Download presentation
Presentation is loading. Please wait.

1
MANAGEMENT OF RUPTURED HEPATOCELLULAR CARCINOMA Joint Hospital Surgical Grand Round 19 th July 2014 Dr. SC Tam United Christian Hospital

2
Introduction Hepatocellular carcinoma is the 5 th common cause of malignancy in the World Hong Kong Cancer Registry 2011: 10 most common cancer10 most common cancer death

3
Ruptured HCC Occurs in 3-15% of patients with HCC Asian > Western Decreasing incidence Causes: Spontaneous (most common) Post-treatment Trauma Mortality rate in acute phrase 25-75% Third leading cause of HCC-related death Liu, et al. J Clin Oncol 2001

4
Mechanism of ruptured Rapid growth of tumour Tumour necrosis Erosion to vessels Hepatic venous thrombosis Coagulopathy

5
Risk factors Zhu, et al: World J Gastroenterol 2012

6
Clinical presentation Letchumanan, et al: Med J Malaysia 2013 PresentationPercentage Known HCC39% Abdominal pain86% Shock42% Liu, et al. J Clin Oncol 2001

7
Diagnosis Computed tomography/ Ultrasound Abdominal paracentesis Emergency laparotomy (20%)
")
8
What? Who? When? How? Ruptured HCC

9
What? Who? When? How? Ruptured HCC

10
Treatment aim Stabilize the patient Resuscitation Correct coagulopathy Achieve haemostasis Minimize damage to normal liver parenchyma Identify ways to lengthen survival Palliation

11
Management strategy Conservative Transcatheter arterial embolization (TAE) Surgical haemostasis
 Surgical haemostasis")
12
What? Who? When? How? Ruptured HCC

13
Do something vs. do nothing? The more we do, the better?

14
Do little? 63/508 (12%) admitted for ruptured HCC 16/63 (25%) underwent conservative management 100% in patient mortality Chearanai, et al. Cancer 1983
 admitted for ruptured HCC 16/63 (25%) underwent conservative management 100% in patient mortality Chearanai, et al. Cancer")
15
Do more? Lai, et al. Arch Surg 2006

16
Conservative management Period 1 vs. period 2 Intervene when: Unstable Signs of continuous bleeding Not considered “terminal” Period 1Period 2 Conservative8%69% Mortality62%51% Median survival7 days12 days Mortality (not “terminal”)60%35% Median survival (not “terminal”)8 days72 days Leung, et al. Arch Surg 1999
60%35% Median survival (not terminal )8 days72 days Leung, et al. Arch Surg")
17
Conservative management Advanced malignancy, poor pre-morbid state Poor liver function Stable patient with no signs of continuous bleeding

18
What? Who? When? How? Ruptured HCC

19
Surgical haemostasis Open surgical method was mainstay of treatment in 60s to 80s Perihepatic packing Plication of bleeder Ligation of hepatic artery (ipsilateral/ common) Injection of alcohol Radiofrequency ablation Tumour resection No large study comparing different technique Surgeon’s preference depending on situation
 Injection of alcohol Radiofrequency ablation Tumour resection No large study comparing different technique Surgeon’s preference depending on situation")
20
Transcatheter arterial embolization Gained popularity since 90s Injection of Gelfoam (absorbable) Achieve haemostasis >70% Contraindicated: Portal vein thrombosis Arteriovenous shunting Technical difficulty Bilirubin > 50umol/L
 Achieve haemostasis >70% Contraindicated: Portal vein thrombosis Arteriovenous shunting Technical difficulty Bilirubin > 50umol/L")
21
Transcatheter arterial embolization High success rate: 4/35 (11%) failed TAE Better survival 10/35 (29%) died of liver failure in 1 month Median survival 5.6 weeks Liu, et al. J Clin Oncol 2001 Lai, et al. Archi Surg 2006

