Download presentation
Presentation is loading. Please wait.

1
Barbara V. Parilla, MD Clinical Professor of Obstetrics and Gynecology University of Illinois at Chicago Director, Maternal Fetal Medicine Advocate Lutheran General Hospital

2
Background cerebral palsy Background cerebral palsy Initial retrospective studies Initial retrospective studies Prospective-randomized trials in detail Prospective-randomized trials in detail Meta-analysis Meta-analysis Hill’s Criteria Hill’s Criteria Molecular mechanism Molecular mechanism Cost-effectiveness Cost-effectiveness Simultaneous tocolysis Simultaneous tocolysis Summary & general recommendations Summary & general recommendations

3
Inexpensive Inexpensive Easy to Administer Easy to Administer Safe Safe Used regularly by OB’s comfortable with it’s use in pre-eclampsia to prevent seizures Used regularly by OB’s comfortable with it’s use in pre-eclampsia to prevent seizures In utero exposure before preterm birth appears to decrease the incidence and severity of cerebral palsy In utero exposure before preterm birth appears to decrease the incidence and severity of cerebral palsy

4
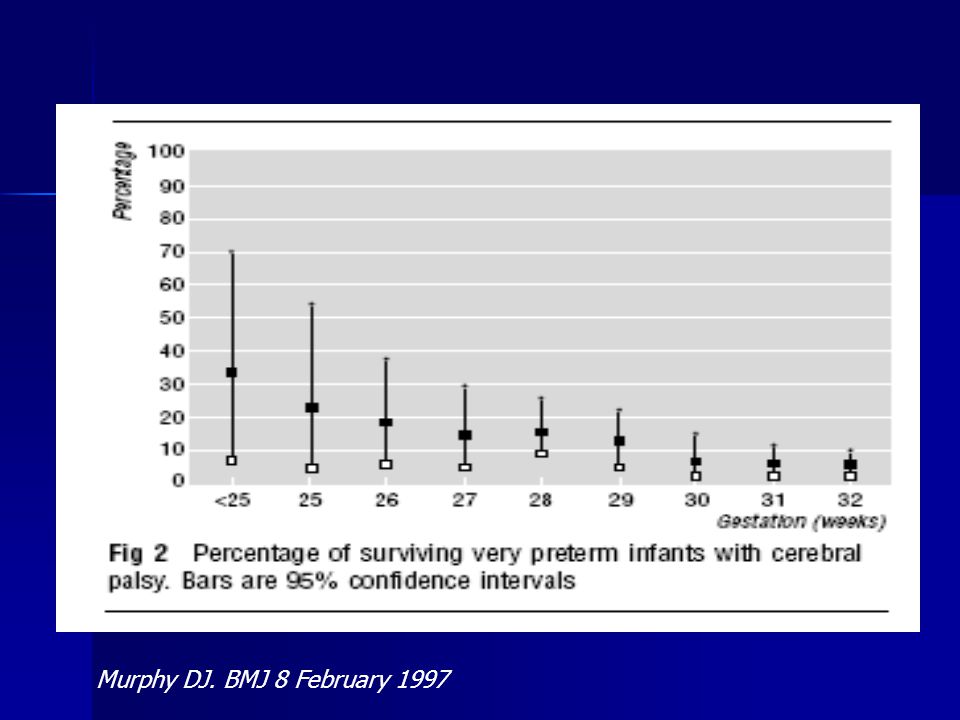
Heterogeneous group of disorders of movement and/or posture Heterogeneous group of disorders of movement and/or posture Most common cause of severe motor disability in childhood Most common cause of severe motor disability in childhood Prevalence 2-3/1,000 live births Prevalence 2-3/1,000 live births Prematurity is a powerful risk factor Prematurity is a powerful risk factor 80x higher among infants 23-27 weeks 80x higher among infants 23-27 weeks Number of children at risk is increasing Number of children at risk is increasing Moster D, Lie RT, Markestad T. Long-term medical and social consequences of preterm birth. N Engl J Med 2008; 359:262.

