal or thoracic viscera must be treated first, and thus repair of the plexus injury must be delayed. @. Leffert emphasized the poor prognosis after lower trunk injuries but advised surgical exploration for sharp injuries of the upper and middle trunks. @When an open injury has been caused by a low-velocity missile, early exploration is not indicated unless injuries to adjacent vessels or viscera make immediate treatment necessary. @Consequently a period of observation is indicated because considerable function may return spontaneously @Again electromyograms should be obtained 3 to 4 weeks after injury to aid in determining the extent of denervation. Thereafter periodic examinations are indicated every 4 to 6 weeks @When such examinations during a reasonable period of time reveal the absence of recovery or that any recovery has halted, exploration and neurorrhaphy, grafting, or neurolysis may be beneficial

42
Surgical Goals Surgical Goals The surgeon should have clear and reasonable surgical goals, which are in order of priority: (1) restoration of elbow flexion. (2) restoration of shoulder abduction. (3) restoration of sensation to the medial border of the forearm and hand. @After brachial plexus repair and reconstruction, 12 to 18 months are required to determine the extent of neural regeneration. /
 restoration of elbow flexion. (2) restoration of shoulder abduction. (3) restoration of sensation to the medial border of the forearm and brachial plexus repair and reconstruction, 12 to 18 months are required to determine the extent of neural regeneration. /")
43
. Tendon transfers about the shoulder that may be considered include
trapezius to deltoid transfer to improve abduction -latissimus dorsi transfer to improve external rotation. - Shoulder arthrodesis is helpful if active scapulothoracic motion is preserved and has been shown to improve elbow flexion by preventing uncontrolled internal rotation of the shoulder. The shoulder should be fused in only 20 to 30 degrees of abduction because most of these patients..

44
@Operations to restore elbow flexion include transfers of the latissimus dorsi, the pectoralis major, the triceps, the sternocleidomastoid, and the flexor-pronator mass). - Marshall et al. reviewed 50 such transfers and found the latissimus dorsi and triceps transfers to be the most reliable. Restoration of elbow flexion is helpful to the patient even if the hand is functionless

45
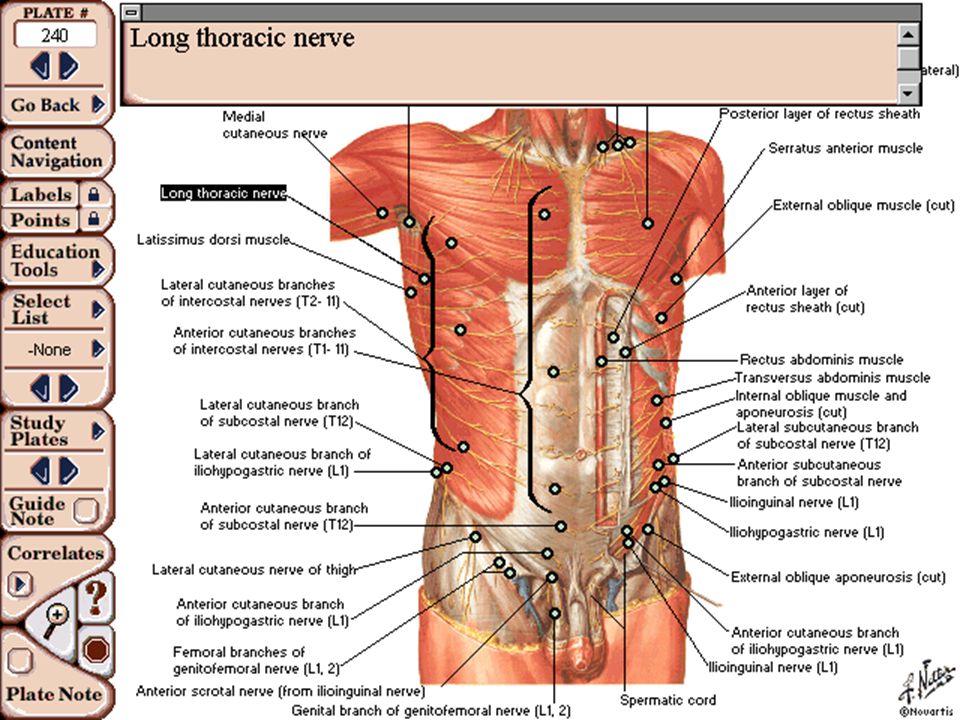
The long thoracic nerve arises from C5, C6, and C7 immediately after they emerge from the intervertebral foramina.

48
. It traverses the neck posterior to the brachial plexus, continues distally along the lateral aspect of the thoracic wall, and innervates the serratus anterior muscle.

50
injuries may result from:
-either sharp or blunt trauma - or from traction when the head is forced acutely away from the shoulder or when the shoulder is depressed, as when carrying heavy weights. - Other causes include exposure to cold, viral infections, and placing patients in the Trendelenburg position with shoulder braces that compress the supraclavicular areas.

51
Examination: -When the serratus anterior is paralyzed, the patient cannot fully flex the arm above the level of the shoulder anteriorly, and active abduction also may be restricted. - When the patient attempts to exert forward pushing movements with the hands, "winging" of the scapula occurs and its vertebral border and inferior angle become unduly prominent.

