Download presentation
Presentation is loading. Please wait.

1
Arthritis in the Elderly Gerald F. Falasca, M.D. Johnson City, TN March 2013 “All the Pearls in 50 Minutes ”

2
GOALS Practical advice Up to date on mgt Hone diagnostic skills

3
DISEASES To Be Touched On Sjogren’s PMR DJD RA Gout

4
CASE 1 A 70 year old woman presents with widespread pain, stiffness and fatigue. She recently started keeping a water bottle at her bedside. Physical exam is remarkable for slight synovitis of hands & wrists, and presence of all fibromyalgia tender points.

5
CASE 1 – cont’d. Sed rate is 30 mm/hr but CRP is normal CRP at 0.7 mg/dl (nl 0 - 1.0 mg/dl) C4 ↑ at 36 mg/dl. RF, CCP & ANA are negative.
 C4 ↑ at 36 mg/dl. RF, CCP & ANA are negative..")
6
CASE 1 – cont’d. What is the most likely diagnosis? A.Polymyalgia rheumatica B.Rheumatoid arthritis C.Fibromyalgia D.Primary Sjogren syndrome E.Paraneoplastic syndrome

7
Causes of Pain All Over in the Elderly Polymyalgia rheumatica Statins Fibromyalgia Depression Sjogren’s Rheumatoid Lupus Osteoarthritis

8
Primary Sjogren’s Dry eyes, dry mouth Fatigue Pain all over No idea what is wrong with them You probably have some in your practice

9
Sjogren’s - History Use of eye drops? Can you eat crackers w/o water? Keep water on night table? Physical Exam: Nothing specific! –Sometimes small joint puffiness –Peripheral neuropathy

10
Sjogren’s - Lab SSA / SSB – insensitive ESR often up CRP high normal

11
Sjogren’s - TX Hydroxychloroquine Low-dose prednisone Methotrexate Rituximab Fibromyalgia treatments (for symptoms)
")
12
Polymyalgia Rheumatica 10-15% go on to GCA Respond well to treatment In other words, this is a potentially serious disease that is treatable.

13
PMR Pain all over; sudden onset. Age > 50 (usually >70!) Weight loss Shoulder limitation of motion (periarthritis) Proximal muscle tenderness Sed rate > 50 mm/hr Anemia
 Weight loss Shoulder limitation of motion (periarthritis) Proximal muscle tenderness Sed rate > 50 mm/hr Anemia.")
14
PREDNISONE in ELDERLY ↓K +, ↑glucose DEXA Calcium + Vit D T/C bisphosphonate Eye exams: cataracts & pressure

15
Amer. College of Rheum. Recommendations for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis 2010 Arthritis Care & Research, Vol. 62, No. 11, November 2010, pp 1515– 1526 DOI 10.1002/acr.20295

16
GOUT

17
The risk factors for gout were known to the ancients.

18
Risk Factors for Gout Obesity, metabolic syndrome Ethanol Diuretics Fructose ingestion Excessive purine ingestion

19
Ben Franklin (1706 -1790) "Be temperate in wine, in eating, girls, and sloth, or the Gout will seize you and plague you…" -- Franklin
 Be temperate in wine, in eating, girls, and sloth, or the Gout will seize you and plague you… -- Franklin")
20
Drugs Associated with Hyperuricemia Diuretics (loop and thiazide types) Low-dose aspirin Ethanol
 Low-dose aspirin Ethanol")
21
Hyperuricemia & Gout Serum Uric Acid (mg/dl) Annual Incidence of Gout (%) < 7.00.1 7.0 – 8.90.5 > 9.04.9
 Annual Incidence of Gout (%) < – >")
27
This is chronic refractory gout!

