Download presentation
Presentation is loading. Please wait.

1
HITECH, Meaningful Use, and Interoperability

2
HITECH Health Information Technology for Economic and Clinical Health – HITECH –Part of the 2009 American Recovery and Reinvestment Act –In February 2010 $750 million in grants and contracts went to agencies in 40 states and to 30 nonprofit organizations to “facilitate the exchange of health information.” –Also $225 million to 55 training programs to help train people for jobs in the health care and Health IT sectors.

3
HITECH Carrots and Sticks –The carrots: $14-27 billion will go to physicians, hospitals and other providers in the form of bonuses on their Medicare and Medicaid payments. –Fiscal year 2011 (October 2010) to hospitals –January 2011 physicians (up to $44,000 per physician under the Medicare portion, $63,000 under Medicaid) –If they can demonstrate that they are making “meaningful use” of health IT in addition to merely purchasing it and installing it. –Then comes the stick In 2015 or 2016 payments will be replaced by penalties for those not showing meaningful use.
 to hospitals –January 2011 physicians (up to $44,000 per physician under the Medicare portion, $63,000 under Medicaid) –If they can demonstrate that they are making meaningful use of health IT in addition to merely purchasing it and installing it. –Then comes the stick In 2015 or 2016 payments will be replaced by penalties for those not showing meaningful use..")
4
HITECH Responsibility for implementing provisions held by HHS Office of the National Coordinator for Health IT –Dr. Karen B. DeSalvo, MD, MPH, MSc –August 2010 plan for certifying electronic health record systems was released. Functional Interoperable Secure

6
Defining Meaningful Use

7
One Step Forward, Two Steps Back Federal officials revised the timeline to allow Stage 2 to be extended through 2016 and Stage 3 to begin in 2017 for the providers that have completed at least two years in Stage 2. Many were reported to be surprised by the complexities' of Stage 2 requirements, and some EHR makers were showing signs of “certification fatigue.”

8
Defining Meaningful Use Stage 1 (some started in 2011) –focuses on electronically capturing health information in a coded format –using that information to track key clinical conditions and communicating that information for care coordination purposes (whether that information is structured or unstructured) –implementing clinical decision support tools to facilitate disease and medication management and reporting clinical quality measures and public health information
 –focuses on electronically capturing health information in a coded format –using that information to track key clinical conditions and communicating that information for care coordination purposes (whether that information is structured or unstructured) –implementing clinical decision support tools to facilitate disease and medication management and reporting clinical quality measures and public health information")
9
Stage 1 Reporting through attestation Objectives and clinical quality measures Reporting may be through yes/no or numerator/denominator attestation

10
Stage 1 Eligible professionals must complete –15 core objectives –5 out of 10 from menu set –6 clinical quality measures 3 core and 3 out of 38 from additional set Hospitals must complete –14 core objectives –5 out of 10 from a menu set –15 clinical quality measures

11
MU Stage 1 Core Set of Objectives Health Outcomes Policy Priority ObjectiveMeasure Improving quality, safety, efficiency, and reducing health disparities Use CPOE for medication orders directly entered by an licensed healthcare professional More than 30% of unique patients with at least one medication in their medication list have at least one medication entered using CPOE Implement drug-drug and drug-allergy interaction checks This functionality is enabled for the entire EHR reporting period (physicians only): generate and transmit permissible prescriptions electronically (eRx) More than 40% of all permissible prescriptions are transmitted electronically using certified EHR technology Record demographicsMore than 50% of all unique patients have demographics as recorded structured data Maintain up-to-date problem list of current and active diagnoses More than 80% have at least one entry or an indication that no problems are known for the patient recorded as structured data
: generate and transmit permissible prescriptions electronically (eRx) More than 40% of all permissible prescriptions are transmitted electronically using certified EHR technology Record demographicsMore than 50% of all unique patients have demographics as recorded structured data Maintain up-to-date problem list of current and active diagnoses More than 80% have at least one entry or an indication that no problems are known for the patient recorded as structured data")
12
MU Stage 1 Core Set of Objectives Health Outcomes Policy Priority ObjectiveMeasure Improving quality, safety, efficiency, and reducing health disparities Maintain active medication listMore than 80% of patients have at least one entry recorded as structured data Maintain active medication allergy list More than 80% of patients have at least one entry recorded as structured data Record and chart vital signsFor more than 50% of patients age 2 and over, height, weight, and blood pressure are recorded Record smoking status for patients 13 years old or older More than 50% have smoking status recorded as structured data Implement one clinical decision support rule and the ability to track compliance with the rule Implement one clinical decision support rule Report clinical quality measures to CMS or the States Electronically submit clinical quality measures

