Download presentation
Presentation is loading. Please wait.

1
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 Conference Review Presenter Name InstitutionDate

2
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 Agenda CoronaryCoronary –RESOLUTE Pooled –DUTCH PEERS Transcatheter ValvesTranscatheter Valves –CoreValve Extreme Risk – 2yr –PARTNER Cohort B – 5yr Renal DenervationRenal Denervation –SYMPLICITY HTN-3 – 1yr This is a selection of key slides from data presented at Transcatheter Cardiovascular Therapeutics (TCT) conference on Sep 13-17 2014.
 conference on Sep")
3
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 Coronary

5
RESOLUTE Pooled – Small Vessel DM Percutaneous coronary intervention (PCI) of small vessels has been associated with high risk of recurrent events, especially in patients with diabetes mellitus (DM). The Resolute ™ zotarolimus-eluting stent (R-ZES) showed good clinical outcomes in small vessels as well as patients with DM at 2 years. 1,2 The current analysis aims to study the impact of DM (including insulin dependence) on long term clinical outcomes in patients who underwent PCI in small vessels with R-ZES. Background 1 Caputo R, et al. Catheterization and Cardiovascular Interventions. 2014;84:17–23 (small vessels defined as RVD 2.5mm) 2 Silber S, et al. J Am Coll Cardiol Intv. 2013;6:357– 68
 showed good clinical outcomes in small vessels as well as patients with DM at 2 years. 1,2 The current analysis aims to study the impact of DM (including insulin dependence) on long term clinical outcomes in patients who underwent PCI in small vessels with R-ZES. Background 1 Caputo R, et al. Catheterization and Cardiovascular Interventions. 2014;84:17–23 (small vessels defined as RVD 2.5mm) 2 Silber S, et al. J Am Coll Cardiol Intv. 2013;6:357– 68.")
6
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM Patient-level data of 2722 patients who had at least one lesion treated in a small vessel (RVD ≤ 2.5mm) from 10 clinical trials in the RESOLUTE global clinical program were included in this post-hoc pooled analysis. Patients were stratified according to their diabetic status: – –Insulin-dependent DM (IDDM, N=233) – –Non-insulin dependent DM (Non-IDDM, N=725) – –Non-diabetic (N=1764) Kaplan Meier cumulative incidence out to 3-year follow- up was calculated. Given differences in baseline characteristics, patients were matched by propensity scores based on 26 baseline variables and adjusted p-values are provided. Methods
 from 10 clinical trials in the RESOLUTE global clinical program were included in this post-hoc pooled analysis. Patients were stratified according to their diabetic status: – –Insulin-dependent DM (IDDM, N=233) – –Non-insulin dependent DM (Non-IDDM, N=725) – –Non-diabetic (N=1764) Kaplan Meier cumulative incidence out to 3-year follow- up was calculated. Given differences in baseline characteristics, patients were matched by propensity scores based on 26 baseline variables and adjusted p-values are provided. Methods.")
7
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 Latest Available Follow Up RESOLUTE Global Clinical Program RESOLUTE 1 Non-RCT First-in-Human (R=139) 5 yr RESOLUTE AC 2,3 1:1 RCT vs. Xience V ™ EES (R=1140; X=1152) 5 yr Non-RCT Observational (R=2349) 3 yr 2.25 – 4.0 mm Non-RCT vs. Hx Control (R=1402) 4 yr RESOLUTE US 6 2.5 – 3.5 mm Non-RCT (R=100) vs. Hx Control RESOLUTE Japan 4 yr RESOLUTE Asia 7 Non-RCT Observational (R=312) 2 yr 1:1 RCT vs. Taxus ™ PES (R=200; T=200) R-China RCT 8 2 yr RESOLUTE Int 4,5 RESOLUTE Int 4,5 R-China Registry 9 Non-RCT Observational (R=1800) 2 yr R-Japan SVS 2.25 Non-RCT vs. PG (R=65) 3 yr 38 mm sub-study Non-RCT vs. PG (R=114) 3 yr R-US 38mm 7 2722 Patients With a Lesion in a Small Vessel 1 Meredith IT, et al. EuroIntervention. 2010;5:692-7. 2 Serruys PW, et al. N Engl J Med. 2010;363:136-46. 3 Silber S, et al. Lancet. 2011;377:1241-47. 4 Neumann FJ, et al. EuroIntervention. 2012;7(10):1181-8. 5 Belardi JA, et al. J Interv Cardiol. 2013;26(5):515-23. 6 Yeung AC, et al. JACC. 2011;57:1778-83. 7 Lee M, et al. Am J Cardiol. 2013;112(9):1335-41. 8 Xu B, et al. JACC Cardiovasc Interv. 2013;6(7):664-70. 9 Qiao S, et al. Am J Cardiol. 2013. doi: 10.1016/j.amjcard.2013.10.042. [Epub ahead of print]
 5 yr RESOLUTE AC 2,3 1:1 RCT vs. Xience V ™ EES (R=1140; X=1152) 5 yr Non-RCT Observational (R=2349) 3 yr 2.25 – 4.0 mm Non-RCT vs. Hx Control (R=1402) 4 yr RESOLUTE US – 3.5 mm Non-RCT (R=100) vs. Hx Control RESOLUTE Japan 4 yr RESOLUTE Asia 7 Non-RCT Observational (R=312) 2 yr 1:1 RCT vs. Taxus ™ PES (R=200; T=200) R-China RCT 8 2 yr RESOLUTE Int 4,5 RESOLUTE Int 4,5 R-China Registry 9 Non-RCT Observational (R=1800) 2 yr R-Japan SVS 2.25 Non-RCT vs. PG (R=65) 3 yr 38 mm sub-study Non-RCT vs. PG (R=114) 3 yr R-US 38mm Patients With a Lesion in a Small Vessel 1 Meredith IT, et al. EuroIntervention. 2010;5: Serruys PW, et al. N Engl J Med. 2010;363: Silber S, et al. Lancet. 2011;377: Neumann FJ, et al. EuroIntervention. 2012;7(10): Belardi JA, et al. J Interv Cardiol. 2013;26(5): Yeung AC, et al. JACC. 2011;57: Lee M, et al. Am J Cardiol. 2013;112(9): Xu B, et al. JACC Cardiovasc Interv. 2013;6(7): Qiao S, et al. Am J Cardiol doi: /j.amjcard [Epub ahead of print].")
8
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM % Non-Diabetic n = 1764 pts, 2741 lesions Non-IDDM n = 725 pts, 1104 lesions IDDM n = 233 pts, 336 lesions P-value Non-DM vs NIDDM P-value Non-DM vs IDDM Age (yr)63.7±11.365.1±10.164.8±10.00.003NS Men75.169.856.20.008<0.001 Hypertension69.783.792.3 <0.001 Hyperlipidemia63.970.381.5 0.002<0.001 Current smoker24.619.715.9 0.0090.003 Family history of CAD32.226.139.7 0.0060.046 Prior MI28.929.932.3 NS Prior PCI27.430.838.2 NS<0.001 Prior CABG6.18.39.9 NS0.035 Cardiac status NS<0.001 Silent Ischemia2.33.24.3 Stable Angina36.1 51.0 Unstable Angina35.741.626.0 Myocardial Infarction25.919.118.8 ACS 50.352.735.6NS<0.001 STEMI6.94.51.00.035<0.001 Baseline Patient Characteristics
63.7± ± ± NS Men <0.001 Hypertension <0.001 Hyperlipidemia <0.001 Current smoker Family history of CAD Prior MI NS Prior PCI NS<0.001 Prior CABG NS0.035 Cardiac status NS<0.001 Silent Ischemia Stable Angina Unstable Angina Myocardial Infarction ACS NS<0.001 STEMI <0.001 Baseline Patient Characteristics.")
