Download presentation
Presentation is loading. Please wait.

2
Course 341 MDS Dr Asmaa Faden http://faculty.ksu.edu.sa/Asmaa%20Faden/default.aspx

3
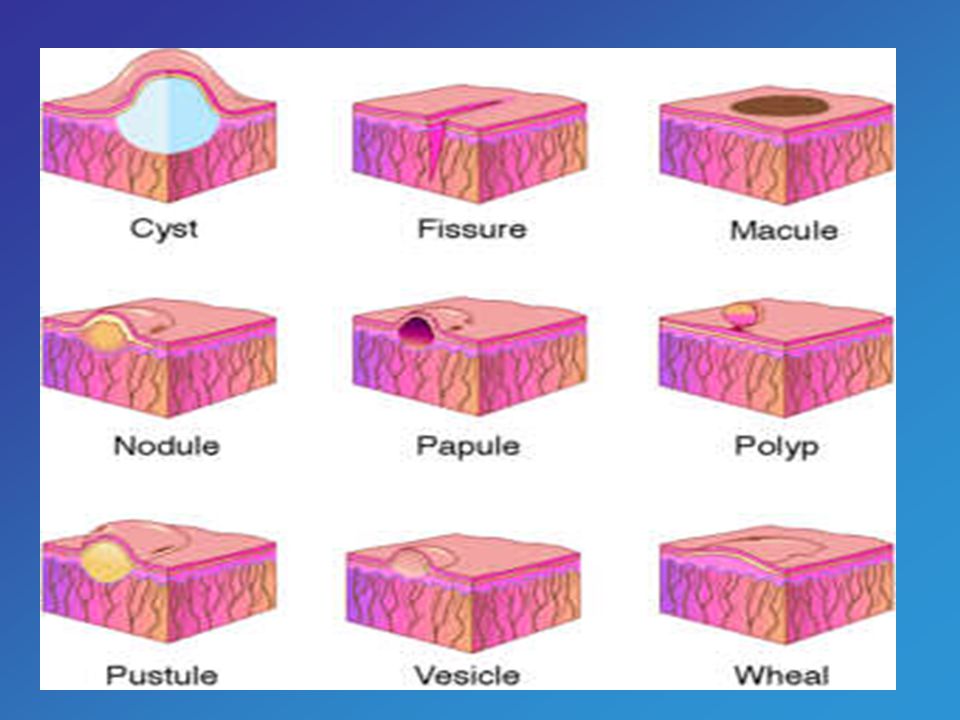
Definitions: Normal mucosa. Vesicle. Bullae. Desquamation.

6
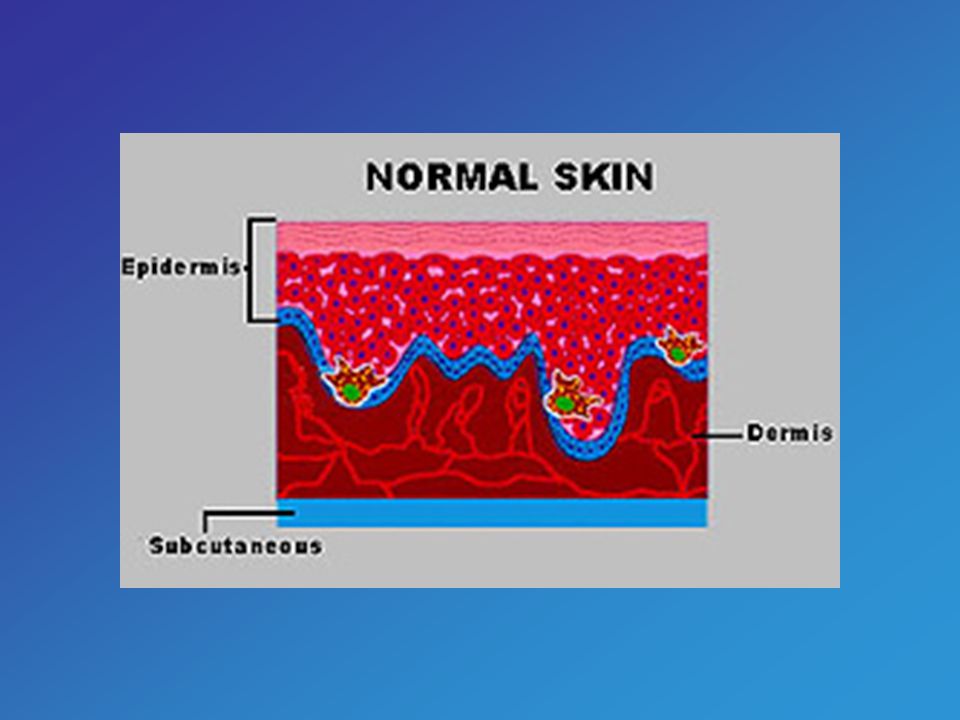
Normal Mucosa: Mucosa is moist tissue that lines some organs and body cavities throughout the body, including your nose, mouth, lungs, and digestive tract. Glands along the mucosa release mucus (a thick fluid).
..")
7
Vesicle: The word vesicle comes from the Latin diminutive vesiculum meaning a small bag or bladder. In dermatology, a vesicle is a small blister, as on the skin. Vesicles also occur on the mucous membranes, such as the buccal mucosa (the lining of the mouth). Vesicles are less than 5 mm in diameter.
. Vesicles are less than 5 mm in diameter..")
8
Bullae: A bulla is a blister more than 5 mm in diameter with thin walls that is full of fluid. In Latin a bulla was a "bubble, stud or knob." It referred to any rounded protrusion, particularly one that was hollow or cystic.