13
MU Stage 1 Core Set of Objectives Health Outcomes Policy Priority ObjectiveMeasure Engage patients and families in their healthcare Provided patients with an electronic copy of the HI, upon request More than 50% of all patients who request an electronic copy are provided it within 3 business days. Hospitals: provided patients with an electronic copy of their discharge instructions at time of discharge, upon request More than 50% of patients who are discharged who request and electronic copy are provided it. Physicians: provided clinical summaries for each office visit Clinical summaries provided within 3 business days. Improve care coordination Capability to exchange key clinical information among providers of care and patient authorized entities electronically Performed at least one test of the certified EHR technology’s capacity to electronically exchange key clinical info Ensure adequate privacy and security Protect EHI created or maintained by certified EHR technology through the implementation of appropriate technical capabilities Conduct or review a security risk analysis and implement updates as necessary and correct identified security deficiencies as part of the risk management process

14
MU Stage 1 Menu Set Objectives 5 of 10 PhysiciansHospitals Drug formulary checks Incorporate clinical lab test results as structured data Generate lists of patients by specific conditions Use certified EHR technology to identify patient-specific education resources Medication reconciliation Summary of care record for each transition of care

15
MU Stage 1 Menu Set Objectives 5 of 10 PhysiciansHospitals Capability to submit electronic data to immunization registries/systems Capability to provide electronic syndromic surveillance data to public health agencies Send reminders to patients per patient preference for preventative/follow up care Record advanced directives for patients 65 or older Provide patients with timely electronic access to their HI Capability to provide electronic submission of reportable lab results to public health agencies

17
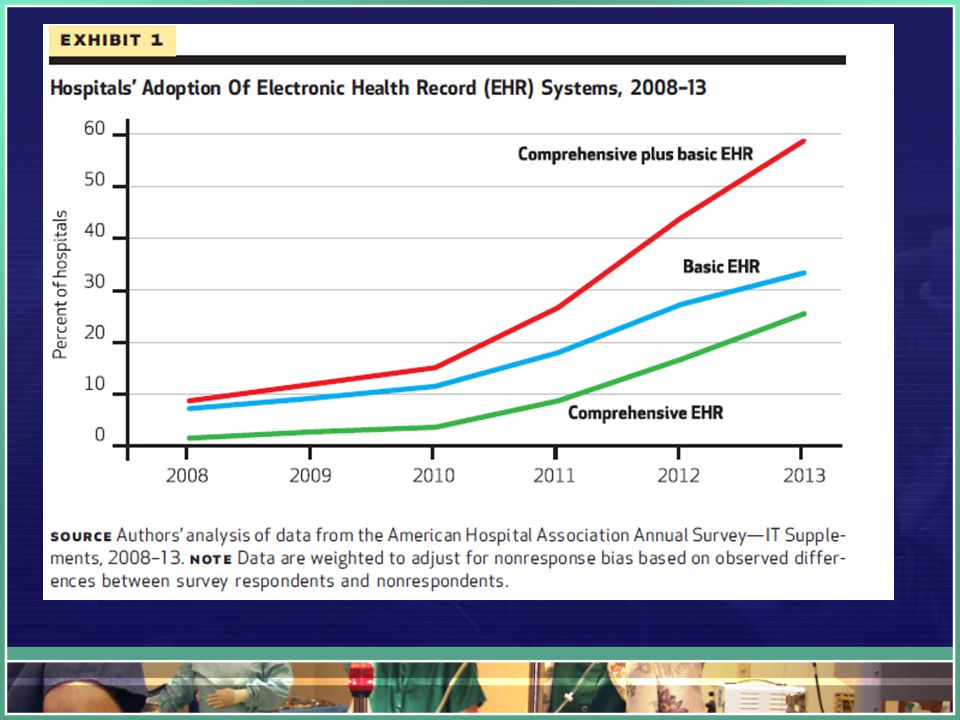
Effect of HITECH on EHR Adoption Significant increase in adoption between 2011 and 2012 Although a majority of hospitals did not achieve MU Small and Critical Access hospitals are at the most risk to fail –Low patient volume means fewer resources –Difficulty recruiting and retaining skilled IT personnel –Those that are recruited will be asked to become experts in all areas of IT (hardware, software, networking, security) rather than specializing. –Suitable IT vendor may be tough – vendors will tend to focus on larger institutions with larger budgets