52
Treatment: When the nerve has been stretched rather than severed, it usually is enough to immobilize the shoulder girdle in extension with the arm against the chest. Care should be taken to avoid contractures of the shoulder, elbow, and wrist while awaiting recovery. -According to Sunderland, the nerve may recover after 3 to 12 months. If paralysis persists or if the nerve has been severed, the prognosis for recovery is poor, and a reconstructive operation may be indicated

56
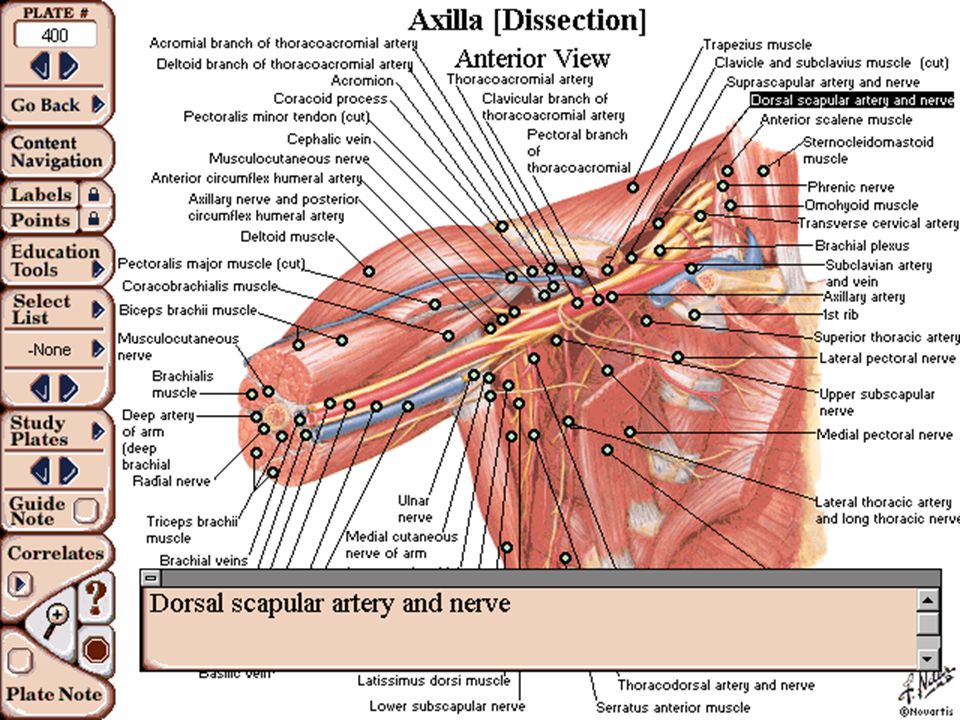
Arising from the upper trunk of the brachial plexus

59
The only surgically significant nerve
The only surgically significant nerve. This is the first important branch seen when the plexus is explored superior to the clavicle. This nerve proceeds distally, passing through the scapular notch to the posterior aspect of the scapula, where it supplies the supraspinatus muscle and, after proceeding around the lateral border of the scapular spine, supplies the infraspinatus muscle..

61
The nerve may be injured by:
-penetrating trauma in the posterior triangle of the neck - cancer surgery in the same area, - blunt or penetrating trauma in the supraclavicular region, - fractures of the superolateral portion of the scapula, especially involving the region of the suprascapular notch, - anterior dislocations of the shoulder joint - entrapment in the suprascapular notch, - space-occupying lesions such as a ganglion at the spinoglenoid notch.

62
Examination -Pain in the shoulder and weakness of the shoulder girdle are common complaints.
Atrophy of both the supraspinatus and infraspinatus muscles may be seen if the nerve is injured at or proximal to the suprascapular notch. - Atrophy of only the infraspinatus muscle suggests entrapment distal to the supraspinatus fossa, as may occur at the spinoglenoid notch. @Electrodiagnostic studies are helpful in confirming the diagnosis

73
The axillary nerve, composed of fibers from C5 and C6, is a branch of the posterior cord of the brachial plexus.

75
emerging inferior to the subscapular and thoracodorsal nerves at the level of the humeral head; it then winds around the neck of the humerus

76
, passing through the quadrangular space to supply the deltoid and teres minor muscles, , and the skin overlying the deltoid. .

78
This nerve commonly is injured by:
-fractures or dislocations about the shoulder, -penetrating wounds, and direct blows. - Rarely, compression of the axillary nerve or one of its major branches may occur in the quadrilateral space and cause chronic pain and paresthesia aggravated by forward flexion or abduction and external rotation of the humerus

79
Examination: -Because a lesion of the axillary nerve sometimes does not cause anesthesia, the diagnosis must rest solely on the presence or absence of function in the deltoid muscle. -Usually deltoid paralysis is easily detected by the inability to actively abduct the arm. However, it is well documented that full abduction of the arm is possible in the presence of deltoid paralysis because of the action of the supraspinatus and because of rotation of the scapula. Therefore it is essential to observe and palpate the deltoid muscle for contraction during the examination. - Electrical stimulation of the nerve in situ is easily accomplished by inserting the needles along the posterior border of the deltoid. Treatment: -Transfer of the insertion of the trapezius is the most satisfactory operation for complete paralysis of the deltoid. -Transfer of Deltoid Origin for Partial Paralysis. .