5
Murphy DJ. BMJ 8 February 1997

7
Case-control study of children with & without CP that were VLBW Case-control study of children with & without CP that were VLBW Children with CP significantly less likely to have been exposed to MgSO 4 Children with CP significantly less likely to have been exposed to MgSO 4 OR 0.14, 95% CI 0.05-0.51 OR 0.14, 95% CI 0.05-0.51 Subsequent observational studies confirmed and refuted findings Subsequent observational studies confirmed and refuted findings MgSO 4 administered as tocolytic or prevention of eclamptic seizure MgSO 4 administered as tocolytic or prevention of eclamptic seizure Nelson KB, Grether JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low birthweight infants? Pediatrics 1995;95:263.

8
RR = incidence in exposed individuals ÷ incidence in unexposed individuals. RR = incidence in exposed individuals ÷ incidence in unexposed individuals. RR can be calculated from studies in which the proportion of patients exposed and unexposed to a risk is known, such as a cohort study. RR can be calculated from studies in which the proportion of patients exposed and unexposed to a risk is known, such as a cohort study. OR = the odds that an individual with a specific condition has been exposed to a risk factor ÷ the odds that a control has been exposed. OR = the odds that an individual with a specific condition has been exposed to a risk factor ÷ the odds that a control has been exposed. OR is used in case-control studies and is often generated in multivariate analyses as well. OR is used in case-control studies and is often generated in multivariate analyses as well. OR provides a reasonable estimate of the RR for uncommon conditions OR provides a reasonable estimate of the RR for uncommon conditions

9
Confidence interval (CI): A point estimate from a sample population may not reflect the "true" value from the entire population. Confidence interval (CI): A point estimate from a sample population may not reflect the "true" value from the entire population. Often helpful to provide a range that is likely to include the true value. A CI is a commonly used estimate. The boundaries of a confidence interval give values within which there is a high probability (95 percent by convention) that the true population value can be found. Often helpful to provide a range that is likely to include the true value. A CI is a commonly used estimate. The boundaries of a confidence interval give values within which there is a high probability (95 percent by convention) that the true population value can be found. The calculation of a CI considers the standard deviation of the data and the number of observations. The calculation of a CI considers the standard deviation of the data and the number of observations. A CI narrows as the number of observations increases, or its variance (dispersion) decreases. A CI narrows as the number of observations increases, or its variance (dispersion) decreases. Statistics
: A point estimate from a sample population may not reflect the true value from the entire population. Often helpful to provide a range that is likely to include the true value. A CI is a commonly used estimate. The boundaries of a confidence interval give values within which there is a high probability (95 percent by convention) that the true population value can be found. Often helpful to provide a range that is likely to include the true value. A CI is a commonly used estimate. The boundaries of a confidence interval give values within which there is a high probability (95 percent by convention) that the true population value can be found. The calculation of a CI considers the standard deviation of the data and the number of observations. The calculation of a CI considers the standard deviation of the data and the number of observations. A CI narrows as the number of observations increases, or its variance (dispersion) decreases. A CI narrows as the number of observations increases, or its variance (dispersion) decreases. Statistics.")
10
The RR and OR are interpreted relative to the number one. The RR and OR are interpreted relative to the number one. OR of 0.6, for example, suggests that patients exposed to a variable of interest were 40 percent less likely to develop a specific outcome compared to the control group. OR of 0.6, for example, suggests that patients exposed to a variable of interest were 40 percent less likely to develop a specific outcome compared to the control group. Similarly, OR of 1.5 suggests that the risk was increased by 50 percent. Similarly, OR of 1.5 suggests that the risk was increased by 50 percent. If the 95% CI crosses 1, it is NOT statistically significant If the 95% CI crosses 1, it is NOT statistically significant Statistics