9
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM % Non-Diabetic n = 1764 pts, 2741 lesions Non-IDDM n = 725 pts, 1104 lesions IDDM n = 233 pts, 336 lesions P-value Non-DM vs NIDDM P-value Non-DM vs IDDM Lesion location (lesion level): LAD43.840.341.9 NS LCx31.733.227.4 NS RCA23.325.128.6 NS Left main0.70.50.9 NS Bypass graft0.50.81.2NS B2/C Lesion class ACC/AHA65.667.264.2NS Bifurcation15.014.311.2NS In-stent restenosis3.73.46.3NS RVD 1 2.4±0.42.5±0.42.4±0.4NS0.007 MLD0.6±0.4 NS Diameter stenosis74.8±16.376.0±16.072.9±16.00.0470.05 Lesion length (mm)16.4±10.117.9±12.016.0±10.1<0.001NS Lesions treated per patient1.6±0.8 1.4±0.7NS0.005 Number of stents per patient1.8±1.1 1.6±1.0NS0.010 Stent length per patient (mm)36.6±25.238.4±27.531.7±21.6NS0.002 Complex patients 2 46.442.937.8NS0.014 Lesion and Procedure Characteristics 1 RVD of all treated lesions of patients who have at least one small vessel (RVD ≤2.5mm) stented. 2 Complex patient definition: Bifurcation, Bypass grafts, ISR, AMI 2 vessels stented, renal insufficiency or failure (creatinine >140 µmol/L), lesion length >27 mm, >1 lesion per vessel, lesion with thrombus or TO (preprocedure TIMI = 0).
: LAD NS LCx NS RCA NS Left main NS Bypass graft NS B2/C Lesion class ACC/AHA NS Bifurcation NS In-stent restenosis NS RVD 1 2.4±0.42.5±0.42.4±0.4NS0.007 MLD0.6±0.4 NS Diameter stenosis74.8± ± ± Lesion length (mm)16.4± ± ±10.1<0.001NS Lesions treated per patient1.6± ±0.7NS0.005 Number of stents per patient1.8± ±1.0NS0.010 Stent length per patient (mm)36.6± ± ±21.6NS0.002 Complex patients NS0.014 Lesion and Procedure Characteristics 1 RVD of all treated lesions of patients who have at least one small vessel (RVD ≤2.5mm) stented. 2 Complex patient definition: Bifurcation, Bypass grafts, ISR, AMI 2 vessels stented, renal insufficiency or failure (creatinine >140 µmol/L), lesion length >27 mm, >1 lesion per vessel, lesion with thrombus or TO (preprocedure TIMI = 0)..")
10
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM Target Lesion Failure to 3 Years Time After Initial Procedure (Years) No. at risk Non-Diabetics 1764173416141169 Non-IDDM 725722667448 IDDM 233226201178 0 Cumulative Incidence of TLF (%) 50 30 20 0 10 Non-DM vs Non-IDDM P = 0.86 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics 40 10.7% 123 21.2% 9.8% Non-DM vs IDDM P < 0.001 Target Lesion Failure is defined as cardiac death, target vessel MI and target lesion revascularization. Data from post-hoc analysis.
 No. at risk Non-Diabetics Non-IDDM IDDM Cumulative Incidence of TLF (%) Non-DM vs Non-IDDM P = 0.86 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics % % 9.8% Non-DM vs IDDM P < Target Lesion Failure is defined as cardiac death, target vessel MI and target lesion revascularization. Data from post-hoc analysis..")
11
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM Target Lesion Revascularization to 3 Years No. at risk Non-Diabetics 1764176316591210 Non-IDDM 725724683455 IDDM 233232210186 0 50 30 20 0 10 40 123 Cumulative Incidence of TLR (%) Time After Initial Procedure (Years) 12.2% 5.0% 4.9% Non-DM vs Non-IDDM P = 0.65 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P < 0.001 Data from post-hoc analysis.
 Time After Initial Procedure (Years) 12.2% 5.0% 4.9% Non-DM vs Non-IDDM P = 0.65 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P < Data from post-hoc analysis..")
12
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM Cardiac Death / TVMI to 3 Years 0 Cumulative Incidence of Cardiac Death/TVMI (%) 50 30 20 10 40 123 Time After Initial Procedure (Years) 0 11.5% 6.9% 5.4% No. at risk Non-Diabetics 1764 173516561222 Non-IDDM 725 722681465 IDDM 233227213196 Non-DM vs Non-IDDM P = 0.27 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P = 0.002 Data from post-hoc analysis.
 Time After Initial Procedure (Years) % 6.9% 5.4% No. at risk Non-Diabetics Non-IDDM IDDM Non-DM vs Non-IDDM P = 0.27 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P = Data from post-hoc analysis..")
13
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM Stent Thrombosis (ARC Def/Prob) to 3 Years 0 Cumulative Incidence of ARC Definite or Probable Stent Thrombosis (%) 0 10 0 5 123 Time After Initial Procedure (Years) 1.3% 1.0% No. at risk Non-Diabetics 1764 176317021264 Non-IDDM 725 724699474 IDDM 233232223205 Non-DM vs Non-IDDM P = 0.94 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P = 0.52 Data from post-hoc analysis.
 to 3 Years 0 Cumulative Incidence of ARC Definite or Probable Stent Thrombosis (%) Time After Initial Procedure (Years) 1.3% 1.0% No. at risk Non-Diabetics Non-IDDM IDDM Non-DM vs Non-IDDM P = 0.94 Small Vessel Non-IDDM Small Vessel IDDM Small Vessel Non-Diabetics Non-DM vs IDDM P = 0.52 Data from post-hoc analysis..")
14
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RESOLUTE Pooled – Small Vessel DM This analysis of patients undergoing PCI in small vessels with R-ZES showed similar 3-year outcomes between non-IDDM and non-DM patients, which was lower than with IDDM. Stent Thrombosis (ARC Def/Prob) to 3 years was similar between non-DM and both groups of diabetics; supporting the safety of R-ZES in small vessels. These outcomes further demonstrated the long-term safety and effectiveness of R-ZES in Non-IDDM and non-DM patients in small coronary vessels. Conclusions Data from post-hoc analysis.
 to 3 years was similar between non-DM and both groups of diabetics; supporting the safety of R-ZES in small vessels. These outcomes further demonstrated the long-term safety and effectiveness of R-ZES in Non-IDDM and non-DM patients in small coronary vessels. Conclusions Data from post-hoc analysis..")