80
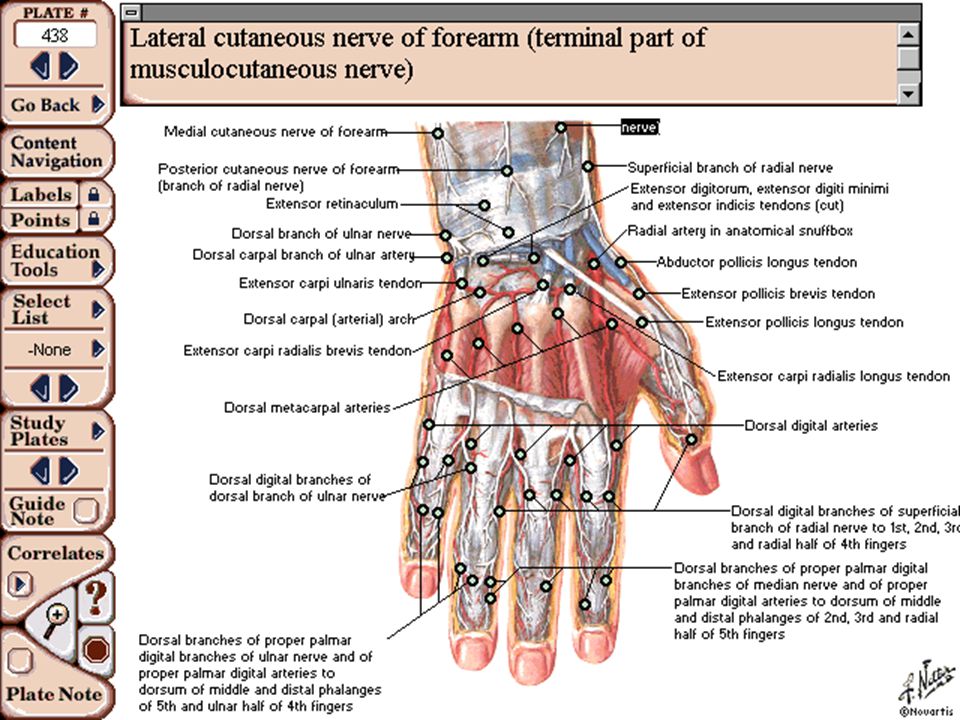
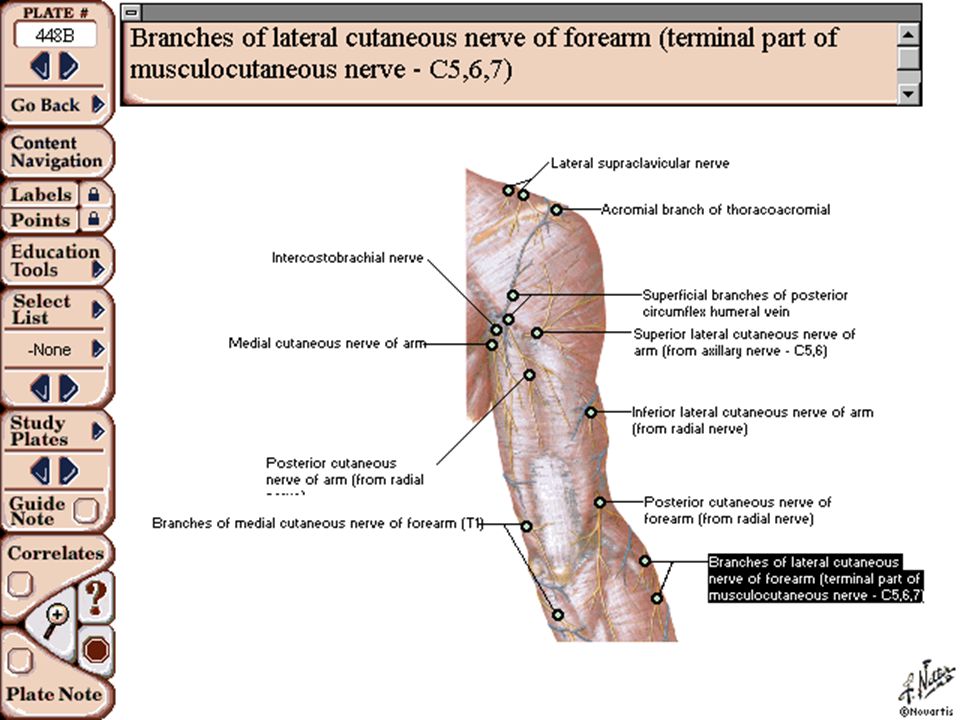
The musculocutaneous nerve, composed of fibers from C5 and C6, is a branch of the lateral cord of the brachial plexus

83
muscles supplied by the musculocutaneous nerve are the biceps; the brachialis and the coracobrachialis.