11
Mittendorf R. Lancet; 11/22/97, Vol. 350 Issue 9090, p1517. 149 maternal randomizations 149 maternal randomizations Randomized 4 arms Randomized 4 arms –Tocolytic PTL <34 wks <4cm (MgSO 4 v “other”- unblinded, switchover to different tocolytic allowed if MgSO 4 failed) 4g load, 2-3 g/h n=46, 47 –Preventive arm- double-blinded PTL>4cm received MgSO 4 or saline n=28 –Primary outcome total paediatric mortality (fetal, neonatal, and post neonatal) and cerebral palsy
 4g load, 2-3 g/h n=46, 47 –Preventive arm- double-blinded PTL>4cm received MgSO 4 or saline n=28 –Primary outcome total paediatric mortality (fetal, neonatal, and post neonatal) and cerebral palsy.")
12
Interim safety monitoring showed 9 paediatric deaths Interim safety monitoring showed 9 paediatric deaths 10 total deaths: 5 singletons, 3 twin pairs where 1 sibling died, 1 twin pair where both died 10 total deaths: 5 singletons, 3 twin pairs where 1 sibling died, 1 twin pair where both died Non-twin deaths ? sequelae infections ? additional tocolysis Non-twin deaths ? sequelae infections ? additional tocolysis Mittendorf R. Lancet; 11/22/97, Vol. 350 Issue 9090, p1517.

13
The Australian Collaborative Trial of Magnesium Sulphate - ACTOMgSO 4 The Australian Collaborative Trial of Magnesium Sulphate - ACTOMgSO 4 1062 women <30 wks expected to deliver <24 hrs 1062 women <30 wks expected to deliver <24 hrs Randomly assigned 4 g load then 1g/hr or placebo for 24 hr max Randomly assigned 4 g load then 1g/hr or placebo for 24 hr max Primary outcomes: rates of total pediatric mortality, cerebral palsy, and combined outcome at 2 yrs (available for 99%) Primary outcomes: rates of total pediatric mortality, cerebral palsy, and combined outcome at 2 yrs (available for 99%) Crowther CA, Hiller JE, Doyle LW, Haslam RR. JAMA 2003;290:2669

