Download presentation
1
EVIDENCE AND DEBATE SCREENING FOR PROSTATE CANCER

2
LEARNING TOPICS Part A: Show me the numbers! What does the available evidence show about the benefits and harms of prostate cancer screening? What additional data may be added to a PSA test to help guide management of an elevated PSA test? Part B: So what do we do? Discuss! Should we be screening for prostate cancer? If so, PSA or DRE or both? Who should we consider screening? How often? Should it be a decision that is shared between providers and patients? How do we do that?

3
THIS IS ON THE BOARDS TOO! A 52-year-old man is evaluated during a periodic health examination. He has benign prostatic hyperplasia, and his father died of prostate cancer at the age of 74 years. His only current medication is tamsulosin. He has no urinary symptoms. Vital signs are normal, as is the remainder of the physical examination Which of the following is the most appropriate management? A. Discuss the risks and benefits of prostate cancer screening B. Obtain a prostate-specific antigen level C. Perform a digital rectal examination D. Perform a digital rectal examination and obtain a prostate- specific antigen level

4
BACKGROUND Prostate cancer is prevalent 1 man in 6 diagnosed in his lifetime Autopsy studies of men who died of other causes found prostate cancer in 30% of men under 80, and in 80% of men over 80 Most men die with, not from, prostate cancer Second leading cause of cancer death in men after lung 1 man in 36 will die from prostate cancer Prostate cancer deaths have been falling for 20 years 40% reduction in prostate ca mortality 1993-2009 PSA screening was approved by the FDA in 1994

5
PSA TEST CHARACTERISTICS PSA >4.0 Sensitivity 21% for all prostate ca 51% for high grade prostate ca (gleason >8) Specificity 91% False elevation in: BPH, prostatitis PSA >3.0 Sensitivity 32% (68% high grade) Specificity 85%
 Specificity 91% False elevation in: BPH, prostatitis PSA >3.0 Sensitivity 32% (68% high grade) Specificity 85%")
6
TWO LARGE RCTS: METHODS PLCO: 10 U.S. centers 76,685 Men 55- 74 13 years f/u Exclusion: Hx of prostate Ca, current cancer Tx, >1 PSA screening prior to entry Annual PSA and DRE vs. usual care PSA cutoff 4 ng/mL ERSPC: multiple countries 162,388 men 55- 69 11 years f/u Exclusion: Hx of prostate Ca Q4 years PSA vs. usual care. Sweden: every 2 years. Belgium + Netherlands, also DRE PSA cutoff 3 ng/mL Finland: 4 ng/mL Belgium: 10ng/mL up to ‘97

7
ADHERENCE AND CONTAMINATION: PLCO ISSUES PLCO Compliance 85% for PSA screening, 86% DRE 52% rate of PSA testing control group in 6th year 41-46% rate of DRE testing control grp 44% of subjects in each group had 1 or more PSA at baseline ERSPC Compliance 82% (screened at least once) 20% rate of PSA testing control grp
 20% rate of PSA testing control grp")
9
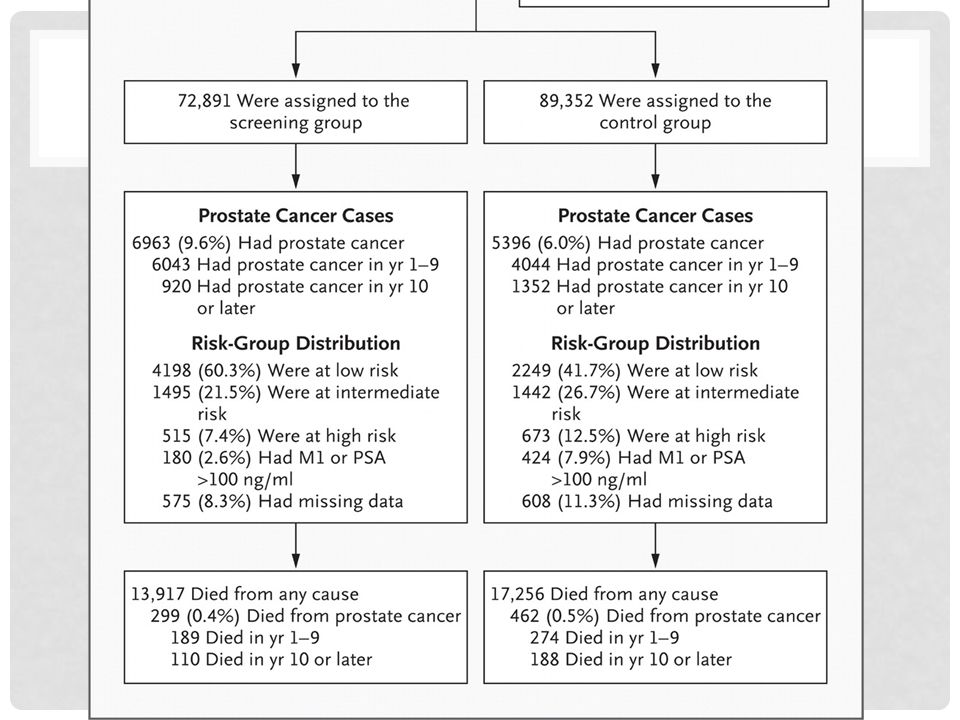
ESRPC BENEFIT? CRUNCH THE NUMBERS Death from Prostate Ca 0.4% vs. 0.5% (p=0.003) RRR? 20% ARR? 0.1% Number needed to invite? 1000 (down from 1410 at 9 years) No difference in all-cause mortality
 RRR. 20% ARR. 0.1% Number needed to invite (down from 1410 at 9 years) No difference in all-cause mortality.")
10
GOTEBERG/SWEDISH TRIAL 50% of subjects also included in ERSPC 20,000 men 50-65 Intervention PSA q 2 years 14 year f/u ARR 0.9% to 0.5%: NNI ~300 12.7% cases of prostate cancer in intervention vs. 8.2%

