Download presentation
Presentation is loading. Please wait.

1
Aero-digestive Endoscopy Dr. Vishal Sharma

2
History

3
Bozzini (1806): angled speculum with mirror using wax candle, first examined larynx Manuel Garcia (1854): Using dental mirror, hand mirror & sunlight visualized his own vocal cords Adolph Kussmaul (1868): 1 st rigid esophagoscopy Gustav Killian (1897): 1 st rigid bronchoscopy Chevalier Jackson (early 1900s): father of modern rigid endoscopy Oscar Kleinsasser (1960): suspension micro-laryngoscope Shigeto Ikeda (1966): first fiberoptic bronchoscopy & oesophagoscopy H.H. Hopkins: rigid fiberoptic telescopes

4
Adolph Kussmaul

5
Gustav Killian

6
Chevalier Jackson

7
Shigeto Ikeda

8
Direct Laryngoscopy

9
Chevalier Jackson’s Direct Laryngoscope

10
Anterior commissure Direct Laryngoscope

11
Boyce’s Endoscopy position Supine position with head elevated by 10 cm

12
Tongue Base visualized

13
Epiglottis visualized

14
Vocal cords visualized

15
Micro-laryngoscopy

16
Kleinsasser Microlaryngoscope

17
Chest Piece

18
Laryngoscope fixed

19
Microscope focused

20
Indications for Laryngoscopy

21
Diagnostic Therapeutic Biopsy of suspected malignancy Foreign body in larynx & pyriform fossa removal (larynx & pyriform fossa) Examination of hidden areas: Excision biopsy anterior commissure, laryngeal of benign ventricle, subglottis, infrahyoid laryngeal lesion epiglottis, pyriform fossa apex Dilatation of laryngeal stricture Unsuccessful indirect laryngoscopy
 Examination of hidden areas: Excision biopsy anterior commissure, laryngeal of benign ventricle, subglottis, infrahyoid laryngeal lesion epiglottis, pyriform fossa apex Dilatation of laryngeal stricture Unsuccessful indirect laryngoscopy")
22
Micro-laryngoscopyDirect Laryngoscopy Binocular visionMonocular vision Better illuminationLess illumination MagnificationNo magnification Better precisionLess precision Both hands are free1 hand holds scope Video attachment possibleNo Can be combined with microscopic Laser No