14
MgSO 4 v placebo MgSO 4 v placebo Pediatric mortality 13.8 v 17.1 (RR 0.83, 95% CI 0.64-1.09) Pediatric mortality 13.8 v 17.1 (RR 0.83, 95% CI 0.64-1.09) Cerebral Palsy 6.8 v 8.2 (RR 0.83, 95% CI 0.54-1.27) Cerebral Palsy 6.8 v 8.2 (RR 0.83, 95% CI 0.54-1.27) Combined outcome 19.8 v 24 (RR 0.83. 95% CI 0.66-1.03) Combined outcome 19.8 v 24 (RR 0.83. 95% CI 0.66-1.03) Despite lack of statistical significance, potentially clinically important Despite lack of statistical significance, potentially clinically important Crowther CA, Hiller JE, Doyle LW, Haslam RR. JAMA 2003;290:2669
 Combined outcome 19.8 v 24 (RR % CI ) Despite lack of statistical significance, potentially clinically important Despite lack of statistical significance, potentially clinically important Crowther CA, Hiller JE, Doyle LW, Haslam RR. JAMA 2003;290:2669.")
15
When only gross motor function considered MgSO 4 exposed had significantly lower rates 3.4 v 6.6% (RR 0.51, 95% CI 0.29-0.91) When only gross motor function considered MgSO 4 exposed had significantly lower rates 3.4 v 6.6% (RR 0.51, 95% CI 0.29-0.91) Combined outcome gross motor and death 17 v 22.7% (RR 0.75, 95% CI 0.59-0.96) Combined outcome gross motor and death 17 v 22.7% (RR 0.75, 95% CI 0.59-0.96)
 When only gross motor function considered MgSO 4 exposed had significantly lower rates 3.4 v 6.6% (RR 0.51, 95% CI ) Combined outcome gross motor and death 17 v 22.7% (RR 0.75, 95% CI ) Combined outcome gross motor and death 17 v 22.7% (RR 0.75, 95% CI )")
16
Magnesium sulfate tocolysis: time to quit “Intravenous magnesium sulfate tocolysis remains a North American anomaly. This therapy rose to prominence based on poor science and the recommendations of authorities. However, a Cochrane systematic review concluded that magnesium sulfate is ineffective as a tocolytic. The review found no benefit in preventing preterm or very preterm birth. Moreover, the risk of total pediatric mortality was significantly higher for infants exposed to magnesium sulfate (relative risk 2.8; 95% confidence interval 1.2-6.6). Given its lack of benefit, possible harms, and expense, magnesium sulfate should not be used for tocolysis. Any further use of magnesium sulfate for tocolysis should be restricted to formal clinical trials with approval by an institutional review board and signed informed consent for participants. Should tocolysis be desired, calcium channel blockers, such as nifedipine, seem preferable.” “Intravenous magnesium sulfate tocolysis remains a North American anomaly. This therapy rose to prominence based on poor science and the recommendations of authorities. However, a Cochrane systematic review concluded that magnesium sulfate is ineffective as a tocolytic. The review found no benefit in preventing preterm or very preterm birth. Moreover, the risk of total pediatric mortality was significantly higher for infants exposed to magnesium sulfate (relative risk 2.8; 95% confidence interval 1.2-6.6). Given its lack of benefit, possible harms, and expense, magnesium sulfate should not be used for tocolysis. Any further use of magnesium sulfate for tocolysis should be restricted to formal clinical trials with approval by an institutional review board and signed informed consent for participants. Should tocolysis be desired, calcium channel blockers, such as nifedipine, seem preferable.” Grimes D. Obstet Gynecol (Oct 2006) 108(4):986-9
. Given its lack of benefit, possible harms, and expense, magnesium sulfate should not be used for tocolysis. Any further use of magnesium sulfate for tocolysis should be restricted to formal clinical trials with approval by an institutional review board and signed informed consent for participants. Should tocolysis be desired, calcium channel blockers, such as nifedipine, seem preferable. Intravenous magnesium sulfate tocolysis remains a North American anomaly. This therapy rose to prominence based on poor science and the recommendations of authorities. However, a Cochrane systematic review concluded that magnesium sulfate is ineffective as a tocolytic. The review found no benefit in preventing preterm or very preterm birth. Moreover, the risk of total pediatric mortality was significantly higher for infants exposed to magnesium sulfate (relative risk 2.8; 95% confidence interval ). Given its lack of benefit, possible harms, and expense, magnesium sulfate should not be used for tocolysis. Any further use of magnesium sulfate for tocolysis should be restricted to formal clinical trials with approval by an institutional review board and signed informed consent for participants. Should tocolysis be desired, calcium channel blockers, such as nifedipine, seem preferable. Grimes D. Obstet Gynecol (Oct 2006) 108(4):")
17
NICHD/MFMU multicenter placebo controlled trial “beneficial effects of antenatal magnesium sulfate” NICHD/MFMU multicenter placebo controlled trial “beneficial effects of antenatal magnesium sulfate” 2241 women 24-31 wks at risk for imminent delivery 2241 women 24-31 wks at risk for imminent delivery 6 gm load, 2 g/hr 6 gm load, 2 g/hr Infusion stopped after 12 hrs if delivery no longer considered imminent Infusion stopped after 12 hrs if delivery no longer considered imminent F/U available 95.6% children F/U available 95.6% children Rouse DJ, Hirtz DG, Thom E, et al. N Engl J Med. 2008; 359:895.