90
It most commonly is injured by:
-penetrating injuries -occasionally by anterior dislocation of the shoulder or fractures of the humeral neck. - When this nerve is injured in the axilla, the injury often is in conjunction with injuries to other components of the brachial plexus.

91
Examination: -The only muscle supplied by the musculocutaneous nerve that can be examined accurately is the biceps; the brachialis and the coracobrachialis are difficult to palpate. -Complete division of the nerve may be overlooked because the sensory loss may be ill defined and flexion of the elbow by the brachioradialis may be strong enough to mask biceps paralysis. In these instances it is essential to palpate the biceps while testing its function to identify specific muscle contractions - Sensory examination is of no great value because complete anesthesia is rare. Division of this nerve may cause less disability than that of any other major nerve in the body, and for this reason, especially in older patients, suture occasionally is not even indicated.

96
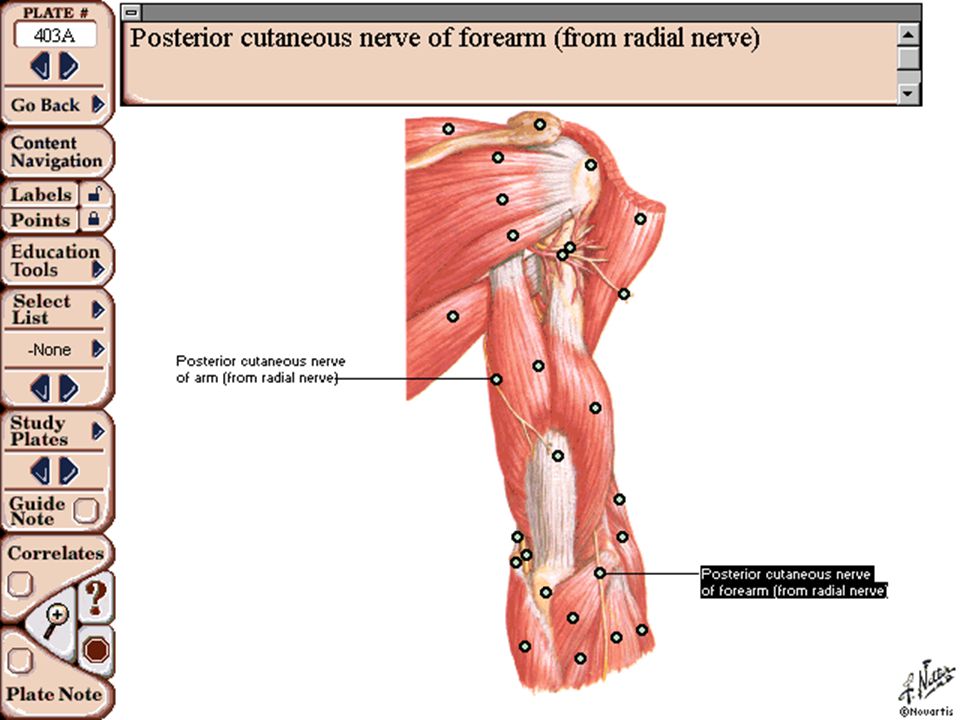
The radial nerve, a continuation of the posterior cord of the brachial plexus, consists of fibers from C6, C7, and C8 and sometimes T1..

104
It is primarily a motor nerve that innervates the triceps, the supinators of the forearm, and the extensors of the wrist, fingers, and thumb.

109
This nerve is injured most often by:
-fractures of the humeral shaft. -Gunshot wounds are the second most common cause of radial nerve injury. Other causes include lacerations of the arm and proximal forearm, - injection injuries, - and prolonged local pressure.

110
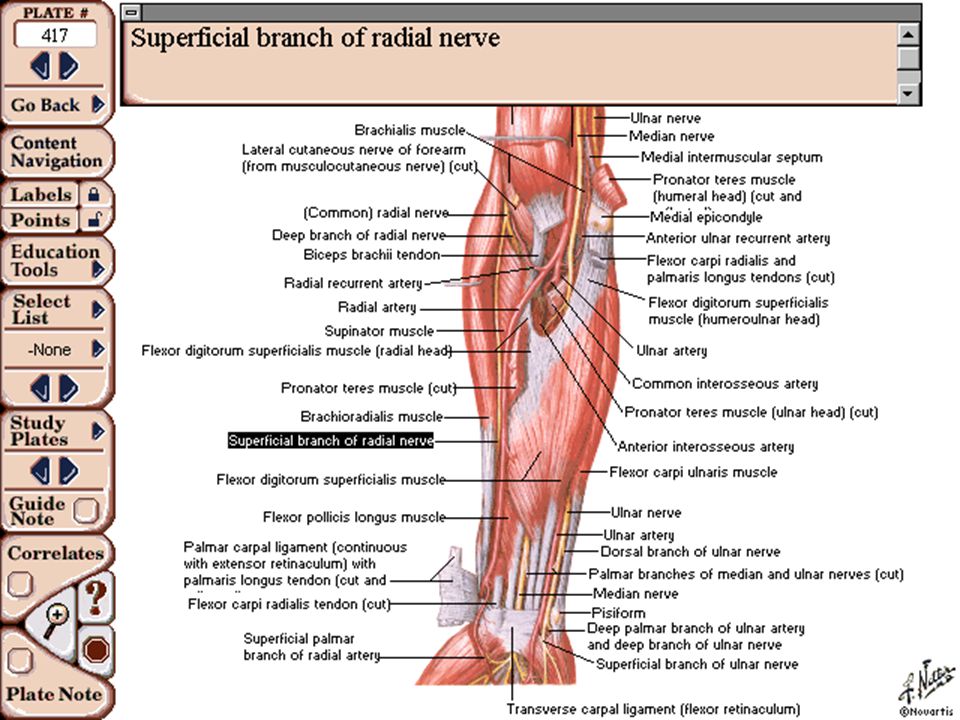
Entrapment syndromes of the radial nerve
-may develop when the nerve or one of its branches is compressed at some point along its course. -Compression of the radial nerve in the arm may be caused by the fibrous arch of the lateral head of the triceps muscle. -The posterior interosseous nerve may be compressed by the fibrous arcade of Frohse, fracture-dislocations or dislocations of the elbow, fractures of the forearm, Volkmann ischemic contracture, neoplasms, enlarged bursae, aneurysms, or rheumatoid synovitis of the elbow. -According to Spinner, posterior interosseous nerve entrapment is of two types. In one type all the muscles supplied by the nerve are completely paralyzed; these include the extensor digitorum communis, extensor indicis proprius, extensor digiti quinti, extensor carpi ulnaris, abductor pollicis longus, and extensor pollicis brevis. In the second type only one or a few of these muscles are paralyzed.