22
Algorithm Terminal, poor liver function Cheung, et al. PLoS One 2014

23
Radiofrequency ablation Cheung, et al. PLoS One 2014

24
Radiofrequency ablation Cheung, et al. PLoS One 2014 Overall Had surgery TACE Conservative

25
What? Who? When? How? Ruptured HCC

26
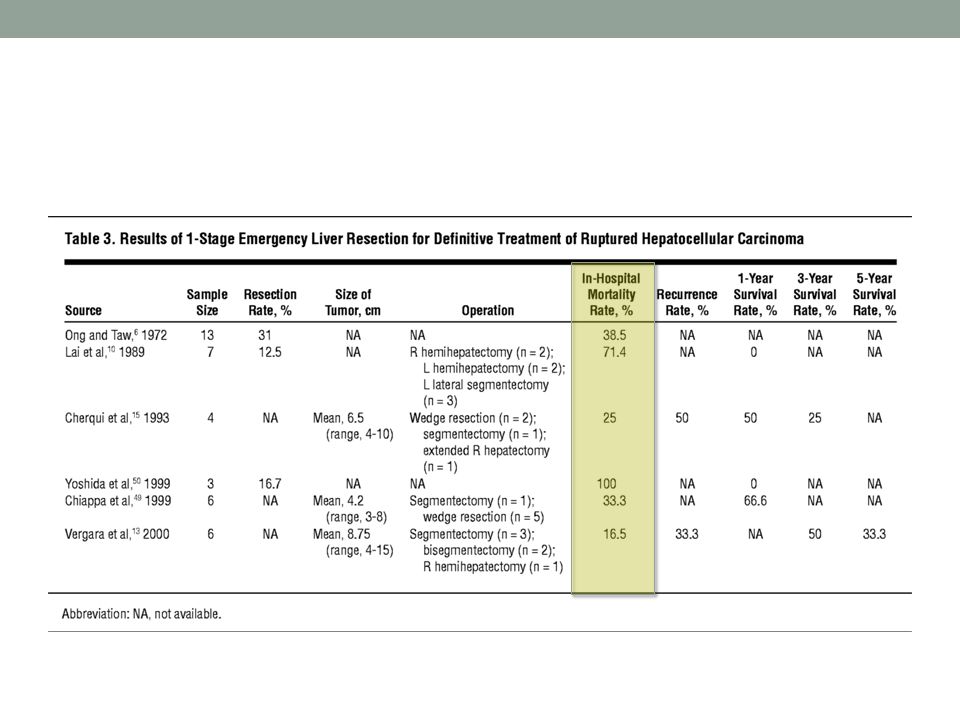
Definitive treatment of HCC 1-stage emergency liver resection vs. staged operation

27
Emergency liver resection High mortality rate 16.5%-100% Highly controversial Only in highly selected patients ProsCons Stop the bleeding Definite treatment No delay ?Hepatic reserve Worsening of liver function Coagulopathy Occult tumour nodules

28
Lai, et al. Archi Surg 2006

29
Prognosis Prognostic factors: Pre-ruptured disease state Liver function Child-Puge score/ Bilirubin Severity of haemorrhage (shock/ haemoglobin level) Median survival 8.9 weeks 30-day mortality 38% Liu, et al. J Clin Oncol 2001

30
Staged liver resection Eligible ~21%-56% of cases Lai, et al. Archi Surg 2006

31
Staged liver resection RupturedNot ruptured Survival1-year57.1%77.1% 3-year19.0%59.8% 5-year7.6%41.2% Disease-free survival1-year27.6%57.1% 3-year14.3%40.6% 5-year3.8%32.9% Zhu, et al. World J Gastroenterol 2012

32
Summary Rupture HCC is uncommon but highly fatal Aim of treatment: Stabilization and achieve haemostasis Often definitive management to selected patients Treatments do not alter outcome in patients with advanced malignancy and poor liver function Radiofrequency ablation is new and promising Staged liver resection > 1-stage emergency resection Prognosis is poor Correct management improves survival

33
Definite treatment/ staged liver resection TAE Conservative Surgery Unstable Continuous bleeding Failed Haemostasis Summary