28
Amer. College of Rheum. Guidelines for Management of Gout. Part 1 & 2 Arthritis Care & Research, Vol. 64, No. 10, October 2012, pp 1431– 1461 DOI 10.1002/acr.21773

29
The Three Phases of Gout Treatment Treat acute attack Prevent new attacks Reduce uric acid level (sometimes)
")
30
Phase 1 - Termination NSAID Colchcine Intra-articular steroids Systemic steroids IL-1 inhibitor (off-label use)
")
31
NSAIDs Treatment of choice in otherwise healthy (elderly?) patient. Avoid in renal insufficiency and in peptic ulcer disease. Avoid salicylates (these cause swings in serum uric acid).
..")
32
Intra-Articular Steroids One or a few joints. Make sure infection not present.

33
Oral Colchicine 1.2 mg followed by 0.6 mg 2 hrs later. Loading dose same in renal insufficiency. Maintenance (preventive) dose 0.6 mg qd or bid. 0.3 mg 2-3 times per week in dialysis patients (preventive).
 dose 0.6 mg qd or bid. 0.3 mg 2-3 times per week in dialysis patients (preventive)..")
34
Systemic Steroids Polyarticular attacks or fever. Longstanding attacks (>3-5 days). Need divided doses. Taper over 7-10 days. Start prophylactic agent (colchicine) as soon as possible.
 as soon as possible..")
35
Adjunctive Measures Rest Ice Elevation Analgesics Anti-motility agents (if using colchicine or indomethacin) Continue hypouricemic agent if patient has been taking it.
 Continue hypouricemic agent if patient has been taking it.")
36
Phase 2 - Preventive Therapy Colchicine or NSAID. Always use when beginning a hypouricemic drug. Continue several weeks to years (depending on tophi, serum uric acid). Always use before surgery in previously gouty patient.
. Always use before surgery in previously gouty patient..")
37
Phase 3 - Hypouricemic Therapy Not every patient needs it. May not need it in: –Very elderly –Non-compliant –Infrequent attacks and no tophi May exacerbate attacks early on

38
Goals of Hypouricemic Treatment Aim for serum uric acid under 6, preferably near 5 for some chronic gouty patients. But remember: –allopurinol toxicity more likely with higher dose. –More likely with renal insufficiency.

39
Hypouricemic Agents Allopurinol Febuxostat Probenecid Losartan (off-label) Vitamin C (off-label) Pegloticase
 Vitamin C (off-label) Pegloticase")
40
Major Toxicities of Allopurinol Increased gout attacks early on (use prophylaxis) Rash (may be severe) Stevens-Johnson syndrome Vasculitis Hepatitis Renal failure (interstitial nephritis) Bone marrow suppression
 Rash (may be severe) Stevens-Johnson syndrome Vasculitis Hepatitis Renal failure (interstitial nephritis) Bone marrow suppression")
41
Allopurinol Hypersensitivity Syndrome Fever Rash Renal Failure Hepatic injury Leukocytosis Eosinophilia (the tipoff!) May be fatal. Hard to treat. Serious reactions to allopurinol reported in 1 of 260 patients. Arthritis Rheum 29:82, 1986

42
Febuxostat Non-xanthine inhibitor of XO and XD. Better tolerated than allopurinol. Lower uric acid levels than allopurinol (53% vs. 21% met target of 6.0 mg/dl). Better dissolution of tophi.
. Better dissolution of tophi..")
43
Tophus Reduction Mean Reduction in Tophus Area Becker MA. N Engl J Med. 2005 Dec 8;353(23):2450-61. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. Group % Area Reduction P Value Feb 80 mg83P =.08 (NS) Feb 120 mg66P = 0.16 (NS) Allop 300mg50
: Febuxostat compared with allopurinol in patients with hyperuricemia and gout. Group % Area Reduction P Value Feb 80 mg83P =.08 (NS) Feb 120 mg66P = 0.16 (NS) Allop 300mg50.")
44
Febuxostat vs. Allopurinol Percentage of Patients Achieving Serum Uric Acid < 6 mg/dl Study 1: Allopurinol dosed at 300 mg/d for Cl Cr ≥ 60 ml/min or 200 mg/d for 30 ≤ Cl Cr ≤ 59 ml/min.