111
radial tunnel syndrome
-entrapment of the posterior interosseous nerve cause chronic and refractory tennis elbow. -can occur at four potentially compressive anatomical structures: the origin of the extensor carpi radialis brevis, adhesions about the radial head, the radial recurrent arterial fan, and the arcade of Frohse as the posterior interosseous nerve enters the supinator. @Lotem et al. found that when symptoms and signs of radial nerve entrapment in the arm develop only after muscular effort, spontaneous recovery can be anticipated. @However, when entrapment is caused by other conditions, especially in the forearm, surgical exploration and decompression of the nerve usually are beneficial. @Compression of the superficial radial nerve causes pain in the forearm and sensory impairment on the dorsum of the thumb. The nerve may be caught in scar tissue at the wrist after surgery or trauma.

112
Examination The following muscles supplied by the radial nerve can be tested accurately because their bellies or tendons or both can be palpated: - the triceps brachii, brachioradialis, - extensors carpi radialis, extensor digitorum communis, extensor carpi ulnaris, - abductor pollicis longus, and - extensor pollicis longus. @ Injury to this nerve results in inability to extend the elbow or supinate the forearm and in a typical wristdrop

114
@The triceps is not seriously affected by injuries of the nerve at the level of the middle of the humerus or distally. @ In injuries of the nerve at its bifurcation into the deep and superficial branches the brachioradialis and the extensor carpi radialis longus continue to function; thus the arm can be supinated and the wrist can be extended.. @Sensory examination is relatively unimportant, even when the nerve is divided in the axilla, because usually there is no autonomous zone.

115
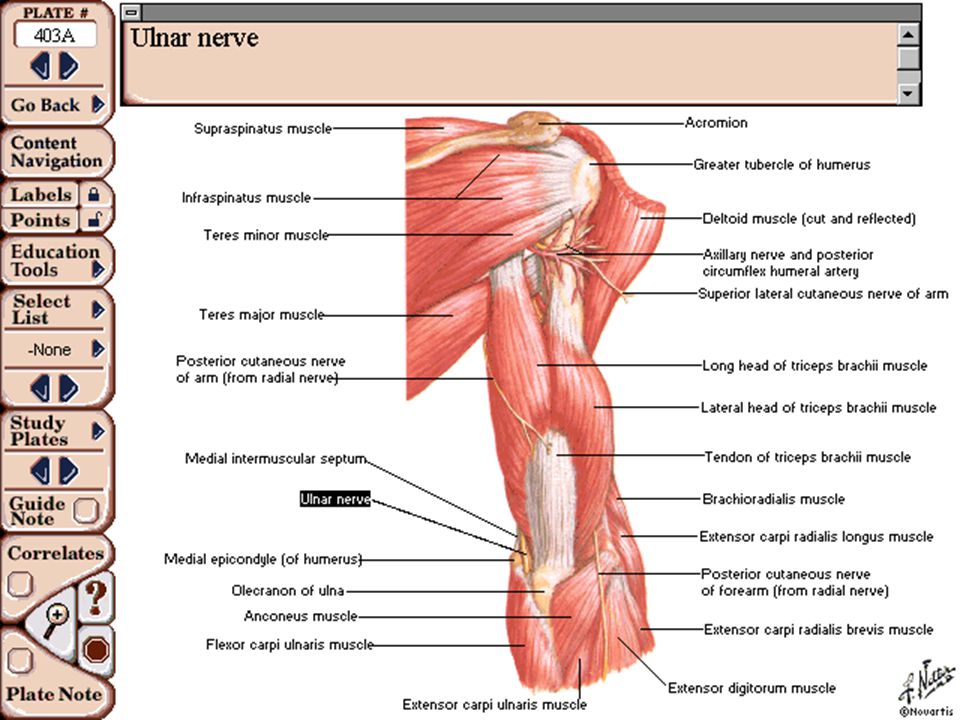
The ulnar nerve is composed of fibers from C8 and T1 coming from the medial cord of the brachial plexus.