18
Primary study outcome “stillbirth or infant death by one year corrected age or moderate to severe CP ≥ 2 yrs corrected age” Primary study outcome “stillbirth or infant death by one year corrected age or moderate to severe CP ≥ 2 yrs corrected age” MgSO 4 v placebo 11.3 v 11.7% MgSO 4 v placebo 11.3 v 11.7% Rate of moderate to severe CP 1.9 v 3.5% (RR 0.55, 95% CI 0.32-0.95) Rate of moderate to severe CP 1.9 v 3.5% (RR 0.55, 95% CI 0.32-0.95) Only infants randomized at <28 wks showed a significant reduction in moderate or severe CP Only infants randomized at <28 wks showed a significant reduction in moderate or severe CP Risk of death similar in the 2 groups 9.5 v 8.5 (RR 1.12 95% CI 0.85-1.47) Risk of death similar in the 2 groups 9.5 v 8.5 (RR 1.12 95% CI 0.85-1.47) Suggests that lower rate of CP not simply due to increased death rate in MgSO 4 group Suggests that lower rate of CP not simply due to increased death rate in MgSO 4 group
 Rate of moderate to severe CP 1.9 v 3.5% (RR 0.55, 95% CI ) Only infants randomized at <28 wks showed a significant reduction in moderate or severe CP Only infants randomized at <28 wks showed a significant reduction in moderate or severe CP Risk of death similar in the 2 groups 9.5 v 8.5 (RR % CI ) Risk of death similar in the 2 groups 9.5 v 8.5 (RR % CI ) Suggests that lower rate of CP not simply due to increased death rate in MgSO 4 group Suggests that lower rate of CP not simply due to increased death rate in MgSO 4 group")
19
Enrolled 573 women < 33 wks expected to deliver <24 hrs Enrolled 573 women < 33 wks expected to deliver <24 hrs Single 4 gm loading dose or placebo, no maintenance Single 4 gm loading dose or placebo, no maintenance Infants followed for 2 years after hospital D/C Infants followed for 2 years after hospital D/C Primary outcome was white matter injury on neonatal cranial US Primary outcome was white matter injury on neonatal cranial US Composite outcomes of “CP or death” and “severe motor dysfunction or death” were secondary Composite outcomes of “CP or death” and “severe motor dysfunction or death” were secondary Marret S, Marpeau L, Follet-Bouhamed C, et al. Gynecol Obstet Fertil 2008; 36:278

20
Protective effect of MgSO 4 against “cerebral palsy or death” OR 0.65, 95% CI 0.42-1.03 Protective effect of MgSO 4 against “cerebral palsy or death” OR 0.65, 95% CI 0.42-1.03 Exposure to MgSO 4 was protective against “severe motor dysfunction or death” OR 0.62, 95% CI 0.41-0.93 Exposure to MgSO 4 was protective against “severe motor dysfunction or death” OR 0.62, 95% CI 0.41-0.93 Despite lack of statistical significance, the average size of the reduction is potentially clinically important Despite lack of statistical significance, the average size of the reduction is potentially clinically important Marret S, Marpeau L, Follet-Bouhamed C, et al. Gynecol Obstet Fertil 2008; 36:278

24
Consistency of the association Consistency of the association Strength of the association Strength of the association Dose-response relationship Dose-response relationship Temporal relationship Temporal relationship Biologic plausibility Biologic plausibility Experiment Experiment Coherence Coherence