45
Febuxostat: Best Use Allopurinol failures Renal insufficiency Tophaceous gout

46
Allopurinol & Febuxostat Drug Interactions Life threatening interaction with azathioprine, 6-mercaptopurine. –Reduce dose of purine analogue by approximately 2/3. Theophylline Other interactions also

47
Gout vs. Pseudogout Gout –hallux, ankle, knee, hand –younger, male Pseudogout –knee, wrist, ankle –older, female Almost any joint can be affected by either disease!

51
CPPD Deposition Wrist: triangular ligament Pelvis: symphysis pubis Knee: menisci Also: annulus fibrosis, articular capsules, bursae, ligaments, tendons

52
Clinical Associations with Psuedogout Aging Previous joint surgery Previous joint trauma Familial types Gout Amyloidosis Hyperpara Hemochromatosis Hypomagnesemia Familial hypocalciuric hypercalcemia Hypophosphatasia Wilson’s disease Ochronosis

53
Pseudo-DJD Pattern of CPPD 50% of CPPD patients. Wrists, MCPs, elbows, shoulders, knees. Note difference from usual DJD pattern. Heberden’s or Bouchard’s frequently found. May be acute or chronic.

54
Treatment of Acute Psuedogout Aspiration (more important than in gout!) Rest Intra-articular steroids NSAIDs Systemic steroids Colchicine? IL-1 Inhibitors?