131
Injuries: -When it is injured in the upper arm, other nerves or the brachial artery because of their proximity also may be injured. -In the middle of the arm the ulnar nerve is relatively protected,. -in the distal arm and at the elbow it often is injured by dislocations of the elbow and supracondylar and condylar fractures. -The nerve is injured most commonly in the distal forearm and wrist; in these locations it may be injured by gunshot wounds, lacerations, fractures, or dislocations. - In civilian life lacerations cause most of the injuries at the wrist. .

132
Tardy ulnar nerve palsy
may develop after: malunited fractures of the lateral humeral condyle in children, - displaced fractures of the medial humeral epicondyle, -dislocations of the elbow, - contusions of the nerve. - In malunion of the lateral humeral condyle, cubitus valgus develops; in this deformity the ulnar nerve is gradually stretched and can become incompletely paralyzed. -also may develop in patients who have a shallow ulnar groove on the posterior aspect of the medial humeral epicondyle,. - hypoplasia of the humeral trochlea, . - an inadequate fibrous arch that normally keeps the nerve in the groove, resulting in recurrent subluxation or dislocation of the nerve..

133
cubital tunnel syndrome
compression neuropathy of the ulnar nerve about the elbow with no antecedent trauma. - As the ulnar nerve enters the cubital tunnel it is first bordered by the medial epicondyle anteriorly, then by the elbow joint laterally, and finally by the two heads of the flexor carpi ulnaris medially. -In other areas the nerve may be compressed by ligaments, neoplasms, rheumatoid synovitis, aneurysms, vascular thromboses, or anomalous muscles.

134
Postoperative ulnar nerve palsy:
- may result from either direct pressure on the ulnar nerve at the elbow or prolonged flexion of the elbow during surgery. - The ulnar nerve is especially vulnerable to compression when the forearm is allowed to rest in pronation. -Alvine and Schurrer suggested that some patients may have a preexisting subclinical cubital tunnel syndrome that may predispose them to this complication.

135
Examination -Interrupting the ulnar nerve proximal to the elbow is followed by paralysis of:
- the flexor carpi ulnaris, -the flexor profundus to the little and ring fingers, -the lumbricals of the same fingers, - all of the interossei, - the adductor of the thumb, - and all of the short muscles of the little when a nerve is completely divided at this level, the intrinsic muscles of the hand function normally because of anomalous innervation of these muscles by the median nerve. In these instances the fibers that supply the intrinsic muscles may be incorporated in the median nerve down to the middle of the forearm where they leave the median nerve to join the ulnar nerve (Martin- Gruber anastomosis)..
..")
136
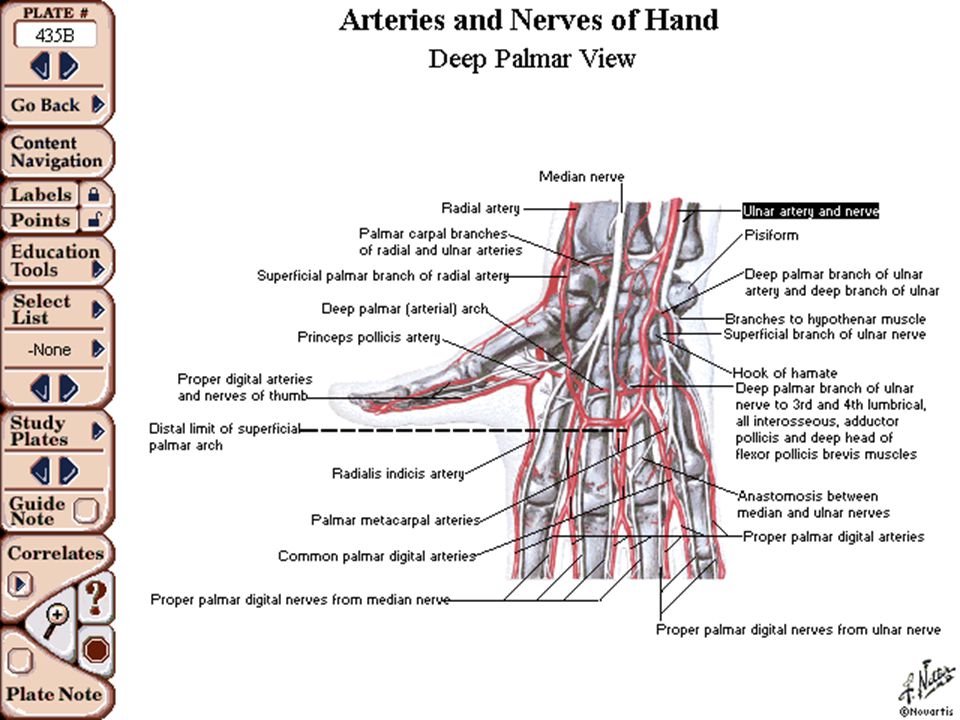
Complete division of the ulnar nerve at the wrist
usually causes paralysis of all ulnar-innervated intrinsic muscles unless an anatomical variation connects the median and ulnar nerves in the palm (Riche-Cannieu anastomosis). Usually when the nerve is divided at the wrist, only the opponens pollicis, the lateral or superficial head of the flexor pollicis brevis, and the lateral two lumbricals remain functional
. Usually when the nerve is divided at the wrist, only the opponens pollicis, the lateral or superficial head of the flexor pollicis brevis, and the lateral two lumbricals remain functional.")
137
- the abductor digiti quinti, and
@In practice only three muscles -the flexor carpi ulnaris, - the abductor digiti quinti, and - the first dorsal interosseus—can be tested accurately. The bellies or tendons (or both) of these muscles may be easily palpated or seen
 of these muscles may be easily palpated or seen.")
138
@Atrophy of the muscles supplied by the ulnar nerve and clawing of the little and ring fingers usually are confirmatory evidence of paralysis of the muscles supplied by this nerve. @ However, if the nerve has been injured proximal to the elbow, clawing of these two fingers may be absent because the flexor digitorum profundus to the ring and little fingers also is denervated. @The sensory examination usually is straightforward, although anatomical variations may cause confusing sensory findings. One need examine only the middle and distal phalanges of the little finger, which make up the autonomous zone of the ulnar nerve . -Complete anesthesia to pinpricks in this area strongly suggests total division of the nerve.