15
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14

24
II. Transcatheter Valves

25
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14

50
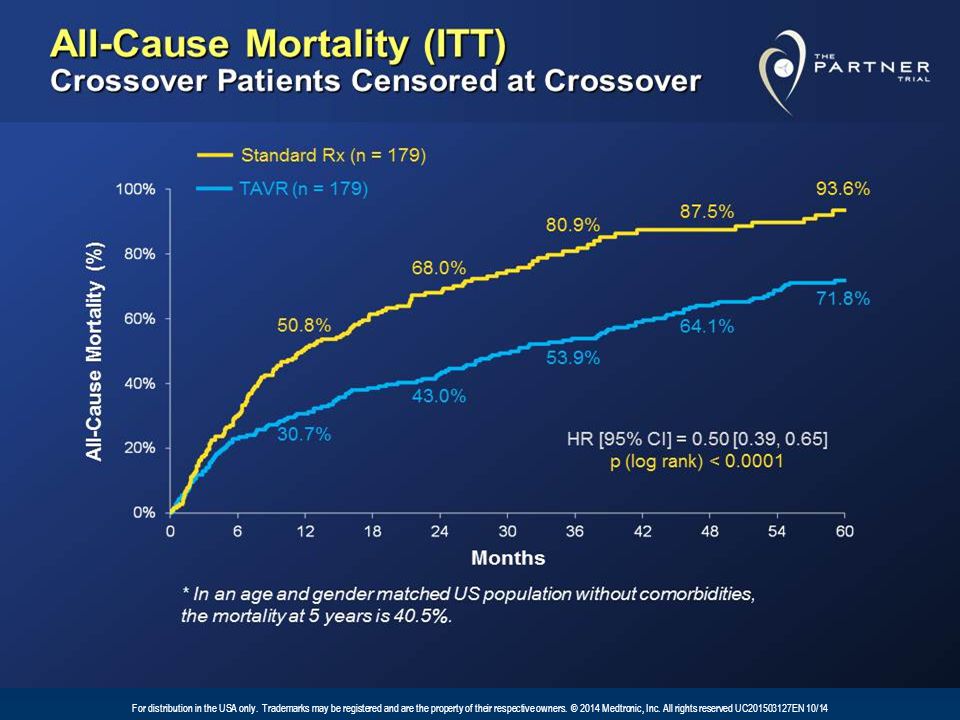
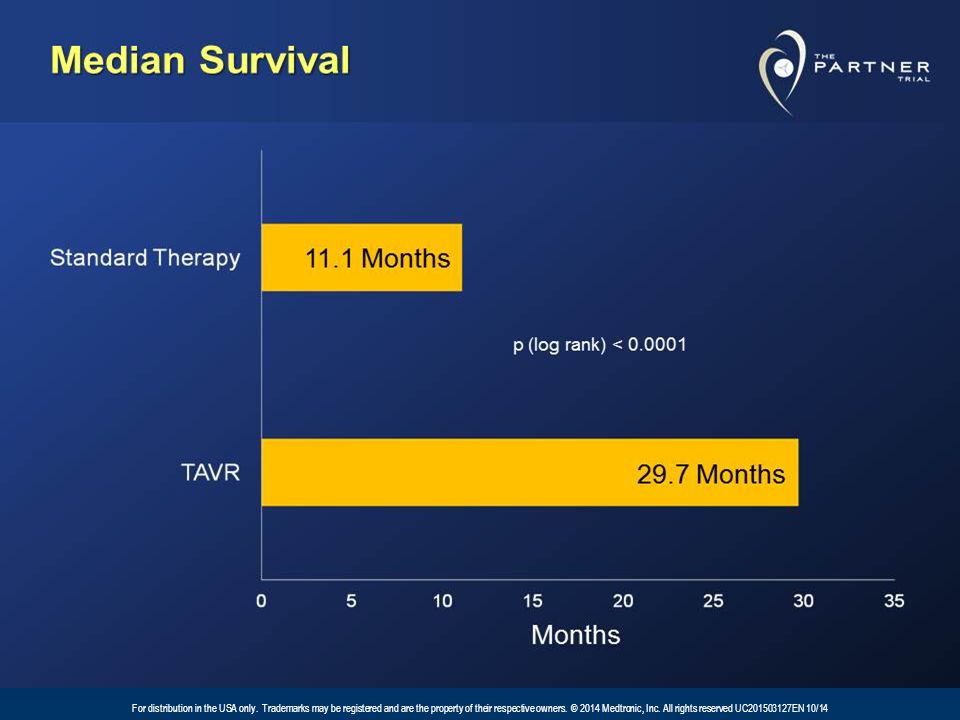
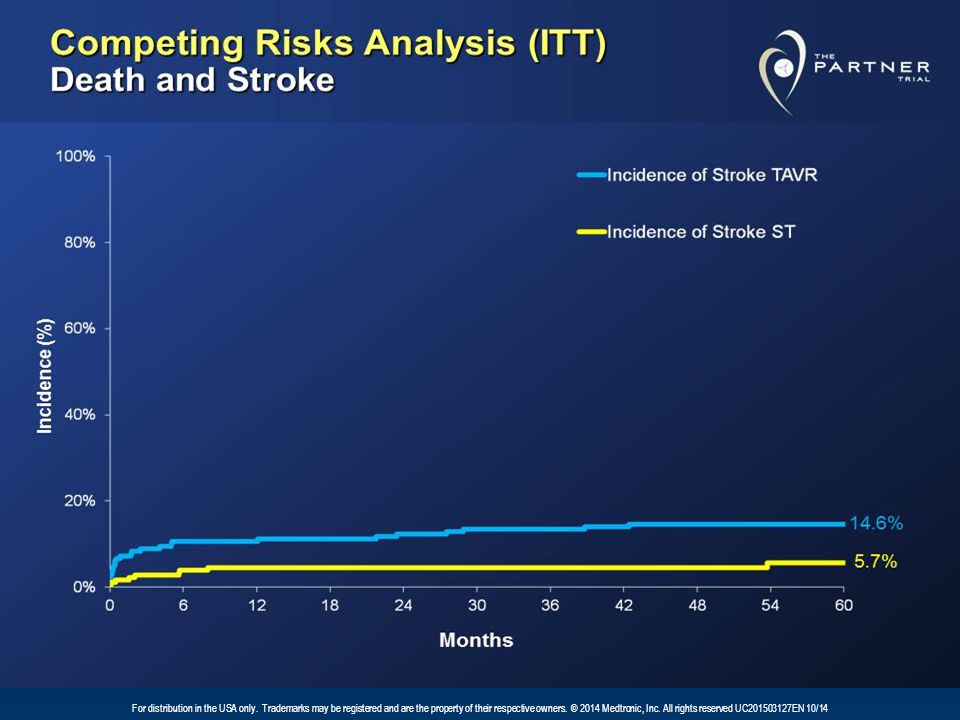
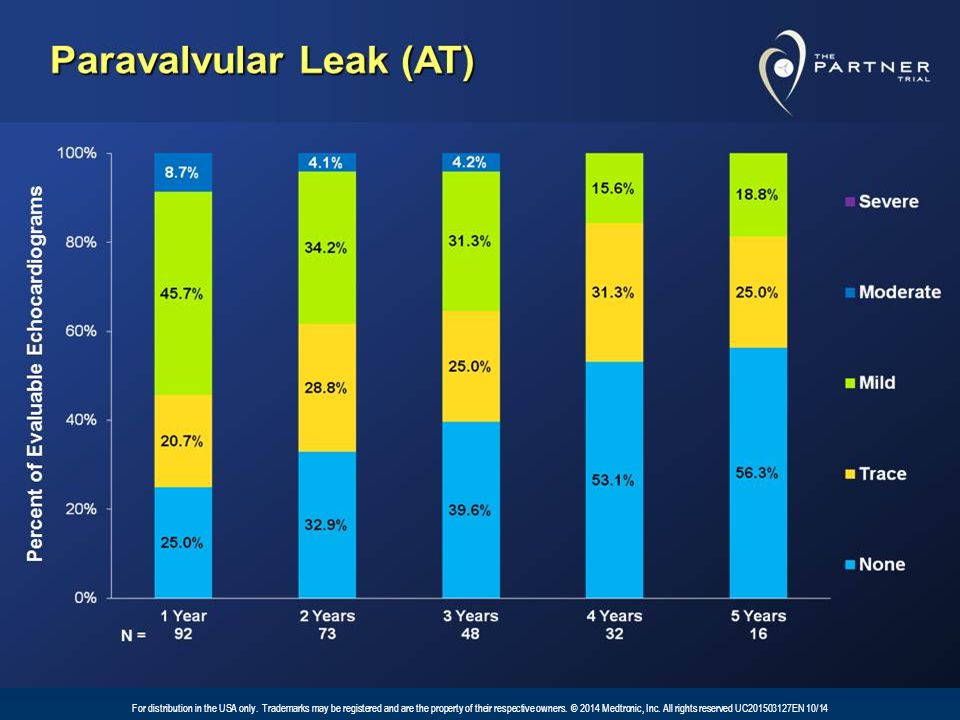
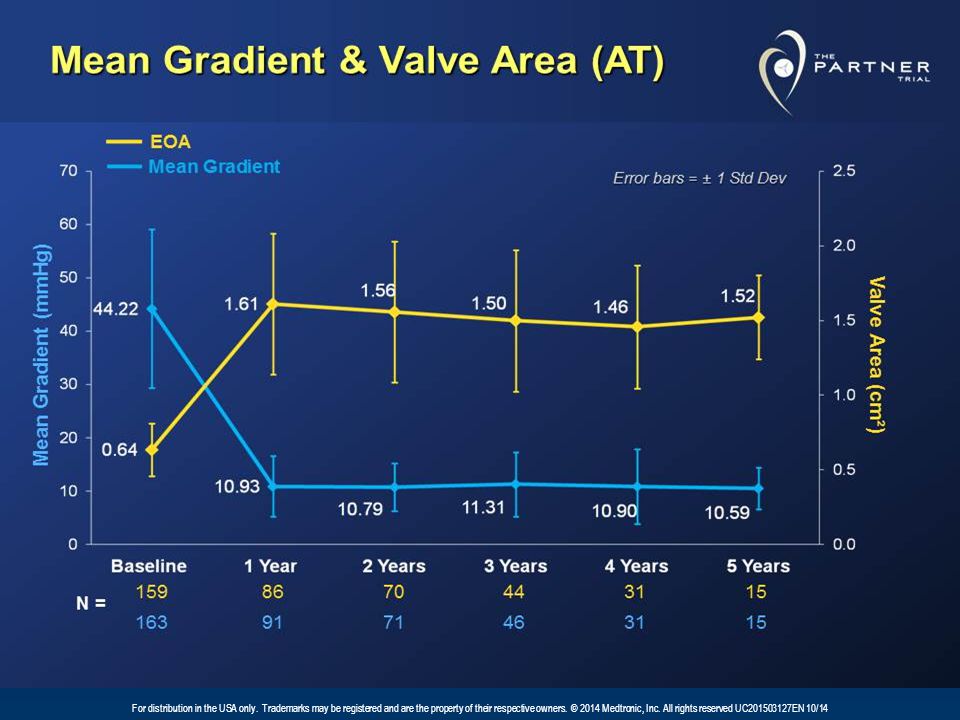
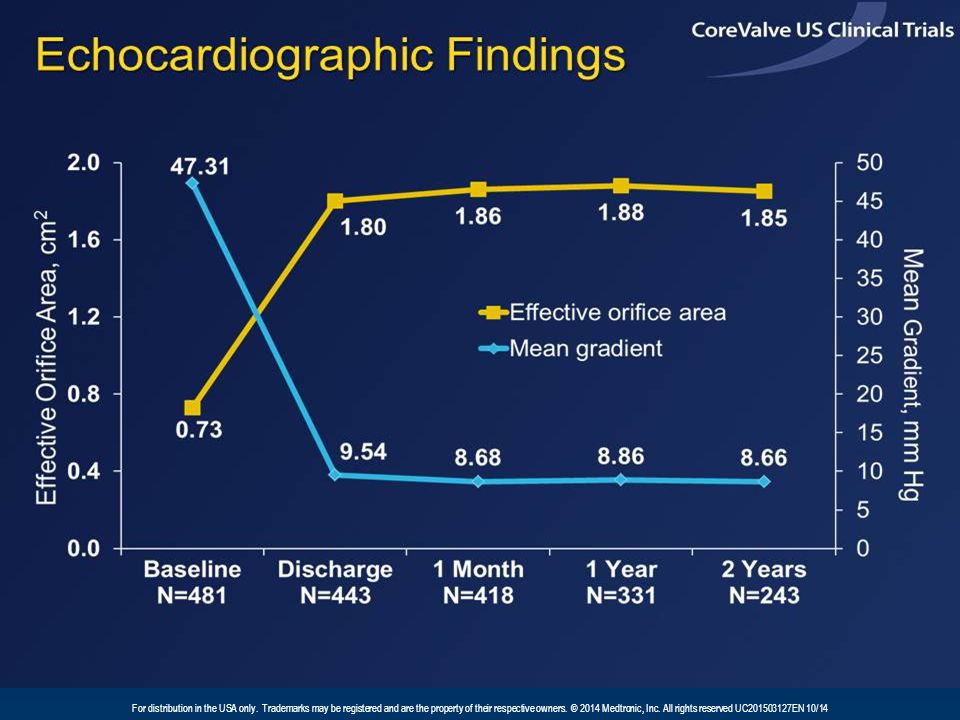
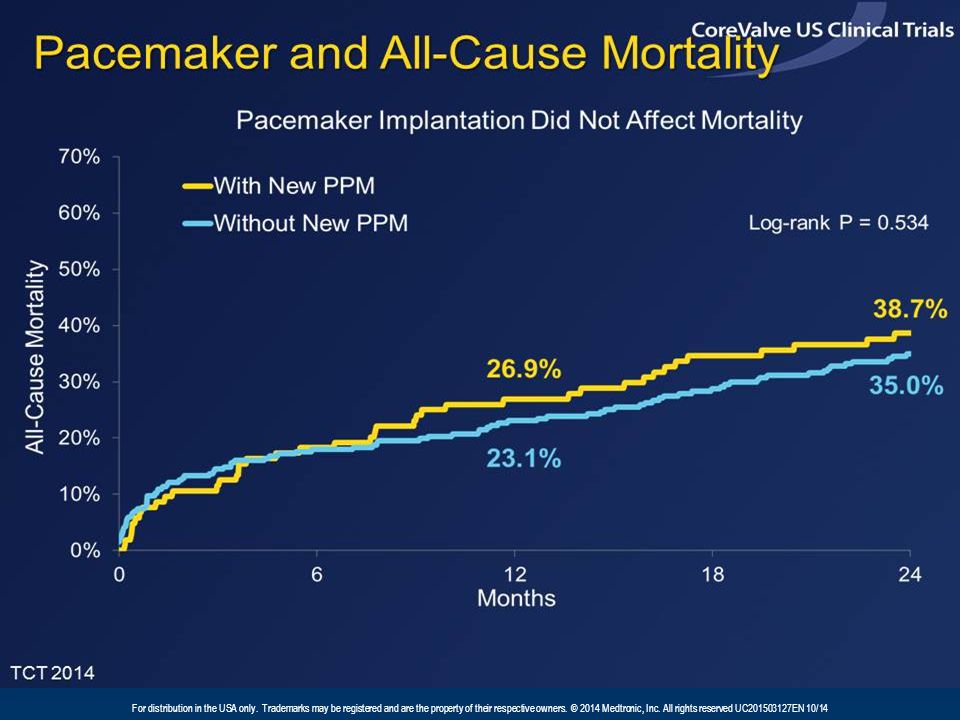
TAVR – Take Home Messages The 5-year results from PARTNER B demonstrate the longer-term benefits of TAVR in patients unsuitable for surgical AVR.The 5-year results from PARTNER B demonstrate the longer-term benefits of TAVR in patients unsuitable for surgical AVR. The 2-year results from the CoreValve US Extreme Risk Study confirmed the improved survival benefit of this therapy. We observed:The 2-year results from the CoreValve US Extreme Risk Study confirmed the improved survival benefit of this therapy. We observed: –low rates of mortality and major stroke, –sustained hemodynamics and –low rates of moderate PVL, which were not associated with mortality

51
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 III. Renal Denervation The following data from the SYMPLICITY HTN-3 trial are included as renal denervation was a key topic at the TCT conference and continues to generate a lot of interest. When reviewing these data it is important to recognize that while the SYMPLICITY HTN-3 trial met its primary safety endpoint, it failed to meet its primary efficacy endpoint.