9
Desquamation: The shedding of the outer layers of the skin, for example, once the rash of measels fades, there is desquamation. The word comes from the Latin "desquamare" meaning "to scrape the scales off a fish."

10
Classifications: I - Febrile-associated vesicular eruptions. II - Non-febrile-associated vesicular eruptions. III - Bullous Diseases. IV - Desquamative Lesions.

11
(I) Febrile-associated vesicular eruptions: 1- Herpetic gingivostomatitis. 2- Herpangina. 3- Hand-foot and mouth Disease. 4- Primary Varicella-zoster (Chickenpox). 5- Secondary Varicella-zoster (Shingles).
. 5- Secondary Varicella-zoster (Shingles)..")
12
(II) Non-febrile-associated vesicular e ee eruptions: 1- Recurrent Herpes Stomatitis. 2- Recurrent Herpes Labialis. 3- Contact Vesicular stomatitis. 4- Impetigo.

13
(III) Bullous Diseases: 1- Pemphigus Vulgaris. 2- Bullous Pemphigoid. 3- Benign Mucous Membrane Pemphigoid. 4- Bullous Lichen Planus. 5- Erythema Multiforme. 6- Stevens-Johnson Syndrome. 7- Epidermolysis Bullosa. 8- Dermatitis Herpetiformis.

14
(IV) Desquamative Lesions: 1- Ginigivosis (Desquamative Gingivitis). 2- Erosive Lichen Planus. 3- Toothpaste Idiosyncrasy Lesions.

15
Febrile-Associated Vesicular Eruptions 1- Herpetic Gingivostomatitis: Background: Primary herpetic gingivostomatitis is a relatively common viral infection of the oral mucosa. Age: Children and young adults Clinical Features: - The onset of the disease is abrupt, and is clinically characterized by high fever, headache, malaise, anorexia, irritability, bilateral sensitive regional lymphadenopathy, and sore mouth lesions.

16
1- Herpetic Gingivostomatitis: Clinical Features: cont’d -The affected mucosa is red and edematous, with numerous coalescing vesicles, which rapidly rupture, leaving painful small, round, shallow ulcers covered by yellow fibrin. - New lesions continue to develop during the first three to five days. The ulcers heal in 10–14 days. Both the attached and non-attached oral mucosa may be affected. Gingival lesions are almost always present, resulting in enlargement and edematous and painful erosions.

17
1- Herpetic Gingivostomatitis: Histopathological Descriptions: Intraepithelial vesicle formation. is seen with necrotic exudates and a neutrophilic infiltrate. Differential Diagnosis: - R- Recurrent aphthae (non-febrile and recurrent), herpetic gingivostomatitis is not recurrent intra-orally with the exception of recurrent herpetic stomatitis (microvesicles localized unilaterally on the palatal gingiva). - C- Coxsackie virus (localized to the oropharynx). - S- Shingles (seen in older people, unilateral lesions). - N- Necrotizing ulcerative gingivitis (no vesicles on non-attached mucosa) Management: Symptomatic. In severe cases, systemic acyclovir or valaciclovir.
, herpetic gingivostomatitis is not recurrent intra-orally with the exception of recurrent herpetic stomatitis (microvesicles localized unilaterally on the palatal gingiva). - C- Coxsackie virus (localized to the oropharynx). - S- Shingles (seen in older people, unilateral lesions). - N- Necrotizing ulcerative gingivitis (no vesicles on non-attached mucosa) Management: Symptomatic. In severe cases, systemic acyclovir or valaciclovir..")
18
2- Herpangina Herpangina is an acute self-limiting viral infection, usually caused by coxsackie virus group A, Age: Children. Clinical Features: The disease presents with an acute onset of fever, sore throat, dysphagia, headache, and malaise, followed by diffuse erythema and vesicles. - The disease is contagious, and outbreaks among school-age children.

19
2- Herpangina Clinical Features Cont’d: -T-The vesicles are small and numerous, and rupture rapidly, leaving painful ulcers that heal within 7–10 days. - Characteristically, the lesions appear on the soft palate and uvula, tonsillar pillars, and posterior pharyngeal wall.