23
Rigid Bronchoscopy

24
Rigid Bronchoscope

25
Close-up of proximal end

26
Bronchoscope introduced

27
At laryngeal inlet

28
Epiglottis identified

29
Vocal cords identified

30
Scope passed through glottis after 90 0 rotation

31
Scope rotated back

32
Tracheal rings identified

33
Carina identified

34
Bronchopulmonary segments

35
Endoscopy position

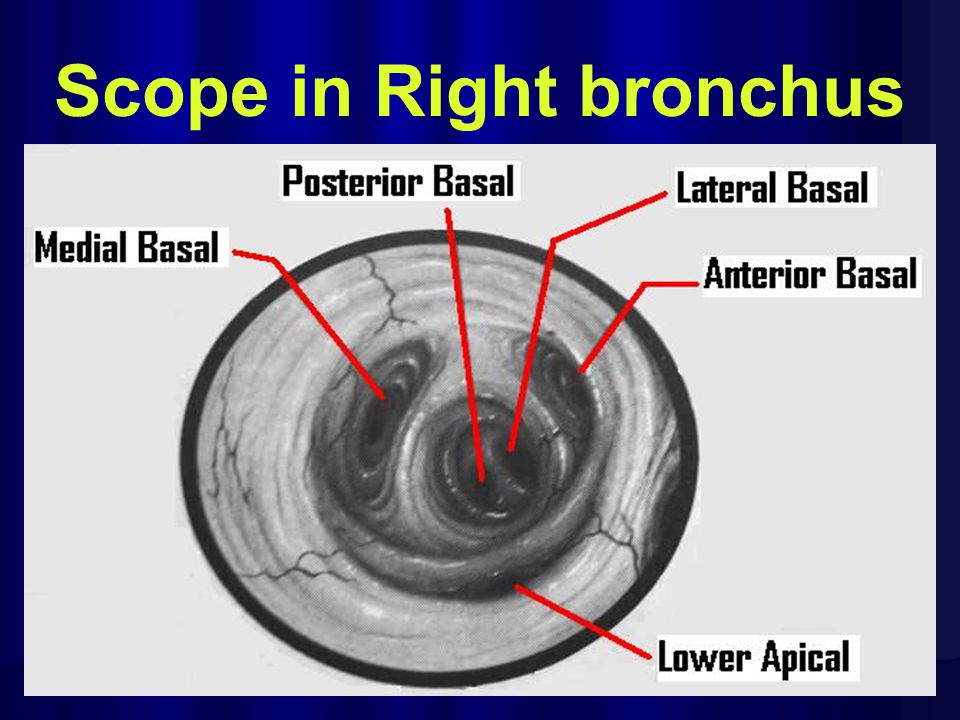
36
Scope in Right bronchus

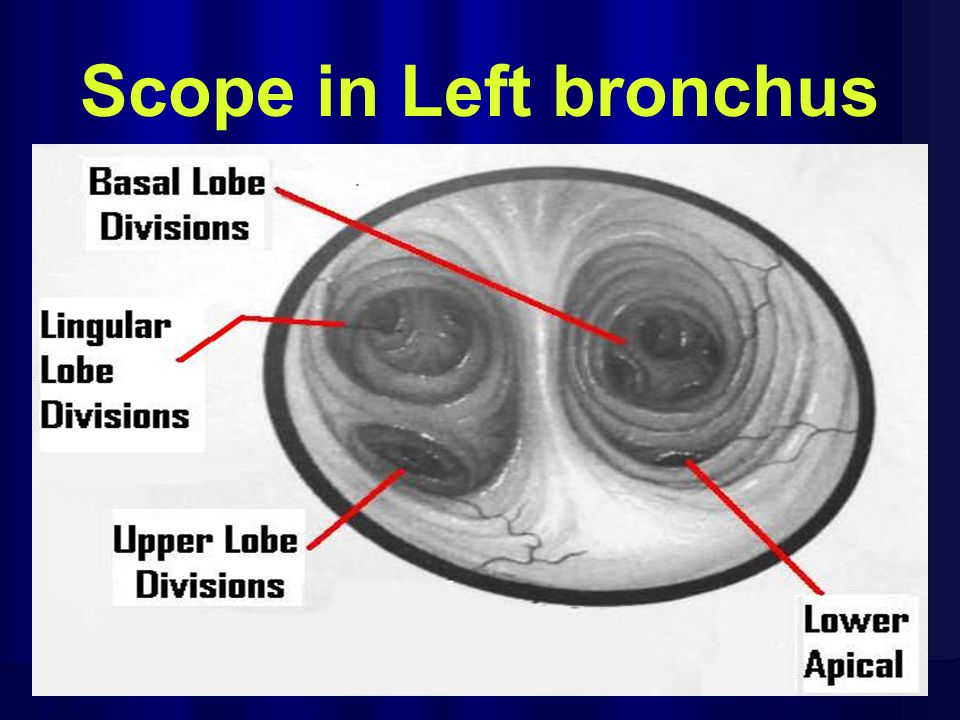
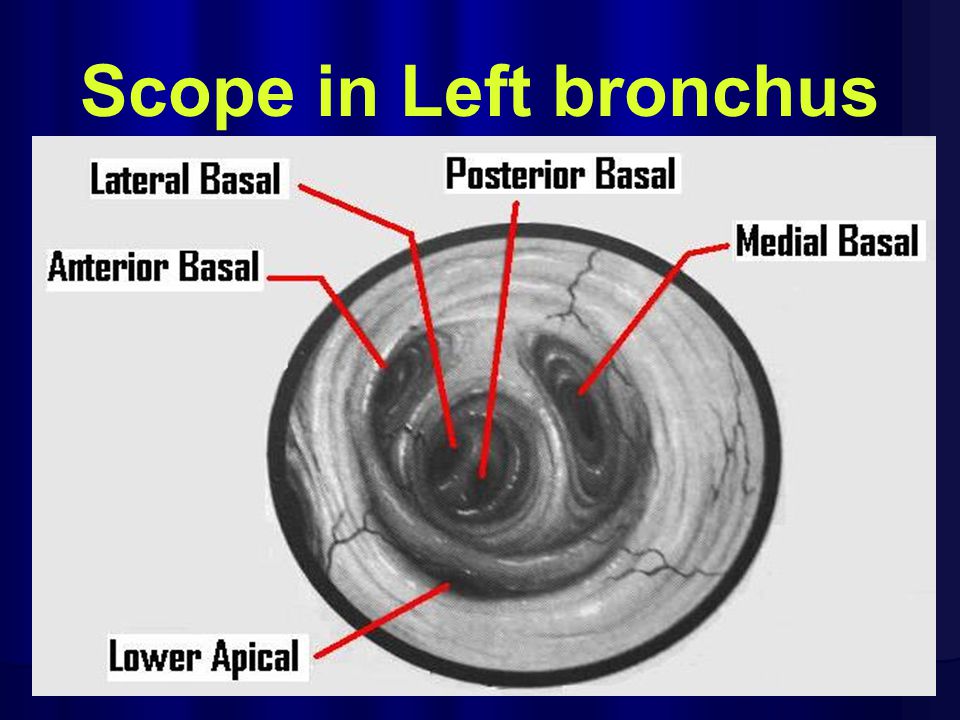
39
Scope in Left bronchus