11
ESRPC HARM? How many men were overdiagnosed? -> Diagnosed by screening that would not have been diagnosed before death ESRPC: Number Needed to Diagnose to prevent one death: 33 Cases of prostate Ca: 65% higher risk with screening 9.6% vs. 6.0% Low risk prostate ca 60% vs. 42% of cases False positives? (risk of biopsy?) 16% of 136,000 PSA tests were positive -> 85% of these underwent bx ->21,000 biopsies for 13,000 cases diagnosed
 16% of 136,000 PSA tests were positive -> 85% of these underwent bx ->21,000 biopsies for 13,000 cases diagnosed.")
12
AFTER THE BIOPSY: ASSIGNING RISK TNM staging (T4 =invading adjacent tissue) Gleason Score: histology Sum of the most common cell pattern and the highest grade
 Gleason Score: histology Sum of the most common cell pattern and the highest grade")
13
TREATMENT FOR PROSTATE CANCER: WHAT ARE THE AES? If localized and life expectancy >10 yrs and intermediate risk (gleason >7, PSA >10) Radical prostatectomy and radiation equally effective Impotence and Incontinence are common complications of radical prostatectomy Radiation proctitis and cystitis common If high-risk Androgen deprivation tx (gnRH agonist) AES:impotence, hot flashes, fatigue, gynecomastia, osteoporosis, weight gain Chemotherapy may increase survival 3-6 months in metastatic disease: docetaxel
 Radical prostatectomy and radiation equally effective Impotence and Incontinence are common complications of radical prostatectomy Radiation proctitis and cystitis common If high-risk Androgen deprivation tx (gnRH agonist) AES:impotence, hot flashes, fatigue, gynecomastia, osteoporosis, weight gain Chemotherapy may increase survival 3-6 months in metastatic disease: docetaxel.")
14
TREATMENT VS. WATCHFUL WAITING FOR LOCALIZED PROSTATE CANCER US PIVOT RCT T1-T2, any grade, PSA <50 Most PCa detected through screening No significant difference in mortality 50% of participants died by the end of the 10 year trial Scandinavian Study T1-T2, any grade, PSA <50 Most PCa detected through sx (> 75% palpable) 6% absolute reduction in mortality at 15 years with treatment 20.7% vs.14.6% No benefit in men older than 65
 6% absolute reduction in mortality at 15 years with treatment 20.7% vs.14.6% No benefit in men older than 65.")
15
OTHER CONSIDERATIONS Lead Time estimated to be 6 or 7 years Why is this important?

16
BEFORE THE BIOPSY: HOW CAN WE MAKE A SCREENING TEST BETTER? RISK STRATIFICATION DRE? Doubling time of PSA? PSA density (relative to prostate size) PCA3 is a new tumor marker, studies underway Higher specificity/sensitivity for high risk ca May be most useful in determining watchful waiting vs. treatment?
 PCA3 is a new tumor marker, studies underway Higher specificity/sensitivity for high risk ca May be most useful in determining watchful waiting vs. treatment .")
17
MORE INDIVIDUALIZED RISK African American Race: ~40% increased risk based on prostate cancer prevention trial

19
SWEDISH STUDY CASE CONTROL Subgroup of ERSPC April 2013: Case Control study of relation between PSA at age 40-55 and risk of metastasis 15-year risk for metastatic prostate ca at highest deciles of PSA: 0.6% PSA >1.3 at 40 1.6% >1.6 at 45-49 5.2% >2.4 at 51-55 25-year risk is 0.2% for a 60 yr old man if PSA <1 If 2 repeat screenings in 50s and at 60?