55
Pseudogout Prevention Colchicine NSAID Magnesium? There’s no allopurinol for pseudogout (unfortunately).
..")
56
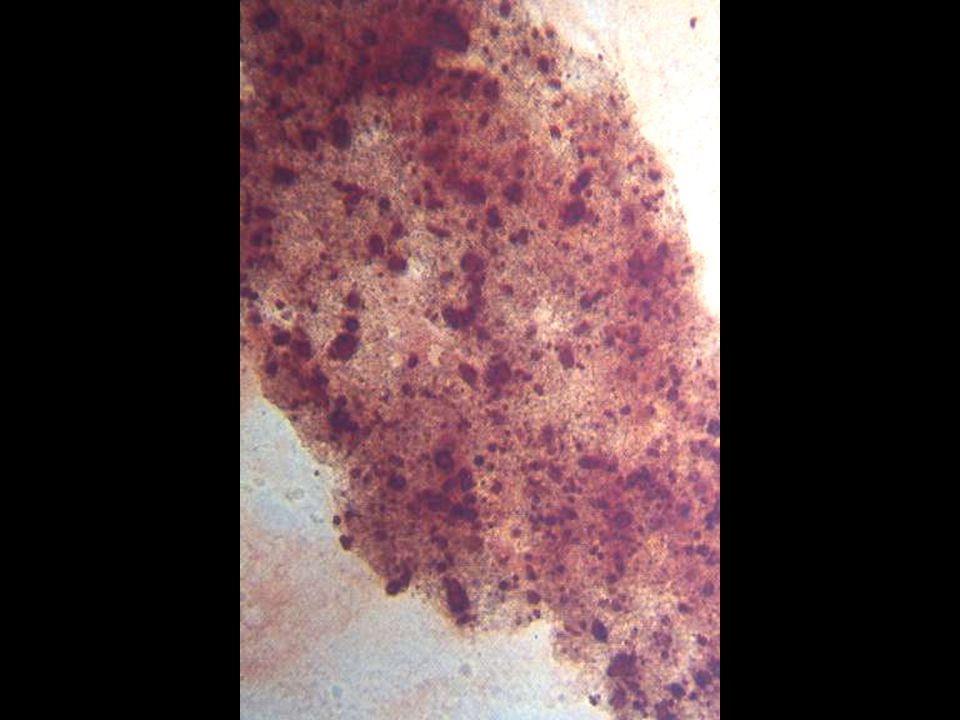
The Basic (Non-Acidic) Calcium Phosphates Hydroxyapatite Calcium carbonate Octacalcium phosphate Tricalcium phosphate (whitlockite) Hydroxyapatite is non- birefringent.
 Calcium Phosphates Hydroxyapatite Calcium carbonate Octacalcium phosphate Tricalcium phosphate (whitlockite) Hydroxyapatite is non- birefringent.")
58
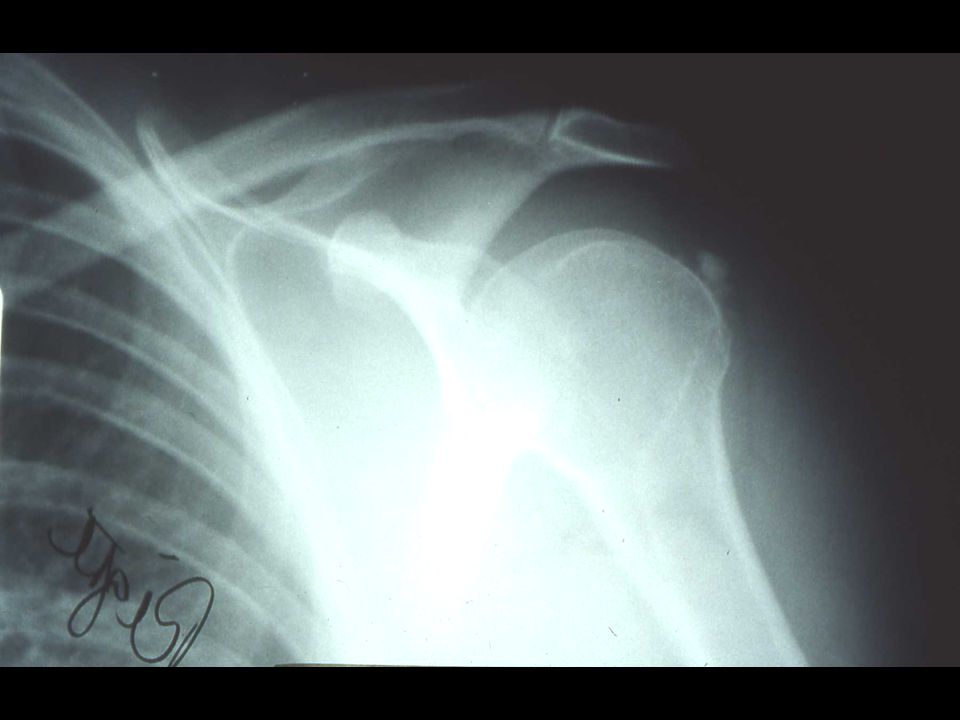
Syndromes Associated with Hydroxyapatite Acute monoarthritis (pseudopseudogout) Acute calcific tendinitis, bursitis Scleroderma, dermatomyositis Heterotopic calcification Milwaukee shoulder Crowned Dens Synd.
 Acute calcific tendinitis, bursitis Scleroderma, dermatomyositis Heterotopic calcification Milwaukee shoulder Crowned Dens Synd.")
59
Acute Apatite Monoarthritis (Pseudopseudogout) Is usually a peri-arthritis. Intense inflammation (looks septic) Synovial fluid often non- inflammatory. Often causes podagra (especially in younger women). Look for the telltale calcifications on radiographs.
 Synovial fluid often non- inflammatory. Often causes podagra (especially in younger women). Look for the telltale calcifications on radiographs..")
62
CROWNED DENS SYNDROME

63
Crowned Dens Synd Headache Pain with head rotation Shoulder myalgias Very elevated sed rate

64
RHEUMATOID ARTHRITIS In the Elderly

65
Rheumatoid Even in the elderly, completely new paradigm of treatment. Dual goals: –Symptom improvement –Prevention of structural damage

66
Rheumatoid “Small joint polyarthritis with morning stiffness” MCPs, wrists, MTPs ESR, CRP may or may not be up. RF or anti-CCP pos 70%

67
RA in the Elderly M:F ratio more nearly equal More shoulder involvement May overlap with polymyalgia rheumatoica

68
Initial Tx of RA Low dose prednisone (actually a good DMARD!) Methotrexate – safer than we expected in 1987! –Lung toxicity is possible –Follow liver enzymes –Added infection risk is relatively low (2-3%).
..")
70
What We Try to Prevent

71
The New Paradigm Is it likely that the patient will have destructive or debilitating disease in the long-term? If so, begin one or more DMARDs (often MTX). If inadequate response after 3 months, add or switch DMARDs, often includes a TNFI.
. If inadequate response after 3 months, add or switch DMARDs, often includes a TNFI..")
72
Anti-CCP CCP = cyclic citrullinated peptides RA synovium overproduces CCP RA patients THEN make ANTIBODIES to CCP 70% sensitive, 90% specific Anti-CCP is often present years before RA manifests itself.