18
Defining Meaningful Use Stage 2 (2014) –encourages the use of health IT for continuous quality improvement at the point of care and the exchange of information in the most structured format possible Some Stage 1 objectives were either combined or eliminated, most of the Stage 1 objectives are now core objectives under the Stage 2 criteria.
 –encourages the use of health IT for continuous quality improvement at the point of care and the exchange of information in the most structured format possible Some Stage 1 objectives were either combined or eliminated, most of the Stage 1 objectives are now core objectives under the Stage 2 criteria.")
19
Defining Meaningful Use For many of these Stage 2 objectives, the threshold that providers must meet for the objective has been raised. Some new objectives were also introduced for Stage 2, and most of these were introduced as menu objectives for Stage 2.

21
Stage 2 vs. Stage 1 New Stage 2 Core Objectives: –Use secure electronic messaging to communicate with patients on relevant health information (for EPs only) –Automatically track medications from order to administration using assistive technologies in conjunction with an electronic medication administration record (eMAR) (for Eligible Hospitals)
 –Automatically track medications from order to administration using assistive technologies in conjunction with an electronic medication administration record (eMAR) (for Eligible Hospitals).")
22
Interoperability Four areas of EHR technology that are important to consider –How applications interact with EHR system users (such as ordering labs) –How systems communicate with each other (such as messaging standards) –How information is processed and managed (such as data import into an EHR) –How consumer devices integrate with other systems and applications (such as tablet PCs for secure messaging)
 –How systems communicate with each other (such as messaging standards) –How information is processed and managed (such as data import into an EHR) –How consumer devices integrate with other systems and applications (such as tablet PCs for secure messaging)")
23
Interoperability National Coordinator for HIT: –Interoperability ensures that health-related information flows seamlessly from General Practitioner, to Specialist, to Hospital, to Patient. –Regardless of geographic, organizational, or vendor boundaries –Interoperability refers to the architecture or standards that make it possible for diverse EHR systems to work compatibly in a true information network –One of the key distinctions between Stage 1 and Stage 2 is that the bar is raised for interoperability

24
Stage 2 vs. Stage 1 Stage 2 criteria place an emphasis on health information exchange between providers to improve care coordination for patients. –Providers who transition or refer a patient to another setting of care or provider of care must provide a summary of care record for more than 50% of those transitions of care and referrals. –For more than 10% of transitions and referrals must provide a summary of care record electronically. –The physician or hospital that transitions or refers their patient to another setting of care or provider of care must either a) conduct one or more successful electronic exchanges of a summary of care record with a recipient using technology that was designed by a different EHR developer than the sender's, or b) conduct one or more successful tests with the CMS-designated test EHR during the EHR reporting period.
 conduct one or more successful electronic exchanges of a summary of care record with a recipient using technology that was designed by a different EHR developer than the sender s, or b) conduct one or more successful tests with the CMS-designated test EHR during the EHR reporting period..")
25
Stage 2 vs. Stage 1 Stage 2 also replaces the previous Stage 1 objectives to provide electronic copies of health information or discharge instructions and provide timely access to health information with objectives that allow patients to access their health information online. Stage 2 Patient Access Objectives: –Provide patients the ability to view online, download and transmit their health information within four business days of the information being available to the EP (for EPs only) –Provide patients the ability to view online, download and transmit their health information within 36 hours after discharge from the hospital (for Eligible Hospitals)
 –Provide patients the ability to view online, download and transmit their health information within 36 hours after discharge from the hospital (for Eligible Hospitals).")
26
Stage 2 vs. Stage 1 There are also new items in the menu lists Additional Clinical Quality Measures, including 1. Patient and Family Engagement 2. Patient Safety 3. Care Coordination 4. Population and Public Health 5. Efficient Use of Healthcare Resources 6. Clinical Processes/Effectiveness

27
Paper Discussion More than half of US hospitals have at least a basic HER, but stage 2 criteria remain challenging for most –Adler-Milstein et al.