20
Febrile-Associated Vesicular Eruptions 2- Herpangina Histopathological Descriptions: Intraepithelial vesicles with an eosinophilic exudates. Nuclear ballooning degeneration of epithelial cells is a feature. Differential Diagnosis: - The limitation of lesions to the soft palate/faucial region is essentially diagnostic. Management: Supportive

21
3- Hand-foot and mouth Disease Hand-foot-and-mouth disease is an acute self-limiting contagious viral infection transmitted from one individual to another. Caused by Coxsackie virus Group A. Age: Children and young adults. Clinical Features: Oral manifestations are always present, and are characterized by small vesicles (5–30 in number) that rapidly rupture, leaving painful, shallow ulcers (2–6 mm in diameter) surrounded by a red halo. The buccal mucosa, tongue, and labial mucosa are the most commonly affected sites.
 that rapidly rupture, leaving painful, shallow ulcers (2–6 mm in diameter) surrounded by a red halo. The buccal mucosa, tongue, and labial mucosa are the most commonly affected sites..")
22
3- Hand-foot and mouth Disease Clinical Features Cont’d: -S-Skin lesions are not constant, and present as small vesicles with a narrow red halo. The lateral borders and the dorsal surfaces of the fingers and toes are the most common areas involved. - Lesions may appear on the palms, soles, and buttocks. The disease lasts five to eight days. The diagnosis is made on the basis of clinical criteria.

23
Febrile-Associated Vesicular Eruptions 3- Hand-foot and mouth Disease Histopathological Descriptions: Intraepithelial vesicles in early stages. Later stages shows shallow ulcerations and erosions of the marginal epithelium. Differential Diagnosis: - Aphthous ulcers, herpes simplex infection, Herpangina. The distribution of lesions in hand-foot and mouth disease is diagnostic. Management: Supportive.

24
4- Primary Varicella-zoster (Chickenpox) Chickenpox is a dermal vesicular exanthema caused by Varicella-zoster virus. Age: Children Clinical Features: -T-The incubation period lasts 2-3 weeks. - The lesions are located primarily on the trunk and face. - Lesions are vesicular with an erythematous boundary, and are extremely pruritic. - Oral manifestations are common, with early onset of vesicles that rapidly rupture leaving erosions covered with pseudomembrane. - The palatal lesions are predominant oral location which resolves within 5-8 days.

25
Febrile-Associated Vesicular Eruptions 4- Primary Varicella-zoster (Chickenpox) Histopathological Descriptions: superficial intraepithelial vesicle is formed. Nuclear ballooning is a feature, inflammatory infiltrate. Differential Diagnosis: - Herpes, Coxsackie viruses and aphthae. Management: Complications are rare, children should be under care of pediatrician. - Oral manifestations treated palliatively.

26
5- Secondary Varicella-zoster (Shingles) Shingle is an acute self-limiting viral disease caused by re-activation of Varicella-zoster virus. Age: Adults and elderly. Sex: slight male predilection. Clinical Features: The virus propagate within ganglia, and the vesicular eruption follows the distribution of the sensory nerves, being segmental and unilateral. -P-Prodromal neuralgia is followed by clustered vesicles eruptions. - Thoracic and abdominal nerves are most frequently involved.

27
Febrile-Associated Vesicular Eruptions 5- Secondary Varicella-zoster (Shingles) Clinical Features Cont’d: the oral mucosa supplied by 2 nd or 3 rd division of the Trigeminal nerve may be the site of infection. -V-Vesicles are unilaterally and stop at the midline and extremely painful. - Post herpetic neuralgia may develop. - Recurrent episodes have been shown to be at risk of lymphoma, leukemia, and carcinogenesis. - Incubation period 1-3 weeks, vesicles may persist 1-5 weeks. n young male adults, HIV should be suspected.

28
Febrile-Associated Vesicular Eruptions 5- Secondary Varicella-zoster (Shingles) Histopathological Descriptions: - Intraepithelial vesicles with nuclear ballooning degeneration. Inflammatory cells infiltration. Differential Diagnosis: -S-Shingles can mimic herpes virus, Coxsackie virus and aphthous stomatitis. - Unilateral segmental distribution, prevalence in adults, sever pain are diagnostic features. - Antibody titers to VZV are elevated. - Systemic malignancy should be ruled out. Management: - Oral infections can be treated palliatively. - Referral to a physician, systemic antiviral. ule out malignancy.

29
(II) Non-febrile-associated vesiculareruptions (II) Non-febrile-associated vesicular eruptions: 1- Recurrent Herpes Stomatitis. 2- Recurrent Herpes Labialis. 3- Contact Vesicular stomatitis. 4- Impetigo.