73
Goals of the New Criteria Identify persons with “early arthritis” who are at high risk of erosive or debilitating disease. Allow for earlier disease modifying treatment. But…the criteria are not simple!

74
2010 ACR/EULAR CRITERIA FOR CLASSIFICATION OF RHEUMATOID ARTHRITIS Arthritis & Rheumatism 62(9): 2569–2581, 2010.
: 2569–2581, 2010.")
75
Lab Eval of Polyarthritis Rheum factor Anti-CCP ANA C4 Lyme CBC Chem-12 SSA, SSB Anti-RNP

76
Methotrexate Standard of care for RA. dihydrofolate reductase inhibitor. Best initial treatment for most patients. Avoid in pre-existing liver disease, renal disease and in drinkers. Main risk: pulmonary toxicity Higher doses being used, espec. Sub Q. 1/3 of patients will have little or no radiographic progression on MTX alone.

77
Methotrexate (cont’d) Always give only once a week, but dose may be split in two parts, and given 12 hours apart. Most persons should receive supplemental folate 1 mg/d. Follow liver enzymes (with albumin), CBC, creatinine monthly initially.
, CBC, creatinine monthly initially..")
78
Methotrexate - Side Effects Nausea, diarrhea Stomatitis Alopecia Rash Infections MTX pneumonitis Hepatitis Cirrhosis Pulm. fibrosis Pancytopenia Lymphoma? Don’t use if creatinine > 2.0!

79
TNF Inhibitors Potent inhibitors of inflammation Have revolutionized the treatment of RA since 1998. They retard erosions Act quickly Two approaches: monoclonal Ab vs. soluble receptor $$$$

80
Side Effects of TNF Inhibitors Rashes, especially inject. site rxns. Infections. Reactivation of tuberculosis. Demyelinating disease, optic neuritis, seizures. Pancytopenia. Congestive heart failure (effect may last for months). Malignancy (espec. lymphoma)
. Malignancy (espec. lymphoma).")
81
Prednisone Low dose prednisone: 7.5 mg/d Reduces number of erosions at two years in early RA (22% vs. 46%). N Engl J Med 1995 Jul 20;333(3):142-6.
. N Engl J Med 1995 Jul 20;333(3):")
82
Remission: The New Standard? Durable remissions are achievable with combination therapy. Definition of remission important however! Remission depends heavily on treating early (first year of disease) New trials may report the remission rate as the primary outcome measure
 New trials may report the remission rate as the primary outcome measure.")
83
RA Take Home Messages The treatment paradigm has changed in the past 10-15 years. Aggressive treatment changes long-term outcome. The earlier treatment is started, the better. There are new tools to help us make an earlier diagnosis.

84
Osteoarthritis Everyone gets a little Minor degenerative changes on xray often meaningless Knee, 1 st CMC, DIPs, hip, back Usually localized –Exception: Erosive or inflammatory OA.