20
WHAT IS AN INTERNIST TO DO? To screen or not to screen? What would you do? Discuss NEJM case IF we screen: What value should we consider elevated? What ages should we screen? Men 50-65 with life expectancy >10-15 years? Start at 45 like swedish study authors suggest? With DRE? How often? Every 4 years? Every 2? Less often if initial <1? Shared decision? What are the barriers to this?

21
THIS IS ON THE BOARDS TOO! A 52-year-old man is evaluated during a periodic health examination. He has benign prostatic hyperplasia, and his father died of prostate cancer at the age of 74 years. His only current medication is tamsulosin. He has no urinary symptoms. Vital signs are normal, as is the remainder of the physical examination Which of the following is the most appropriate management? A. Discuss the risks and benefits of prostate cancer screening B. Obtain a prostate-specific antigen level C. Perform a digital rectal examination D. Perform a digital rectal examination and obtain a prostate- specific antigen level

22
SHARED DECISION MAKING IOM statement 2001: patient-centered care ensures “that patient values guide all clinical decisions.” An intervention should be considered a standard when there is “virtual unanimity among patients about the overall desirability… of the outcomes.” David Eddy In SDM patients and providers discuss the risks, benefits, and burdens of medical tests and interventions with the goal of reaching decisions that are concordant with a patient’s goals and values

23
HOW DO WE HAVE SHARED DECISIONS IN THE OFFICE? ASK: invite to participate, Assess for knowledge “Tell me what you know about ….” TELL: Communicating statistics on risks and benefits of screening Teach-back ASK: what matters to them? What questions to they have? What decision sounds right for them? Doing everything possible to avoid dying from prostate cancer? Keeping sexual and urinary function? Avoiding a biopsy?

24
“BUT IT’S JUST A BLOOD TEST, DOC!” HOW DO WE COMMUNICATE STATISTICS TO PATIENTS?

25
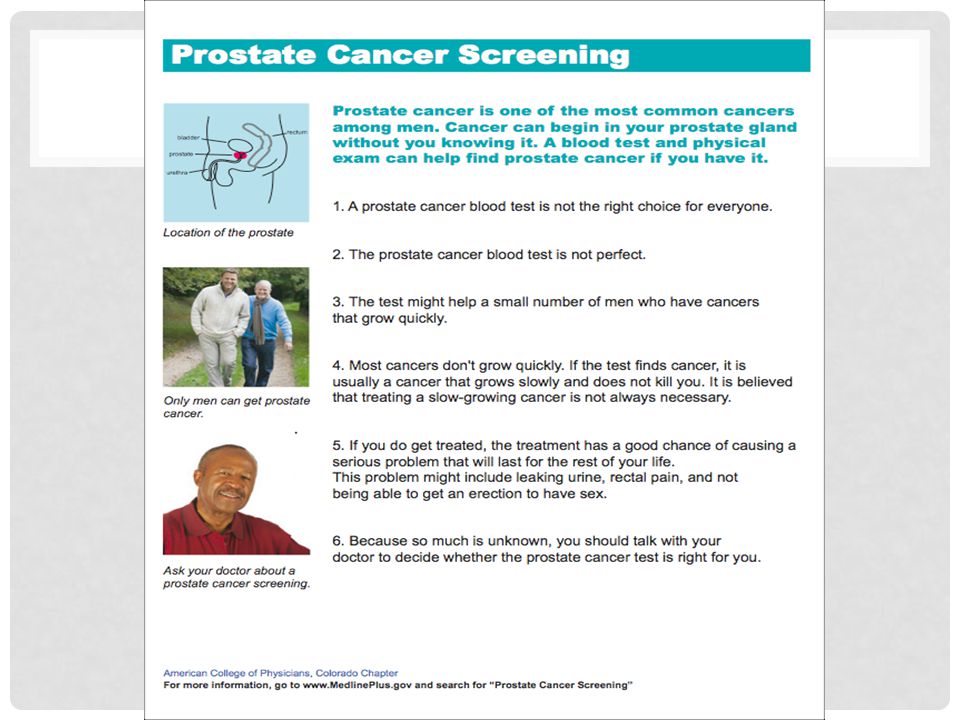
DECISION AIDS Studies show that when patients are more informed they are more likely to take an active role in medical decision making Meta-analysis of Prostate Cancer screening decision aids Increase patient knowledge increase patient participation in decision making lower PSA testing Most are involved (DVDs, long pamphlets), tested under ideal circumstances -> implementation is challenging
, tested under ideal circumstances -> implementation is challenging")
27
TRY THIS Stats review: 1/6 is diagnosed in his lifetime, 1/36 will die Screening increases risk of diagnosis of prostate cancer from 6/100 to 10/100 NNI: 1000 NND: 33 Most of these men will still be treated (field is evolving with PCA3, PSA density, doubling time, treatment vs. watchful waiting, etc.)
.")