139
@In patients suspected of having cubital tunnel syndrome:
-a positive percussion test over the ulnar nerve at the level of the medial epicondyle - and a positive elbow flexion test are strongly suggestive of a significant compressive neuropathy. -With the elbow fully flexed, the patient will complain of numbness and tingling in the small and ring fingers, often within 1 minute. - Nerve conduction studies are helpful and should demonstrate slowing in the ulnar nerve velocities across the elbow, although normal velocities may be maintained during early involvement. Electromyography may demonstrate fibrillations in the ulnar innervated intrinsic muscles.

140
The treatment for refractory tardy ulnar nerve palsy
- may require removal of the nerve from its groove, neurolysis if necessary, and anterior transposition of the nerve to the flexor surface of the elbow. -Conservative treatment for this syndrome should be attempted before surgical treatment. Patients are instructed to avoid prolonged elbow flexion in the workplace and are given elbow extension splints for sleeping. The splint should not be fitted with the forearm held in pronation because this may aggravate the symptoms. - Towels or pillows secured about the elbow may adequately limit elbow flexion during sleep. -Conservative treatment usually is attempted for a period of 3 months before surgical treatment is considered

141
The surgical treatment of cubital tunnel syndrome :
-includes simple decompression, medial epicondylectomy, and anterior transposition of the ulnar nerve either into a subcutaneous, intramuscular, or submuscular bed . -For a moderate degree of compression the greatest number of excellent results and fewest recurrences were obtained with the submuscular technique. The anterior intramuscular technique yielded the fewest excellent results

142
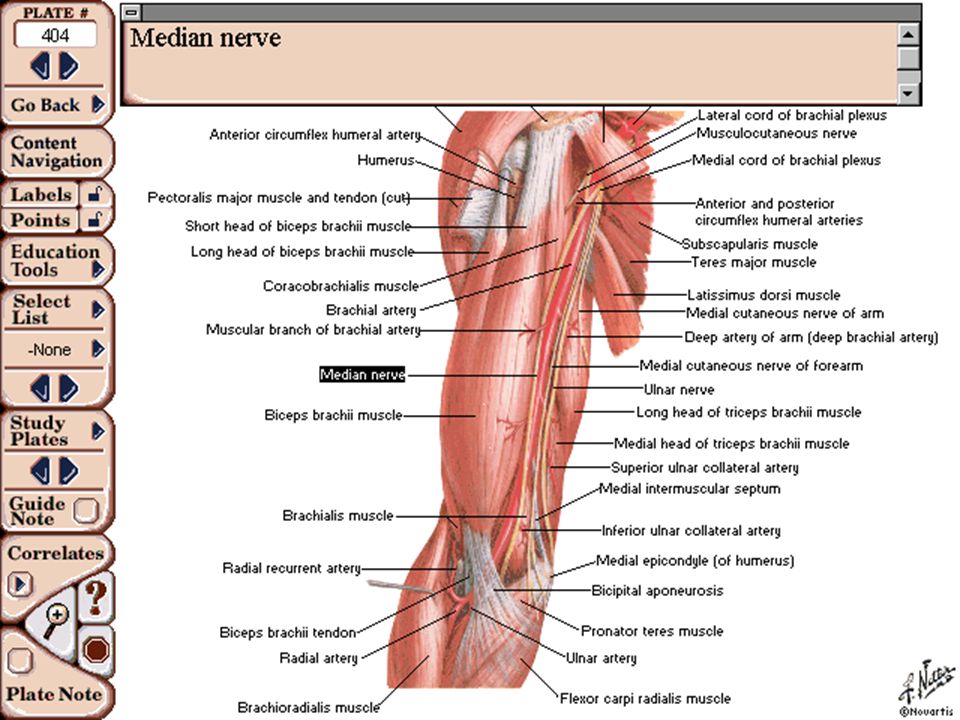
The median nerve, formed by the junction of the lateral and medial cords of the brachial plexus in the axilla, is composed of fibers from C6, C7, C8, and T1