52
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
53
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
54
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
55
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
56
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
57
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
58
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
59
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
60
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
61
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
62
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
63
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
64
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
65
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
66
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
67
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
68
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
69
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
70
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. Not available for sale in the United States.
 law to investigational use. Not available for sale in the United States..")
71
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 RDN – Take Home Messages Continued reduction of BP in SYMPLICITY HTN-3 trial out to 12 monthsContinued reduction of BP in SYMPLICITY HTN-3 trial out to 12 months Impact of denervation distribution is important as demonstrated by both clinical and histopathologic and animal dataImpact of denervation distribution is important as demonstrated by both clinical and histopathologic and animal data Subgroup analyses are suggestive of physiologic and adherence differences amongst groupsSubgroup analyses are suggestive of physiologic and adherence differences amongst groups

72
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 CoreValve System Safety Information During deployment, the bioprosthesis can be advanced or withdrawn as long as annular contact has not been made. Once annular contact is made, the bioprosthesis cannot be advanced in the retrograde direction; if necessary, and the frame has only been deployed ≤2/3 of its length, the bioprosthesis can be withdrawn (repositioned) in the antegrade direction. However, use caution when moving the bioprosthesis in the antegrade direction. Use the handle of the delivery system to reposition the bioprosthesis. Do not use the outer catheter sheath. Once deployment is complete, repositioning of the bioprosthesis (e.g., use of a snare and/or forceps) is not recommended. Repositioning of a deployed valve may cause aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. Do not attempt to retrieve a bioprosthesis if any one of the outflow struts is protruding from the capsule. If any one of the outflow struts has deployed from the capsule, the bioprosthesis must be released from the catheter before the catheter can be withdrawn. Ensure the capsule is closed before catheter removal. If increased resistance is encountered when removing the catheter through the introducer sheath, do not force passage. Increased resistance may indicate a problem and forced passage may result in damage to the device and/or harm to the patient. If the cause of resistance cannot be determined or corrected, remove the catheter and introducer sheath as a single unit over the guidewire, and inspect the catheter and confirm that it is complete. Clinical long-term durability has not been established for the bioprosthesis. Evaluate bioprosthesis performance as needed during patient follow-up. Postprocedure, administer appropriate antibiotic prophylaxis as needed for patients at risk for prosthetic valve infection and endocarditis. Postprocedure, administer anticoagulation and/or antiplatelet therapy per hospital protocol. Excessive contrast media may cause renal failure. Preprocedure, measure the patient's creatinine level. During the procedure, monitor contrast media usage. Conduct the procedure under fluoroscopy. The safety and efficacy of implanting a second CoreValve bioprosthesis within the initial CoreValve bioprosthesis have not been demonstrated. However, in the event that a second CoreValve bioprosthesis must be implanted within the initial CoreValve bioprosthesis to improve valve function, valve size and patient anatomy must be considered before implantation of the second CoreValve bioprosthesis to ensure patient safety (e.g., to avoid coronary obstruction). In the event that valve function or sealing is impaired due to excessive calcification or incomplete expansion, a postimplant balloon dilatation of the bioprosthesis may improve valve function and sealing. To ensure patient safety, valve size and patient anatomy must be considered when selecting the size of the balloon used for dilatation. The balloon size chosen for dilatation should not exceed the diameter of the native aortic annulus. Refer to the specific balloon catheter manufacture’s labeling for proper instruction on the use of balloon catheter devices. Note: Bench testing has only been conducted to confirm compatibility with NuMED Z-MED IITM Balloon Aortic Valvuloplasty catheters where CoreValveTM bioprosthesis device performance was maintained after dilation. Data on File. Potential Adverse Events Potential risks associated with the implantation of the Medtronic CoreValve transcatheter aortic valve may include, but are not limited to, the following: death cardiac arrest coronary occlusion, obstruction, or vessel spasm (including acute coronary closure) emergent surgery (e.g., coronary artery bypass, heart valve replacement, valve explant) multi-organ failure heart failure myocardial infarction cardiogenic shock respiratory insufficiency or respiratory failure cardiovascular injury (including rupture, perforation, or dissection of vessels, ventricle, myocardium, or valvular structures that may require intervention) perforation of the myocardium or a vessel ascending aorta trauma cardiac tamponade cardiac failure or low cardiac output prosthetic valve dysfunction including, but not limited to, fracture; bending (out-of-round configuration) of the valve frame; under-expansion of the valve frame; calcification; pannus; leaflet wear, tear, prolapse, or retraction; poor valve coaptation; suture breaks or disruption; leaks; mal-sizing (prosthesis-patient mismatch); malposition (either too high or too low)/malplacement; regurgitation; stenosis thrombosis/embolus (including valve thrombosis) valve migration/valve embolization ancillary device embolization emergent percutaneous coronary intervention (PCI) emergent balloon valvuloplasty major or minor bleeding that may or may not require transfusion or intervention (including life-threatening or disabling bleeding) allergic reaction to antiplatelet agents, contrast medium, or anesthesia infection (including septicemia and endocarditis) stroke, TIA, or other neurological deficits permanent disability renal insufficiency or renal failure (including acute kidney injury) mitral valve regurgitation or injury tissue erosion vascular access related complications (e.g., dissection, perforation, pain, bleeding, hematoma, pseudoaneurysm, irreversible nerve injury, compartment syndrome, arteriovenous fistula, stenosis) conduction system disturbances (e.g., atrioventricular node block, left- bundle branch block, asystole), which may require a permanent pacemaker CAUTION : Federal (USA) law restricts this device to sale by or on the order of a physician. For further information, please call and/or consult Medtronic at the toll-free numbers or websites listed. Indications The Medtronic CoreValve system is indicated for relief of aortic stenosis in patients with symptomatic heart disease due to severe native calcific aortic stenosis (aortic valve area ≤1.0 cm2 or aortic valve area index ≤ 0.6cm2/m2, a mean aortic valve gradient of ≥40 mm Hg, or a peak aortic-jet velocity of ≥4.0 m/s) and with native anatomy appropriate for the 23, 26, 29 or 31mm valve system who are judged by a heart team, including a cardiac surgeon, to be at extreme risk or inoperable for open surgical therapy (predicted risk of operative mortality and/or serious irreversible morbidity ≥50% at 30 days). Contraindications The CoreValve system is contraindicated for patients presenting with any of the following conditions: known hypersensitivity or contraindication to aspirin, heparin (HIT/HITTS) and bivalirudin, ticlopidine, clopidogrel, Nitinol (Titanium or Nickel), or sensitivity to contrast media, which cannot be adequately premedicated ongoing sepsis, including active endocarditis preexisting mechanical heart valve in aortic position Warnings General Implantation of the Medtronic CoreValve system should be performed only by physicians who have received Medtronic CoreValve training. This procedure should only be performed where emergency aortic valve surgery can be performed promptly. Mechanical failure of the delivery catheter system and/or accessories may result in patient complications. Transcatheter Aortic Valve (Bioprosthesis) Accelerated deterioration of the bioprosthesis may occur in patients presenting with an altered calcium metabolism. Precautions General The safety and effectiveness of the Medtronic CoreValve system have not been evaluated in the pediatric population. The safety and effectiveness of the bioprosthesis for aortic valve replacement have not been evaluated in the following patient populations: without Aortic Stenosis (AS) who are at high, moderate, or low surgical risk (predicted perioperative mortality risk of 29 mm per the baseline diagnostic imaging transarterial access not able to accommodate an 18-Fr sheath sinus of valsalva anatomy that would prevent adequate coronary perfusion moderate to severe mitral stenosis severe ventricular dysfunction with left ventricular ejection fraction (LVEF) <20% as measured by resting echocardiogram end-stage renal disease requiring chronic dialysis or creatinine clearance <20 cc/min symptomatic carotid or vertebral artery disease severe basal septal hypertrophy with an outflow gradient Prior to Use Exposure to glutaraldehyde may cause irritation of the skin, eyes, nose, and throat. Avoid prolonged or repeated exposure to the vapors. Damage may result from forceful handling of the catheter. Prevent kinking of the catheter when removing it from the packaging. This device was designed for single patient use only. Do not reuse, reprocess, or resterilize this product. Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and/or create a risk of contamination of the device, which could result in patient injury, illness, or death. The bioprosthesis size must be appropriate to fit the patient’s anatomy. Proper sizing of the device is the responsibility of the physician. Refer to Instructions for Use for available sizes. Failure to implant a device within the sizing matrix could lead to adverse effects such as those listed in Section 5.0. Patients must present with femoral or subclavian/axillary access vessel diameters of ≥6 mm or an ascending aortic (direct aortic) access site ≥60 mm from the basal plane. Implantation of the bioprosthesis should be avoided in patients with aortic root angulation (angle between plane of aortic valve annulus and horizontal plane/vertebrae) of >30° for right subclavian/axillary access or >70° for femoral and left subclavian/axillary access. Use caution when using the subclavian/ axillary approach in patients with a patent LIMA graft or patent RIMA graft. During Use Adequate rinsing of the bioprosthesis with sterile saline, as described in the Instructions for Use, is mandatory before implantation. During rinsing, do not touch the leaflets or squeeze the bioprosthesis. If a capsule becomes damaged during loading or the capsule fails to close, replace the entire system (bioprosthesis, catheter, and CLS). Do not use a catheter with a damaged capsule. After a bioprosthesis has been inserted into a patient, do not attempt to reload that bioprosthesis on the same or any other catheter. During implantation, if resistance to deployment is encountered (e.g., the micro knob starts clicking or is tight or stuck), apply upward pressure to the macro slider while turning the micro knob. If the bioprosthesis still does not deploy, remove it from the patient and use another system. While the catheter is in the patient, ensure the guidewire is extending from the tip. Do not remove the guidewire from the catheter while the catheter is inserted in the patient. Once deployment is initiated, retrieval of the bioprosthesis from the patient (e.g., use of the catheter) is not recommended. Retrieval of a partially deployed valve using the catheter may cause mechanical failure of the delivery catheter system, aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. All brand names, product names or trademarks belong to their respective holders.
 in the antegrade direction. However, use caution when moving the bioprosthesis in the antegrade direction. Use the handle of the delivery system to reposition the bioprosthesis. Do not use the outer catheter sheath. Once deployment is complete, repositioning of the bioprosthesis (e.g., use of a snare and/or forceps) is not recommended. Repositioning of a deployed valve may cause aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. Do not attempt to retrieve a bioprosthesis if any one of the outflow struts is protruding from the capsule. If any one of the outflow struts has deployed from the capsule, the bioprosthesis must be released from the catheter before the catheter can be withdrawn. Ensure the capsule is closed before catheter removal. If increased resistance is encountered when removing the catheter through the introducer sheath, do not force passage. Increased resistance may indicate a problem and forced passage may result in damage to the device and/or harm to the patient. If the cause of resistance cannot be determined or corrected, remove the catheter and introducer sheath as a single unit over the guidewire, and inspect the catheter and confirm that it is complete. Clinical long-term durability has not been established for the bioprosthesis. Evaluate bioprosthesis performance as needed during patient follow-up. Postprocedure, administer appropriate antibiotic prophylaxis as needed for patients at risk for prosthetic valve infection and endocarditis. Postprocedure, administer anticoagulation and/or antiplatelet therapy per hospital protocol. Excessive contrast media may cause renal failure. Preprocedure, measure the patient s creatinine level. During the procedure, monitor contrast media usage. Conduct the procedure under fluoroscopy. The safety and efficacy of implanting a second CoreValve bioprosthesis within the initial CoreValve bioprosthesis have not been demonstrated. However, in the event that a second CoreValve bioprosthesis must be implanted within the initial CoreValve bioprosthesis to improve valve function, valve size and patient anatomy must be considered before implantation of the second CoreValve bioprosthesis to ensure patient safety (e.g., to avoid coronary obstruction). In the event that valve function or sealing is impaired due to excessive calcification or incomplete expansion, a postimplant balloon dilatation of the bioprosthesis may improve valve function and sealing. To ensure patient safety, valve size and patient anatomy must be considered when selecting the size of the balloon used for dilatation. The balloon size chosen for dilatation should not exceed the diameter of the native aortic annulus. Refer to the specific balloon catheter manufacture’s labeling for proper instruction on the use of balloon catheter devices. Note: Bench testing has only been conducted to confirm compatibility with NuMED Z-MED IITM Balloon Aortic Valvuloplasty catheters where CoreValveTM bioprosthesis device performance was maintained after dilation. Data on File. Potential Adverse Events Potential risks associated with the implantation of the Medtronic CoreValve transcatheter aortic valve may include, but are not limited to, the following: death cardiac arrest coronary occlusion, obstruction, or vessel spasm (including acute coronary closure) emergent surgery (e.g., coronary artery bypass, heart valve replacement, valve explant) multi-organ failure heart failure myocardial infarction cardiogenic shock respiratory insufficiency or respiratory failure cardiovascular injury (including rupture, perforation, or dissection of vessels, ventricle, myocardium, or valvular structures that may require intervention) perforation of the myocardium or a vessel ascending aorta trauma cardiac tamponade cardiac failure or low cardiac output prosthetic valve dysfunction including, but not limited to, fracture; bending (out-of-round configuration) of the valve frame; under-expansion of the valve frame; calcification; pannus; leaflet wear, tear, prolapse, or retraction; poor valve coaptation; suture breaks or disruption; leaks; mal-sizing (prosthesis-patient mismatch); malposition (either too high or too low)/malplacement; regurgitation; stenosis thrombosis/embolus (including valve thrombosis) valve migration/valve embolization ancillary device embolization emergent percutaneous coronary intervention (PCI) emergent balloon valvuloplasty major or minor bleeding that may or may not require transfusion or intervention (including life-threatening or disabling bleeding) allergic reaction to antiplatelet agents, contrast medium, or anesthesia infection (including septicemia and endocarditis) stroke, TIA, or other neurological deficits permanent disability renal insufficiency or renal failure (including acute kidney injury) mitral valve regurgitation or injury tissue erosion vascular access related complications (e.g., dissection, perforation, pain, bleeding, hematoma, pseudoaneurysm, irreversible nerve injury, compartment syndrome, arteriovenous fistula, stenosis) conduction system disturbances (e.g., atrioventricular node block, left- bundle branch block, asystole), which may require a permanent pacemaker CAUTION : Federal (USA) law restricts this device to sale by or on the order of a physician. For further information, please call and/or consult Medtronic at the toll-free numbers or websites listed. Indications The Medtronic CoreValve system is indicated for relief of aortic stenosis in patients with symptomatic heart disease due to severe native calcific aortic stenosis (aortic valve area ≤1.0 cm2 or aortic valve area index ≤ 0.6cm2/m2, a mean aortic valve gradient of ≥40 mm Hg, or a peak aortic-jet velocity of ≥4.0 m/s) and with native anatomy appropriate for the 23, 26, 29 or 31mm valve system who are judged by a heart team, including a cardiac surgeon, to be at extreme risk or inoperable for open surgical therapy (predicted risk of operative mortality and/or serious irreversible morbidity ≥50% at 30 days). Contraindications The CoreValve system is contraindicated for patients presenting with any of the following conditions: known hypersensitivity or contraindication to aspirin, heparin (HIT/HITTS) and bivalirudin, ticlopidine, clopidogrel, Nitinol (Titanium or Nickel), or sensitivity to contrast media, which cannot be adequately premedicated ongoing sepsis, including active endocarditis preexisting mechanical heart valve in aortic position Warnings General Implantation of the Medtronic CoreValve system should be performed only by physicians who have received Medtronic CoreValve training. This procedure should only be performed where emergency aortic valve surgery can be performed promptly. Mechanical failure of the delivery catheter system and/or accessories may result in patient complications. Transcatheter Aortic Valve (Bioprosthesis) Accelerated deterioration of the bioprosthesis may occur in patients presenting with an altered calcium metabolism. Precautions General The safety and effectiveness of the Medtronic CoreValve system have not been evaluated in the pediatric population. The safety and effectiveness of the bioprosthesis for aortic valve replacement have not been evaluated in the following patient populations: without Aortic Stenosis (AS) who are at high, moderate, or low surgical risk (predicted perioperative mortality risk of 29 mm per the baseline diagnostic imaging transarterial access not able to accommodate an 18-Fr sheath sinus of valsalva anatomy that would prevent adequate coronary perfusion moderate to severe mitral stenosis severe ventricular dysfunction with left ventricular ejection fraction (LVEF) <20% as measured by resting echocardiogram end-stage renal disease requiring chronic dialysis or creatinine clearance <20 cc/min symptomatic carotid or vertebral artery disease severe basal septal hypertrophy with an outflow gradient Prior to Use Exposure to glutaraldehyde may cause irritation of the skin, eyes, nose, and throat. Avoid prolonged or repeated exposure to the vapors. Damage may result from forceful handling of the catheter. Prevent kinking of the catheter when removing it from the packaging. This device was designed for single patient use only. Do not reuse, reprocess, or resterilize this product. Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and/or create a risk of contamination of the device, which could result in patient injury, illness, or death. The bioprosthesis size must be appropriate to fit the patient’s anatomy. Proper sizing of the device is the responsibility of the physician. Refer to Instructions for Use for available sizes. Failure to implant a device within the sizing matrix could lead to adverse effects such as those listed in Section 5.0. Patients must present with femoral or subclavian/axillary access vessel diameters of ≥6 mm or an ascending aortic (direct aortic) access site ≥60 mm from the basal plane. Implantation of the bioprosthesis should be avoided in patients with aortic root angulation (angle between plane of aortic valve annulus and horizontal plane/vertebrae) of >30° for right subclavian/axillary access or >70° for femoral and left subclavian/axillary access. Use caution when using the subclavian/ axillary approach in patients with a patent LIMA graft or patent RIMA graft. During Use Adequate rinsing of the bioprosthesis with sterile saline, as described in the Instructions for Use, is mandatory before implantation. During rinsing, do not touch the leaflets or squeeze the bioprosthesis. If a capsule becomes damaged during loading or the capsule fails to close, replace the entire system (bioprosthesis, catheter, and CLS). Do not use a catheter with a damaged capsule. After a bioprosthesis has been inserted into a patient, do not attempt to reload that bioprosthesis on the same or any other catheter. During implantation, if resistance to deployment is encountered (e.g., the micro knob starts clicking or is tight or stuck), apply upward pressure to the macro slider while turning the micro knob. If the bioprosthesis still does not deploy, remove it from the patient and use another system. While the catheter is in the patient, ensure the guidewire is extending from the tip. Do not remove the guidewire from the catheter while the catheter is inserted in the patient. Once deployment is initiated, retrieval of the bioprosthesis from the patient (e.g., use of the catheter) is not recommended. Retrieval of a partially deployed valve using the catheter may cause mechanical failure of the delivery catheter system, aortic root damage, coronary artery damage, myocardial damage, vascular complications, prosthetic valve dysfunction (including device malposition), embolization, stroke, and/or emergent surgery. All brand names, product names or trademarks belong to their respective holders..")
73
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14 Resolute Integrity ZES Safety Information identified lesions ● Patients with tortuous vessels in the region of the target vessel or proximal to the lesion ● Patients with in-stent restenosis ● Patients with moderate or severe lesion calcification at the target lesion ● Patients with occluded target lesions including chronic total occlusions ● Patients with three-vessel disease ● Patients with a left ventricular ejection fraction of 2.5mg/dl ● Patients with longer than 24 months of follow-up The safety and effectiveness of the Resolute Integrity stent have not been established in the cerebral, carotid or peripheral vasculature. Potential Adverse Events Other risks associated with using this device are those associated with percutaneous coronary diagnostic (including angiography and IVUS) and treatment procedures. These risks (in alphabetical order) may include but are not limited to: ● Abrupt vessel closure ● Access site pain, hematoma or hemorrhage ● Allergic reaction (to contrast, antiplatelet therapy, stent material, or drug and polymer coating) ● Aneurysm, pseudoaneurysm or arteriovenous fistula (AVF) ● Arrhythmias, including ventricular fibrillation ● Balloon rupture ● Bleeding ● Cardiac tamponade ● Coronary artery occlusion, perforation, rupture or dissection ● Coronary artery spasm ● Death ● Embolism (air, tissue, device or thrombus) ● Emergency surgery: peripheral vascular or coronary bypass ● Failure to deliver the stent ● Hemorrhage requiring transfusion ● Hypotension/hypertension ● Incomplete stent apposition ● Infection or fever ● MI ● Pericarditis ● Peripheral ischemia/peripheral nerve injury ● Renal failure ● Restenosis of the stented artery ● Shock/pulmonary edema ● Stable or unstable angina ● Stent deformation, collapse or fracture ● Stent migration (or embolization) ● Stent misplacement ● Stroke/transient ischemic attack ● Thrombosis (acute, subacute or late) Adverse Events Related to Zotarolimus Patients’ exposure to zotarolimus is directly related to the total amount of stent length implanted. The actual side effects/complications that may be associated with the use of zotarolimus are not fully known. The adverse events that have been associated with the intravenous injection of zotarolimus in humans include but are not limited to: ● Anemia ● Diarrhea ● Dry skin ● Headache ● Hematuria ● Infection ● Injection site reaction ● Pain (abdominal, arthralgia, injection site) ● Rash Please reference appropriate product Instructions for Use for more information regarding indications, warnings, precautions and potential adverse events. CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician. For further information, please call and/or consult Medtronic at the toll-free numbers or websites listed. Indications The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is indicated for improving coronary luminal diameters in patients, including those with diabetes mellitus, with symptomatic ischemic heart disease due to de novo lesions of length ≤35 mm in native coronary arteries with reference vessel diameters of 2.25 mm to 4.20 mm. Contraindications The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is contraindicated for use in: ● Patients with a known hypersensitivity or allergies to aspirin, heparin, bivalirudin, clopidogrel, prasugrel, ticagrelor, ticlopidine, drugs such as zotarolimus, tacrolimus, sirolimus, everolimus or similar drugs or any other analogue or derivative ● Patients with a known hypersensitivity to the cobalt-based alloy (cobalt, nickel, chromium and molybdenum) ● Patients with a known hypersensitivity to the BioLinx ® polymer or its individual components Coronary artery stenting is contraindicated for use in: ● Patients in whom antiplatelet and/or anticoagulation therapy is contraindicated ● Patients who are judged to have a lesion that prevents complete inflation of an angioplasty balloon or proper placement of the stent or stent delivery system Warnings ● Please ensure that the inner package has not been opened or damaged as this would indicate the sterile barrier has been breached. ● The use of this product carries the same risks associated with coronary artery stent implantation procedures, which include subacute and late vessel thrombosis, vascular complications and/or bleeding events. ● This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy. Precautions ● Only physicians who have received adequate training should perform implantation of the stent. ● Stent placement should only be performed at hospitals where emergency coronary artery bypass graft surgery can be readily performed. ● Subsequent stent restenosis or occlusion may require repeat catheter-based treatments (including balloon dilatation) of the arterial segment containing the stent. The long-term outcome following repeat catheter-based treatments of previously implanted stents is not well characterized. ● The risks and benefits of the stent implantation should be assessed for patients with a history of severe reaction to contrast agents. ● Do not expose or wipe the product with organic solvents such as alcohol. ● When drug-eluting stents (DES) are used outside the specified Indications for Use, patient outcomes may differ from the results observed in the RESOLUTE pivotal clinical trials. ● Compared to use within the specified Indications for Use, the use of DES in patients and lesions outside of the labeled indications, including more tortuous anatomy, may have an increased risk of adverse events, including stent thrombosis, stent embolization, myocardial infarction (MI) or death. ● Care should be taken to control the position of the guide catheter tip during stent delivery, deployment and balloon withdrawal. Before withdrawing the stent delivery system, visually confirm complete balloon deflation by fluoroscopy to avoid guiding catheter movement into the vessel and subsequent arterial damage. ● Stent thrombosis is a low- frequency event that is frequently associated with MI or death. Data from the RESOLUTE clinical trials have been prospectively evaluated and adjudicated using the definition developed by the Academic Research Consortium (ARC). The safety and effectiveness of the Resolute Integrity stent have not yet been established in the following patient populations: ● Patients with target lesions which were treated with prior brachytherapy or the use of brachytherapy to treat in-stent restenosis of a Resolute Integrity stent ● Women who are pregnant or lactating ● Men intending to father children ● Pediatric patients ● Patients with coronary artery reference vessel diameters of 4.20 mm ● Patients with coronary artery lesions longer than 35 mm or requiring more than one Resolute Integrity stent ● Patients with evidence of an acute MI within 72 hours of intended stent implantation ● Patients with vessel thrombus at the lesion site ● Patients with lesions located in a saphenous vein graft, in the left main coronary artery, ostial lesions or bifurcation lesions ● Patients with diffuse disease or poor flow distal to All brand names, product names or trademarks belong to their respective holders.