28
Basic vs comprehensive EHR Basic – all 10 in at least one clinical unit –Patient demographics, physician notes, nursing assessment, patient problems list, medication lists, discharge summaries, lab results, radiologic reports, diagnostic test results, ordering medication Comprehensive – Basic plus 14 additional

30
Results More likely to have basic or comprehensive if: –Large, urban, nonprofit, teaching Critical access less likely to have comprehensive Early adopters tend to be large, major teaching, not-for profit, urban.

31
Meeting Stage 2

32
Stage 2 Challenges: ICD-10 and other reform –Providers and Venders both have lots of plates in the air Vendor Readiness –For providers to achieve meaningful use, they must use an EHR certified by an ONC-authorized testing body. –Hundreds or even thousands of complete EHRs and EHR modules certified for Stage 1 have not been upgraded to Stage 2 standards, potentially leaving customers in the uncomfortable position of having to change vendors in midstream.

33
Stage 2 Challenges: EHR Usability –Part of the certification process includes a usability test, but the rules for this are vague –Testers go out and observe users and then report back to the certifiers. –Also leads to some perverse incentives

34
Stage 2 Challenges: Interoperability –A particular sticking point is with laboratories. The Stage 2 rules require EHRs to be capable of accepting coded lab data. But there's nothing compelling laboratories to put lab reports in the correct format –Electronic communication between professionals Sending PHI over standard email Irrelevance to Specialists Many of the requirements (smoking cessation, patient education, preventative care, patient engagement) are foreign to specialists
 are foreign to specialists.")
35
Stage 2 Challenges: Patient Engagement and Education –Particularly the provision that calls for 50 percent of patients to be given an electronic means of viewing, transmitting or downloading personal health data and for 5 percent of patients to take it upon themselves to be "engaged" by sending unsolicited electronic messages to their healthcare providers. –What is in it for the patient?

36
860 physicians, 63% “meaningful users” –Hypertension and Diabetes patients fared marginally better with MU providers –Asthma and Chronic depression patients fared significantly worse with MU providers –No other significant differences between patients treated by MU and non-MU providers The hope is that Stage 3 will “pack the punch”

37
Defining Meaningful Use Stage 3 (2016 2017) –focuses on promoting improvements in quality, safety and efficiency Improving quality, safety, and efficiency, leading to improved health outcomes Decision support for national high-priority conditions Patient access to self-management tools Access to comprehensive patient data through patient-centered HIE Improving population health
 –focuses on promoting improvements in quality, safety and efficiency Improving quality, safety, and efficiency, leading to improved health outcomes Decision support for national high-priority conditions Patient access to self-management tools Access to comprehensive patient data through patient-centered HIE Improving population health")
38
Stage 3 Attempt to simplify – move from more than 20 objectives to 8: 1. Protect electronic health information 2. e-Prescribing 3. Clinical decision support 4. Computerized provider order entry 5. Patient electronic access to their data 6. Coordination of care through patient engagement 7. Health information exchange 8. Public health reporting

39
Highlights of Stage 3 More than 25% of patients seen by an EP or discharged from a hospital or emergency department (ED) must "actively engage" with their electronic records. For more than 35% of patients seen by an EP or discharged from a hospital or ED, a secure message must be sent using the EHR's secure messaging function or in response to a secure message sent by the patient.

40
Highlights of Stage 3 Patient-generated data from a nonclinical setting must be incorporated into the EHR for more than 15% of patients seen by the EP or discharged from a hospital or ED. EPs and hospitals must use their EHR to create a summary of care and electronically exchange it with other providers for more than 50% of transitions of care and referrals.

41
Highlights of Stage 3 In more than 40% of these transitions of care, the provider has to incorporate in its EHR a summary of care from an EHR used by a different provider. In more than 80% of transitions of care, the provider has to perform a "clinical information reconciliation" that includes not only medications and allergies, but also problem lists.

42
Conclusions: HITECH Bridge to Nowhere? Or a Stepping Stone?

Similar presentations








 & Critical Access Hospitals (CAH)>")