30
NON-Febrile-Associated Vesicular Eruptions 1- Recurrent Herpes Stomatitis Recurrent herpetic stomatitis is a relatively common oral and perioral disease that is due to reactivation of HSV-1. Age: Young adults Clinical Features: -T-The vesicles are usually restricted to the palatal gingiva unilaterally, present as multiple small vesicles arranged in clusters. -T-The vesicles soon rupture, leaving small painful ulcers that heal within 6–10 days. - Prodromal symptoms are burning, itching, tingling, and erythema.

31
1- Recurrent Herpes Stomatitis Histopathological Descriptions: epithelial small vesicles with nuclear ballooning degeneration. Submucosal inflammatory cells infiltrate. Differential Diagnosis: -R-RHS vesicular eruptions are distributed unilaterally and should be differentiated from Shingles (pain and resolution). - Aphthous (non-attached mucosa). - Herpetic lesions fail to resolve within 4 weeks --- HIV. Management: Symptomatic. NON-Febrile-Associated Vesicular Eruptions
. - Aphthous (non-attached mucosa). - Herpetic lesions fail to resolve within 4 weeks --- HIV. Management: Symptomatic. NON-Febrile-Associated Vesicular Eruptions.")
32
2- Recurrent Herpes Labialis (Cold Sore) - Is a recurrent infection of the lips caused by herpes virus-1. Age: Adults Clinical Features: -V-Vesicles occur in clusters on the vermillion border and adjacent perioral skin of the lips. - Oral cavity is free of lesions. - The vesicles are associated with pain and are unsightly due to the location. - Various factors trigger the infection including: trauma, sunlight exposure. - Persistent herpes Labialis may be indicative of immunocompromised status - HIV NON-Febrile-Associated Vesicular Eruptions

33
2- Recurrent Herpes Labialis (Cold Sore) Histopathological Descriptions: Nuclear ballooning degeneration and submucosal inflammatory infiltrate. Differential Diagnosis: vesicles may be confused with: -I-Impetigo (bacterial infection), contact dermatitis (allergic reaction). - History of trauma, sun exposure, and age will determine diagnosis. Management: -A-Avoid photoactivated dye treatments- carcinogenic transformation ??? - Topical antiviral, topical steroids + antibiotic. NON-Febrile-Associated Vesicular Eruptions
, contact dermatitis (allergic reaction). - History of trauma, sun exposure, and age will determine diagnosis. Management: -A-Avoid photoactivated dye treatments- carcinogenic transformation . - Topical antiviral, topical steroids + antibiotic. NON-Febrile-Associated Vesicular Eruptions.")
34
3- Contact Vesicular Stomatitis: - Immune reaction to allergens contacting oral mucosa manifest vesicles. Clinical Features: - Vesicle do not tend to cluster, accompanied by pain or burning sensation.. - Vesicles arise in areas of allergenic contact (intraoral+ perioral) cosmetics??. - Intraorally:”Topical” Mouth wash, dentifrices, acrylic, topical antibiotics, and foods. - “ Systemic” as shellfish or drugs - The lesions regress within 3-5 days.
 cosmetics . - Intraorally: Topical Mouth wash, dentifrices, acrylic, topical antibiotics, and foods. - Systemic as shellfish or drugs - The lesions regress within 3-5 days..")
35
3- Contact Vesicular Stomatitis: Histopathological Descriptions: Intraepithelial vesicles. Acute inflammatory cells infiltrate. Differential Diagnosis: -P-Primary herpes, hand-foot and mouth disease, erythema multiform (all febrile). - History-- eliminate Management: - Allergen discontinued. ntihistamine. NON-Febrile-Associated Vesicular Eruptions
. - History-- eliminate Management: - Allergen discontinued. ntihistamine. NON-Febrile-Associated Vesicular Eruptions.")
36
4- Impetigo: Is a vesicular eruption on the perioral skin and vermillion border. Caused by staphylococci or a mixed staphylococcal- streptococcal infections. Age: Children Clinical Features: - Oral mucosa NOT affected. - Painful and pruritic. - Contagious- scratch implantation NON-Febrile-Associated Vesicular Eruptions

37
4- Impetigo: Histopathological Descriptions: Intraepithelial vesicles. Submucosa inflammatory cell infiltrate. Differential Diagnosis: -P-Perioral vesicles- differentiated from recurrent herpes labialis and contact dermatitis. - History of herpes, allergen. - Linear tracks of vesicles - suggestive of impetigo. Management: Topical Antibiotic + systemic antibiotic NON-Febrile-Associated Vesicular Eruptions

Similar presentations






.>")





 DNA virus HSV 1 and HSV 2.>")

 1. Introduction and types of diseases. 2. Patients examination.>")


.>")
. Erythema multiforme is a serious of acute, self-limited, recrudescent and inflammatory dermatopathy characterized by erythema,>")