25
Most prevalent pathologic lesion in CP is peri ventricular white matter (PVWM) injury resulting from vulnerability of immature preoligodendrocytes (POD) <32 weeks Most prevalent pathologic lesion in CP is peri ventricular white matter (PVWM) injury resulting from vulnerability of immature preoligodendrocytes (POD) <32 weeks POD are precursors of myelinating oligidendrocytes which constitute a major glial population in white matter POD are precursors of myelinating oligidendrocytes which constitute a major glial population in white matter Oxidative stress & excitotoxicity from excessive stimulation of ionotropic glutamate receptors on POD are the most prominent molecular mechanism for PVWM injury Oxidative stress & excitotoxicity from excessive stimulation of ionotropic glutamate receptors on POD are the most prominent molecular mechanism for PVWM injury
 injury resulting from vulnerability of immature preoligodendrocytes (POD) <32 weeks Most prevalent pathologic lesion in CP is peri ventricular white matter (PVWM) injury resulting from vulnerability of immature preoligodendrocytes (POD) <32 weeks POD are precursors of myelinating oligidendrocytes which constitute a major glial population in white matter POD are precursors of myelinating oligidendrocytes which constitute a major glial population in white matter Oxidative stress & excitotoxicity from excessive stimulation of ionotropic glutamate receptors on POD are the most prominent molecular mechanism for PVWM injury Oxidative stress & excitotoxicity from excessive stimulation of ionotropic glutamate receptors on POD are the most prominent molecular mechanism for PVWM injury")
26
Recent studies have identified functional N- methyl-D-aspartate (NMDA) glutamatergic receptors in oligodendroglial injury processes Recent studies have identified functional N- methyl-D-aspartate (NMDA) glutamatergic receptors in oligodendroglial injury processes Antagonists of the NMDA receptors for glutamate are potent neuroprotective agents in several animal models of perinatal brain lesions Antagonists of the NMDA receptors for glutamate are potent neuroprotective agents in several animal models of perinatal brain lesions
 glutamatergic receptors in oligodendroglial injury processes Recent studies have identified functional N- methyl-D-aspartate (NMDA) glutamatergic receptors in oligodendroglial injury processes Antagonists of the NMDA receptors for glutamate are potent neuroprotective agents in several animal models of perinatal brain lesions Antagonists of the NMDA receptors for glutamate are potent neuroprotective agents in several animal models of perinatal brain lesions")
27
In addition, MgSO 4 could also reverse the destructive action of oxygen radicals and excitatory amino acids In addition, MgSO 4 could also reverse the destructive action of oxygen radicals and excitatory amino acids Growing evidence suggests MgSO 4 may reverse the harmful effects of hypoxic/ischemic brain damage by blocking the NMDA receptors and, as a calcium antagonist, hindering calcium influx into the cells Growing evidence suggests MgSO 4 may reverse the harmful effects of hypoxic/ischemic brain damage by blocking the NMDA receptors and, as a calcium antagonist, hindering calcium influx into the cells

28
Strong argument for use in women at risk of PTD <32 Strong argument for use in women at risk of PTD <32 Limitations include variations in inclusion & exclusion criteria GA at administration loading and maintenance doses duration of intervention and use of retreatment Limitations include variations in inclusion & exclusion criteria GA at administration loading and maintenance doses duration of intervention and use of retreatment

29
In the placebo arm of the NICHD/MFMU trial, rate of mod-severe CP was 3.5% In the placebo arm of the NICHD/MFMU trial, rate of mod-severe CP was 3.5% Assuming a MgSO 4 effect size of 30%, with 80% power and a 2-tailed alpha of 0.05 Assuming a MgSO 4 effect size of 30%, with 80% power and a 2-tailed alpha of 0.05 Confirmatory trial would require >8000 women 8000 women <32 weeks and 100% F/U of children Enrollment of 2241 mothers in the 20 center NICHD/MFMU Network trial took 10 years and cost $25 million Enrollment of 2241 mothers in the 20 center NICHD/MFMU Network trial took 10 years and cost $25 million

30
The number needed to treat with MgSO 4 is in line with current use of MgSO 4 for other indications The number needed to treat with MgSO 4 is in line with current use of MgSO 4 for other indications Treating 63 women threatening to deliver <32 weeks will prevent 1 case of mod to severe CP Treating 63 women threatening to deliver <32 weeks will prevent 1 case of mod to severe CP If threshold limited to <28 weeks, NICHD MFMU network suggests that only 29 women would need to be treated to prevent 1 case If threshold limited to <28 weeks, NICHD MFMU network suggests that only 29 women would need to be treated to prevent 1 case

31
Services in which calcium channel blockers are primary tocolytic pose a dilemma Services in which calcium channel blockers are primary tocolytic pose a dilemma Choices include MgSO 4 primary tocolytic (not efficacious) Indomethacin Continue to use calcium channel blockers and MgSO 4 simultaneously and risk hypotension (not recommended) Choices include MgSO 4 primary tocolytic (not efficacious) Indomethacin Continue to use calcium channel blockers and MgSO 4 simultaneously and risk hypotension (not recommended)
 Indomethacin Continue to use calcium channel blockers and MgSO 4 simultaneously and risk hypotension (not recommended) Choices include MgSO 4 primary tocolytic (not efficacious) Indomethacin Continue to use calcium channel blockers and MgSO 4 simultaneously and risk hypotension (not recommended)")
32
144 echos 44 pregnancies 17/60 fetus =28% KJ Moise AJOG 1993;168:1350-3

33
llAll reversible!