42
Flexible Bronchoscope

43
Indications for Bronchoscopy 1.Broncho-alveolar lavage for C/S, AFB, cytology 2.Biopsy of tracheo-bronchial tumours 3.Investigation of chronic cough, hemoptysis, Lt vocal cord palsy, atelectasis, obstructive emphysema, mediastinal growths 4.Removal tracheo-bronchial of foreign bodies 5.Removal of retained respiratory secretions

44
Rigid BronchoscopyFlexible Also functions as airwayNo Better for removal of foreign bodyNo Allows use of LaserNo Visualizes up to 3 rd bronchial division5 th division Not done under local anesthesiaDone Not done in cervical spine problemsDone More risky & traumaticSafer Not done for trans-bronchoscopic biopsyDone

45
Rigid Oesophagoscopy

46
Rigid Oesophagoscope

47
Jackson scopeNegus scope Distal illuminationProximal illumination No markingsMarked NarrowBroad Constant diameterTapered Single bulbDouble bulb

48
Epiglottis visualized

49
Right pyriform fossa

50
Cricopharyngeal sphincter

51
Upper Oesophagus

52
Middle Oesophagus

53
Lower Oesophagus

54
Indications for Oesophagoscopy 1. Investigation of dysphagia, haematemesis, GERD, neck node metastasis of unknown origin 2. Oesophageal foreign body removal 3. Excision biopsy of benign oesophageal lesions 4. Dilatation of oesophageal strictures 5. Sclerotherapy for oesophageal varices 6. Insertion of palliative oesophageal feeding tube

55
Rigid OesophagoscopyFlexible Better for cricopharynx examinationNo Better for removal of foreign bodyNo Allows use of LaserNo Not good for lower oesophageal examnGood Not done under local anesthesiaDone Not done in cervical spine problemsDone More risky & traumaticSafer

56
Thank You

Similar presentations





 and variable length (20-40 cm).These instruments usually have illumination.>")


 Internal trauma (Endotracheal intubation, tracheostomy) Other ▪ Systemic diseases (vasculitis,>")


; PGD (BIOETHICS)>")






 ภาควิชาวิสัญญีวิทยา วิทยาลัยแพทยศาสตร์ กรุงเทพมหานครและวชิรพยาบาล.>")