34
Reference 1. Ngan H, Tso WK, Lai CL, et al: The role of hepatic arterial embolization in the treatment of spontaneous rupture of hepatocellular carcinoma. Clin Radiol 1998;53(5):338-41 2. Liu CL, Fan ST, Lo CM, et al: Management of spontaneous rupture of hepatocellular carcinoma: single-center experience. J Clin Oncol 2001;19(17):3725-32 3. Lai EC, Lau WY: Spontaneous rupture of hepatocellular carcinoma: a systematic review. 2006;Arch Surg 141(2):191-8 4. Kirikoshi H, Saito S, Yoneda M, et al: Outcome and factors influencing survival in cirrhotic cases with spontaneous rupture of hepatocellular carcinoma: a multicenter study. BMC Gastroenterol 2009;9:29 5. Rossetto A, Adani GL, Risaliti A, et al: Combined approach for spontaneous rupture of hepatocellular carcinoma. World J Hepatol 2010;2(1):49-51 6. Bassi N, Caratozzolo E, Bonariol L, et al: Management of ruptured hepatocellular carcinoma: implications for therapy. World J Gastroenterol 2010;16(10):1221-5 7. Kim JY, Lee JS, Oh DH, et al: Transcatheter arterial chemoembolization confers survival benefit in patients with a spontaneously rupturedhepatocellular carcinoma. Eur J Gastroenterol Hepatol 2012;24(6):640-5 8. Zhu Q, Li J, Yan JJ, et al: Predictors and clinical outcomes for spontaneous rupture of hepatocellular carcinoma. World J Gastroenterol 2012;18(48):7302-7 9. Jin YJ, Lee JW, Park SW, et al: Survival outcome of patients with spontaneously ruptured hepatocellular carcinoma treated surgically or by transarterial embolization. World J Gastroenterol 2013;19(28):4537-44 10. Letchumanan VP, Lim KF, Mohamad AB : Diagnosis and management of ruptured hepatoma: single center experience over 10 years. Med J Malaysia 2013;68(5):405-9 11. Cheung TT, Poon RT, Chok KS, et al: Management of spontaneously ruptured hepatocellular carcinomas in the radiofrequency ablation era. PLoS One 2014;9(4):e94453 12. Leung KL, Lau WY, Lai PBS, et al: Spontaneous rupture of hepatocellular carcinoma: conservative management and selective intervention. Arch Surg 1999;134(10):1103-7
: Liu CL, Fan ST, Lo CM, et al: Management of spontaneous rupture of hepatocellular carcinoma: single-center experience. J Clin Oncol 2001;19(17): Lai EC, Lau WY: Spontaneous rupture of hepatocellular carcinoma: a systematic review. 2006;Arch Surg 141(2): Kirikoshi H, Saito S, Yoneda M, et al: Outcome and factors influencing survival in cirrhotic cases with spontaneous rupture of hepatocellular carcinoma: a multicenter study. BMC Gastroenterol 2009;9:29 5. Rossetto A, Adani GL, Risaliti A, et al: Combined approach for spontaneous rupture of hepatocellular carcinoma. World J Hepatol 2010;2(1): Bassi N, Caratozzolo E, Bonariol L, et al: Management of ruptured hepatocellular carcinoma: implications for therapy. World J Gastroenterol 2010;16(10): Kim JY, Lee JS, Oh DH, et al: Transcatheter arterial chemoembolization confers survival benefit in patients with a spontaneously rupturedhepatocellular carcinoma. Eur J Gastroenterol Hepatol 2012;24(6): Zhu Q, Li J, Yan JJ, et al: Predictors and clinical outcomes for spontaneous rupture of hepatocellular carcinoma. World J Gastroenterol 2012;18(48): Jin YJ, Lee JW, Park SW, et al: Survival outcome of patients with spontaneously ruptured hepatocellular carcinoma treated surgically or by transarterial embolization. World J Gastroenterol 2013;19(28): Letchumanan VP, Lim KF, Mohamad AB : Diagnosis and management of ruptured hepatoma: single center experience over 10 years. Med J Malaysia 2013;68(5): Cheung TT, Poon RT, Chok KS, et al: Management of spontaneously ruptured hepatocellular carcinomas in the radiofrequency ablation era. PLoS One 2014;9(4):e Leung KL, Lau WY, Lai PBS, et al: Spontaneous rupture of hepatocellular carcinoma: conservative management and selective intervention. Arch Surg 1999;134(10):")
36
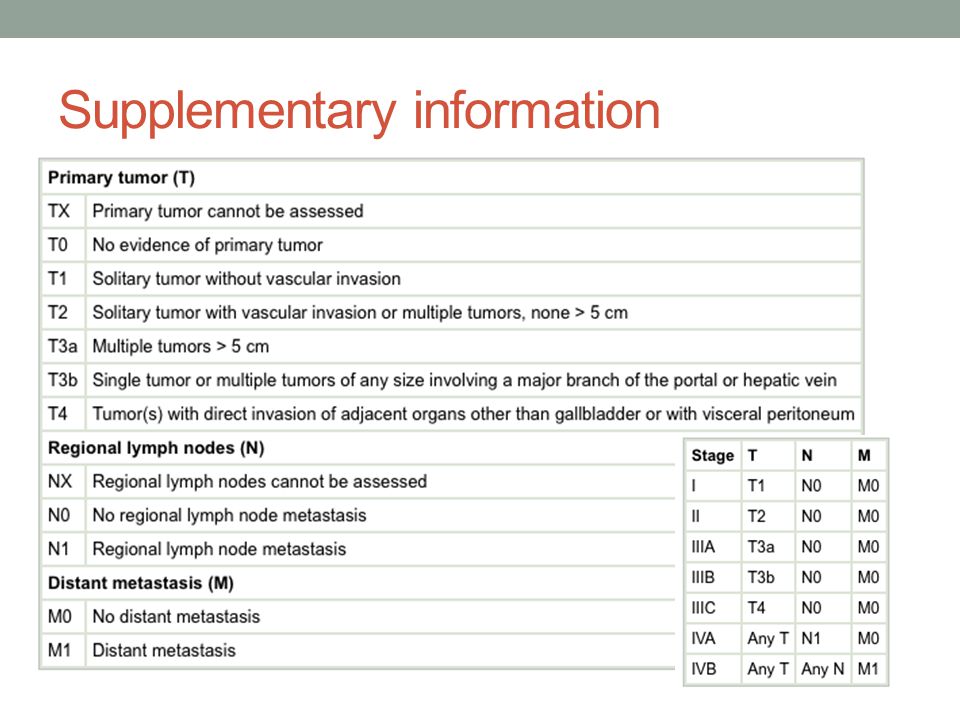
Supplementary information

Similar presentations







 for Liver Tumour Dr Dai Wing Chiu Queen Mary Hospital.>")