34
Indomethacin was the only drug in this review associated with a decrease in preterm birth and birth weight < 2500 g.

35
For women at risk of PTB we suggest antenatal administration of MgSO 4 For women at risk of PTB we suggest antenatal administration of MgSO 4 Randomized placebo-controlled trials of maternal administration of MgSO 4 in women expected to have a PTD within 24 hrs have consistently demonstrated a decrease of CP and severe motor dysfunction in offspring Randomized placebo-controlled trials of maternal administration of MgSO 4 in women expected to have a PTD within 24 hrs have consistently demonstrated a decrease of CP and severe motor dysfunction in offspring However, the possibility of an increased risk of death in a sub group of fetuses or infants has not conclusively been excluded However, the possibility of an increased risk of death in a sub group of fetuses or infants has not conclusively been excluded

36
In the United States, 2% of women deliver <32 weeks. If MgSO 4 was uniformly administered to the 75% of women who deliver spontaneously and it was as effective as in the NICHD/MFMU Network trial, then more than 1000 fewer children a year would suffer from handicapping CP In the United States, 2% of women deliver <32 weeks. If MgSO 4 was uniformly administered to the 75% of women who deliver spontaneously and it was as effective as in the NICHD/MFMU Network trial, then more than 1000 fewer children a year would suffer from handicapping CP “For their sake, we should avail ourselves of this opportunity” “For their sake, we should avail ourselves of this opportunity” Dwight J Rouse. AJOG June 2009

37
ACOG Committee Opinion Number 455 March 2010 “The Committee on Obstetric Practice and SMFM recognize that none of the individual studies found a benefit with regard to their primary outcome. However, the available evidence suggests that MgSO 4 given before anticipated early preterm birth reduces the risk of CP in surviving infants” “The Committee on Obstetric Practice and SMFM recognize that none of the individual studies found a benefit with regard to their primary outcome. However, the available evidence suggests that MgSO 4 given before anticipated early preterm birth reduces the risk of CP in surviving infants”

38
Inclusion criteria, treatment regimens, large trials Study Total # InclusionDoseDuration Death & CP DeathCP Crowther1,255 <30 wks likely deliv 24h 4 g load 1 g/hr Up to 24 hr RR 0.83 0.66-1.03 RR 0.83 0.64-1.09 RR 0.83 0.54-1.27 Marret688 <33 wks 4 g load only Loading dose only OR 0.80 0.58-1.10 OR 0.85 0.55-1.32 OR 0.70 0.41-1.19 Rouse2,241 24-31 wks high risk SPTB 6 g load 2 g/hr Up to 12 hrs; retreat when deliv imminent RR 0.97 0.77-1.23 RR 1.12 0.85-1.47 RR 0.55 0.32- 0.95

39
MgSO 4 administered when imminent delivery from either PPROM or intact preterm seems likely, or before an indicated PTD MgSO 4 administered when imminent delivery from either PPROM or intact preterm seems likely, or before an indicated PTD We limit to 24-32 weeks We limit to 24-32 weeks 4-6 gram load, 2 gm/hr 4-6 gram load, 2 gm/hr Therapy discontinued by 24 hours if delivery has not occurred Therapy discontinued by 24 hours if delivery has not occurred If tocolysis indicated, we use indomethacin If tocolysis indicated, we use indomethacin We retreat for women who do not deliver after an initial course of therapy We retreat for women who do not deliver after an initial course of therapy

40
Rescue Steroids GA < 33 weeks GA < 33 weeks Single course given < 30 weeks Single course given < 30 weeks > 2 weeks ago > 2 weeks ago Delivery considered likely Delivery considered likely Garite TJ. AJOG March 2009

41
Barbara.Parilla@advocatehealth.com

Similar presentations

>")

















>")