85
Nonpharmacologic Therapy for Patients with OA Amer. Coll. Of Rheumatology Patient education Self-management programs (e.g., Arthritis Foundation Self-Management Program) Personalized social support through telephone contact Weight loss (if overweight) Aerobic exercise programs Physical therapy Range-of-motion exercises Muscle-strengthening exercises Assistive devices for ambulation Patellar taping Appropriate footwear Lateral-wedged insoles (for genu varum) Bracing Occupational therapy Joint protection and energy conservation Assistive devices for activities of daily living http://www.rheumatology.org/practice/clinical/guidelines/oa-mgmt.asp
 Personalized social support through telephone contact Weight loss (if overweight) Aerobic exercise programs Physical therapy Range-of-motion exercises Muscle-strengthening exercises Assistive devices for ambulation Patellar taping Appropriate footwear Lateral-wedged insoles (for genu varum) Bracing Occupational therapy Joint protection and energy conservation Assistive devices for activities of daily living")
86
Pharmacologic Therapy for Patients with OA Amer. Coll. Of Rheumatology Acetaminophen COX-2-specific inhibitor Nonselective NSAID [plus misoprostol or a proton pump inhibitor if at ↑GI risk] Non-acetylated salicylate Other pure analgesics: Tramadol Opioids Intraarticular glucocorticoids, hyaluronan Topical Capsaicin Methylsalicylate http://www.rheumatology.org/practice/clinical/guidelines/oa-mgmt.asp

87
OA of the Knee Most sensitive and specific finding on physical exam: CREPITUS! Sometimes knee pain is coming from the hip

88
OA of Knee Glucosamine: mixed data Corticosteroid injection Viscosupplementation Quadriceps exercises Neoprene sleeve Hinged brace

89
OA of the Hip Joint Mimicked by low back pain! Most common cause of trochanteric bursitis is low back pain too! Hip pain usually radiates to groin, not to the “hip”.

90
Hip OA Injections don’t last long and are not practical. Hip replacement is a good operation.

91
1 st CMC Osteoarthritis Brace off-the-shelf Brace custom molded Surgery Liniment

92
NSAIDs Toxicity in Elderly Peptic ulcer disease Hypertension Congestive heart failure CNS changes Intestinal ulceration

93
GI Less Toxic NSAIDs Celecoxib Salsalate Meloxicam Nabumetone Etodolac

94
Risk Factors for UGI Events Amer. Coll. Of Rheumatology Age >=65 Comorbid medical conditions Oral glucocorticoids History of peptic ulcer disease History of upper gastrointestinal bleeding Anticoagulants http://www.rheumatology.org/practice/clinical/guidelines/oa-mgmt.asp

95
RISK FACTORS FOR ULCERS NSAID Use Age > 64 Prior event CHF Ethanol Warfarin Concomitant corticosteroid, low dose aspirin, bisphosphonate, SSRI H. pylori

96
Ann Rheum Dis. 2007 March; 66(3): 417–418. PREVALENCE OF NSAID ULCERS BY AGE
: 417–418. PREVALENCE OF NSAID ULCERS BY AGE")
98
PREVENTION OF NSAID ULCERS Arch Intern Med.Arch Intern Med. 2002 Jan 8;162(2):169-75
:169-75")
99
NSAID ULCER PROPHYLAXIS H2 blockers NOT recommended for prophylaxis PPI or misoprostol recommended PPI doesn’t seem to reduce celecoxib ulcer complications further. Low dose aspirin ELIMINATES any benefit of celecoxib.

100
Amer. Coll. Of Gastro. 2009 Patients with hx PUD should be tested for H. pylori prior to NSAID or ASA use.

101
Amer. Coll. Gastro. Guide. 2009 GI RISK CV RISK* HighModLow HighNo NSAID, no COX-2 Naproxen + (PPI or MIS) LowCOX-2 + (PPI or MIS) COX-2 or (NSAID + (PPI or MIS)) NSAID alone *High CV risk defined as those needing aspirin therapy.
 LowCOX-2 + (PPI or MIS) COX-2 or (NSAID + (PPI or MIS)) NSAID alone *High CV risk defined as those needing aspirin therapy..")
102
Prophylactic Regimens Misoprostol 200 mcg QID Lansoprazole 15 or 30 mg/d Esomeprazole 20 or 40 mg/d

103
CV Risk - Celecoxib 33 monthsAbs%RR Placebo6/6760.9%1.0 200 mg BID18/6832.6%2.6 400 mg BID23/6693.4%3.4 N Engl J Med. 2006;355(9):873.
:873..")
Similar presentations












 Immunomodulatory and immunosuppresive Xenobiotic – Gold salts – Azathioprine – Methotrexate Biological.>")








 Etiology is.>")