148
Median nerve injuries :
-often result in painful neuromas and causalgia. - From the sensory standpoint they are more disabling than injuries of the ulnar nerve because they involve the digits used in fine volitional activity. -Median nerve injuries often are caused by lacerations, usually in the forearm or wrist. Sunderland pointed out that in: - the upper arm the nerve can be injured by relatively superficial lacerations, excessively tight tourniquets, and humeral fractures, and when it is injured near the axilla, the ulnar and musculocutaneous nerves and the brachial artery also are commonly injured. - In the arm the median nerve may be compressed by the ligament of Struthers. -At the elbow the nerve may be injured in supracondylar fractures and posterior dislocations of the elbow.

149
@Median nerve deficits, as seen in the pronator syndrome, may result from compression of the nerve at the pronator teres, the lacertus fibrosus, or the fibrous flexor digitorum sublimis arch or from anomalies including a hypertrophic pronator teres, a high origin of the pronator teres, fibrous bands within the pronator teres, the median nerve passing posterior to both heads of the pronator teres, or an accessory tendinous arch of the flexor carpi radialis arising from the ulna..

150
@The anterior interosseous nerve may be injured in fractures and lacerations or may be compressed or entrapped by any of the following: the tendinous origins of the flexor digitorum sublimis or the pronator teres, variant muscles such as the palmaris profundus and flexor carpi radialis brevis, tendons from the flexor digitorum sublimis to the flexor pollicis longus, an accessory head of the flexor pollicis longus (Gantzer muscles), an aberrant radial artery, thrombosis of the ulnar collateral vessels, enlargement of the bicipital bursa, or a Volkmann ischemic contracture. @At the wrist the median nerve may be injured by fractures of the distal radius and by fractures and dislocations of the carpal bones.

151
Examination The muscles of the forearm and hand supplied by the median nerve that can be tested with relative accuracy are: the pronator teres, - flexor carpi radialis, - flexor digitorum profundus (index), - flexor pollicis longus, - flexor digitorum sublimis, -and abductor pollicis brevis. @ Substitution movements caused by action of intact muscles may cause confusion during the examination.
, - flexor pollicis longus, - flexor digitorum sublimis, -and abductor pollicis Substitution movements caused by action of intact muscles may cause confusion during the examination.")
152
@ Usually if the forearm can be actively maintained in pronation against resistance, the pronator teres is intact. @ If the wrist can be actively maintained in flexion and a contracting flexor carpi radialis is palpated, this muscle is intact. @Similarly if the interphalangeal joint of the thumb can be maintained in flexion against resistance with the wrist in the neutral position and the thumb adducted, the flexor pollicis longus is functioning. @ The flexor digitorum sublimis to each finger is examined separately while the remaining fingers are held in full passive extension. @ Although opposition of the thumb can be difficult to confirm, if the thumb can be actively maintained in palmar abduction and a contracting abductor pollicis brevis is palpated, this muscle is functioning. @The lumbricals cannot be discretely tested because they cannot be palpated and because their function may be confused with that of the interosseus muscles..

153
According to Spinner, the anterior interosseous syndrome:
-can cause varying signs and symptoms. -Typically, the patient has pain in the proximal forearm lasting for several hours and is found to have weakness or paralysis of the flexor pollicis longus, the flexor digitorum profundus to the index and long fingers, and the pronator quadratus. -When the patient attempts to pinch, active flexion of the distal phalanx of the index finger is impossible.

155
Treatment: In patients who have symptoms of carpal tunnel syndrome and pronator teres syndrome, particular attention should be paid to the nerve conduction studies during preoperative planning. - If the nerve conduction test is positive for carpal tunnel syndrome, we agree in recommending carpal tunnel release in anticipation that the proximal symptoms will resolve. -If the nerve conduction test is negative for carpal tunnel syndrome, we recommend proximal median nerve exploration and proximal decompression as the initial procedure of choice. @. For the anterior interosseous syndrome. If the onset of paralysis has been spontaneous, the initial treatment is nonoperative. Surgical exploration is indicated in the absence of clinical or electromyographic improvement after 12 weeks .

156
PERIPHERAL NERVE INJURYIES

157
MoKazem.com هذه المحاضرة هي من سلسلة محاضرات تم إعدادها و تقديمها من قبل الأطباء المقيمين في شعبة الجراحة العظمية في مشفى دمشق, تحت إشراف د. بشار ميرعلي. الموقع غير مسؤول عن الأخطاء الواردة في هذه المحاضرة. This lecture is one of a series of lectures were prepared and presented by residents in the department of orthopedics in Damascus hospital, under the supervision of Dr. Bashar Mirali. This site is not responsible of any mistake may exist in this lecture. Dr. Muayad Kadhim د. مؤيد كاظم

Similar presentations











































































>")

>")





 Cranial nerve function Motor function Sensory function Cerebellar function Reflex.>")