 and treatment procedures. These risks (in alphabetical order) may include but are not limited to: ● Abrupt vessel closure ● Access site pain, hematoma or hemorrhage ● Allergic reaction (to contrast, antiplatelet therapy, stent material, or drug and polymer coating) ● Aneurysm, pseudoaneurysm or arteriovenous fistula (AVF) ● Arrhythmias, including ventricular fibrillation ● Balloon rupture ● Bleeding ● Cardiac tamponade ● Coronary artery occlusion, perforation, rupture or dissection ● Coronary artery spasm ● Death ● Embolism (air, tissue, device or thrombus) ● Emergency surgery: peripheral vascular or coronary bypass ● Failure to deliver the stent ● Hemorrhage requiring transfusion ● Hypotension/hypertension ● Incomplete stent apposition ● Infection or fever ● MI ● Pericarditis ● Peripheral ischemia/peripheral nerve injury ● Renal failure ● Restenosis of the stented artery ● Shock/pulmonary edema ● Stable or unstable angina ● Stent deformation, collapse or fracture ● Stent migration (or embolization) ● Stent misplacement ● Stroke/transient ischemic attack ● Thrombosis (acute, subacute or late) Adverse Events Related to Zotarolimus Patients’ exposure to zotarolimus is directly related to the total amount of stent length implanted. The actual side effects/complications that may be associated with the use of zotarolimus are not fully known. The adverse events that have been associated with the intravenous injection of zotarolimus in humans include but are not limited to: ● Anemia ● Diarrhea ● Dry skin ● Headache ● Hematuria ● Infection ● Injection site reaction ● Pain (abdominal, arthralgia, injection site) ● Rash Please reference appropriate product Instructions for Use for more information regarding indications, warnings, precautions and potential adverse events. CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician. For further information, please call and/or consult Medtronic at the toll-free numbers or websites listed. Indications The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is indicated for improving coronary luminal diameters in patients, including those with diabetes mellitus, with symptomatic ischemic heart disease due to de novo lesions of length ≤35 mm in native coronary arteries with reference vessel diameters of 2.25 mm to 4.20 mm. Contraindications The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is contraindicated for use in: ● Patients with a known hypersensitivity or allergies to aspirin, heparin, bivalirudin, clopidogrel, prasugrel, ticagrelor, ticlopidine, drugs such as zotarolimus, tacrolimus, sirolimus, everolimus or similar drugs or any other analogue or derivative ● Patients with a known hypersensitivity to the cobalt-based alloy (cobalt, nickel, chromium and molybdenum) ● Patients with a known hypersensitivity to the BioLinx ® polymer or its individual components Coronary artery stenting is contraindicated for use in: ● Patients in whom antiplatelet and/or anticoagulation therapy is contraindicated ● Patients who are judged to have a lesion that prevents complete inflation of an angioplasty balloon or proper placement of the stent or stent delivery system Warnings ● Please ensure that the inner package has not been opened or damaged as this would indicate the sterile barrier has been breached. ● The use of this product carries the same risks associated with coronary artery stent implantation procedures, which include subacute and late vessel thrombosis, vascular complications and/or bleeding events. ● This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy. Precautions ● Only physicians who have received adequate training should perform implantation of the stent. ● Stent placement should only be performed at hospitals where emergency coronary artery bypass graft surgery can be readily performed. ● Subsequent stent restenosis or occlusion may require repeat catheter-based treatments (including balloon dilatation) of the arterial segment containing the stent. The long-term outcome following repeat catheter-based treatments of previously implanted stents is not well characterized. ● The risks and benefits of the stent implantation should be assessed for patients with a history of severe reaction to contrast agents. ● Do not expose or wipe the product with organic solvents such as alcohol. ● When drug-eluting stents (DES) are used outside the specified Indications for Use, patient outcomes may differ from the results observed in the RESOLUTE pivotal clinical trials. ● Compared to use within the specified Indications for Use, the use of DES in patients and lesions outside of the labeled indications, including more tortuous anatomy, may have an increased risk of adverse events, including stent thrombosis, stent embolization, myocardial infarction (MI) or death. ● Care should be taken to control the position of the guide catheter tip during stent delivery, deployment and balloon withdrawal. Before withdrawing the stent delivery system, visually confirm complete balloon deflation by fluoroscopy to avoid guiding catheter movement into the vessel and subsequent arterial damage. ● Stent thrombosis is a low- frequency event that is frequently associated with MI or death. Data from the RESOLUTE clinical trials have been prospectively evaluated and adjudicated using the definition developed by the Academic Research Consortium (ARC). The safety and effectiveness of the Resolute Integrity stent have not yet been established in the following patient populations: ● Patients with target lesions which were treated with prior brachytherapy or the use of brachytherapy to treat in-stent restenosis of a Resolute Integrity stent ● Women who are pregnant or lactating ● Men intending to father children ● Pediatric patients ● Patients with coronary artery reference vessel diameters of 4.20 mm ● Patients with coronary artery lesions longer than 35 mm or requiring more than one Resolute Integrity stent ● Patients with evidence of an acute MI within 72 hours of intended stent implantation ● Patients with vessel thrombus at the lesion site ● Patients with lesions located in a saphenous vein graft, in the left main coronary artery, ostial lesions or bifurcation lesions ● Patients with diffuse disease or poor flow distal to All brand names, product names or trademarks belong to their respective holders..")
74
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14

75
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved UC201503127EN 10/14

Similar presentations


































>")





