Download presentation
Presentation is loading. Please wait.

1
Principles of Fracture Treatment

2
What is a (bony) fracture?
Disruption of a bone’s normal structure or “wholeness” Crack, break, or rupture in a bone There are many how’s and why’s to bony fractures Terms used to describe each are related

3
Definition of Fracture
There are 2 types of # in which this is not so: Pathological fract. Stress fract.

4
Pathological fracture :
It is one in which a bone is broken through an area weakened by pre-existing disease , & by a degree of force that would have left normal bone intact e.g osteoporosis , O.M. , bone tumours.

5
Stress fracture : Bone, like other materials, reacts to repeated loading. On occasion, it becomes fatigued & a crack develops e.g military installations, ballet dancers & athletes.

6
Diagnosis Clinical picture Radiography

7
Clinical Features of Fracture
History of trauma Symptoms & signs: 1. Pain & tenderness Swelling 3. Deformity Crepitus 5. Loss of function Abnormal move. 7. N.V. injuries

8
Orthopaedic History A good general orthopaedic history contains:
Onset, Duration, and Location of a problem Limitations and debilitation attributed to the problem Good surgical history, especially with regards to orthopaedic surgeries and prior anesthesia Co-morbid conditions that contribute to the problem or will preclude healing in some manner

9
Physical Exam Basics Inspect and Palpate everything- start with normal structures and move to abnormal Range of motion in all planes Strength Sensation Reflexes Gait Stability

10
Physical Exam Basics NVI What does this mean?
Neurologic exam- Always document the neurologic status. Some fractures are associated with nerve injuries and knowing the status of the nerve is critical Vascular exam- Always check for pulses distal to the fracture sight. Missed vascular injuries can be devastating

11
Pre-reading Musculoskeletal Radiographs
1: Name, date, old films for comparison 2: What type of view(s) 3: Identify bone(s) & joint(s) demonstrated 4: Skeletal maturity (physes: growth plates) 5: Soft tissue swelling 6: Bones & joints (fractures & dislocations)
 3: Identify bone(s) & joint(s) demonstrated. 4: Skeletal maturity. (physes: growth plates) 5: Soft tissue swelling. 6: Bones & joints. (fractures & dislocations)")
12
Physical Exam NEVER trust someone else’s exam. ALWAYS put your hands on the patient and see for yourself Always trust your exam- you WILL pick up something that someone else has missed at some point

14
OPEN AND CLOSED FRACTURES

16
Intro to Reading X-rays
Reading a radiograph is essentially describing the anatomy of a certain structure In order for it to be universal and understandable for others, clarity and precision are essential A fracture is described based on the findings of the physical exam and a review of radiographs

17
Reading X-rays Say what it is- what anatomic structure are you looking at and how many different views are there Regional Location- Diaphysis (rule of 1/3), Metaphysis, Epiphysis including intra and extra-articular Direction of the fracture line- Transverse, Oblique, Spiral
, Metaphysis, Epiphysis including intra and extra-articular. Direction of the fracture line- Transverse, Oblique, Spiral.")
18
Reading X-rays Condition of the bone- comminution (3 or more parts), Segmental (middle fragment), Butterfly segment, incomplete, avulsion, stress, impacted Deformity-Displacemtent (distal with respect to proximal), angulation (varus, valgus), rotation, shortening (in cm’s), distraction
, Segmental (middle fragment), Butterfly segment, incomplete, avulsion, stress, impacted. Deformity-Displacemtent (distal with respect to proximal), angulation (varus, valgus), rotation, shortening (in cm’s), distraction.")
19
Fracture Pattern Transverse Produced by a distracting or tensile force

20
Fracture Pattern Spiral Produced by a torsional force

21
Fracture Pattern Produced by pure bending force Butterfly

22
Fracture Pattern Comminuted
Broken into many pieces- high energy with combined forces

23
Displacement Characterized by % of bone contact on either view

24
Angulation Distal fragment relative to proximal
Varus, Valgus, Anterior, Posterior Apex of angle formed by fragments E.g., Apex Anterior, Apex Medial, Apex Ulnar

25
Location ie distal third of tibia
Commonly described in thirds of affected bone ie distal third of tibia ie junction of proximal and middle third of femur If fractured at two levels describe as segmental

26
Location-Diaphysis Shaft portion of bone

27
Location-Metaphysis The ends of the bone (if the fracture goes into a joint it is described as intra- articular)
")
28
Now All Together Transverse fracture of the femur at the middle third- distal third junction with 100% displacement and varus (or apex lateral) angulation
 angulation.")
29
What do you see?

30
What do you see?

31
What do you see?

32
Mnemonic: OLD ACID O: Open vs. closed L: Location
D: Degree (complete vs. incomplete) A: Articular extension C: Comminution / Pattern I: Intrinsic bone quality D: Displacement, angulation, rotation
 A: Articular extension. C: Comminution / Pattern. I: Intrinsic bone quality. D: Displacement, angulation, rotation.")
33
O: Open vs. Closed Open fracture Closed fracture
AKA: “Compound fracture” A fracture in which bone penetrates through skin; “Open to air” Some define this as a fracture with any open wound or soft tissue laceration near the bony fracture Closed fracture Fracture with intact overlying skin

34
L: Location Which bone? Thirds (long bones) Anatomic orientation
Epiphysis Which bone? Thirds (long bones) Proximal, middle, distal third Anatomic orientation E.g. proximal, distal, medial, lateral, anterior, posterior Anatomic landmarks E.g. head, neck, body / shaft, base, condyle Segment (long bones) Epiphysis, physis, metaphysis, diaphysis Physis Metaphysis Diaphysis (Shaft) Articular Surface
 Proximal, middle, distal third. Anatomic orientation. E.g. proximal, distal, medial, lateral, anterior, posterior. Anatomic landmarks. E.g. head, neck, body / shaft, base, condyle. Segment (long bones) Epiphysis, physis, metaphysis, diaphysis. Physis. Metaphysis. Diaphysis. (Shaft) Articular Surface.")
35
D: Degree of Fracture Complete Incomplete
Complete cortical circumference involved Fragments are completely separated Incomplete Not fractured all the way through “Only one cortex” involved e.g “Greenstick fracture”

36
A: Articular Extension / Involvement
Intra-articular fractures “Involves the articular surface” Dislocation Loss of joint surface / articular congruity Fracture-dislocation

37
C: Comminution / Pattern
Transverse (Simple) Oblique (Simple) Spiral (Simple) Linear / longitudinal Segmental Comminuted Compression / impacted “Buckle / Torus” Distraction / avulsion
 Oblique (Simple) Spiral (Simple) Linear / longitudinal. Segmental. Comminuted. Compression / impacted. Buckle / Torus Distraction / avulsion.")
38
C: Comminution / Pattern
Transverse (Simple)
")
39
C: Comminution / Pattern
Oblique (Simple) Spiral (Simple) Oblique in 2+ views
 Spiral (Simple) Oblique in 2+ views.")
40
C: Comminution / Pattern
Linear / longitudinal / split

41
C: Comminution / Pattern
Segmental Bone broken in 2+ separate places; Fx lines do not connect

42
C: Comminution / Pattern
Comminuted Broken, splintered, or crushed into >3 pieces

43
C: Comminution / Pattern
Compression Impacted (e.g. “Buckle / Torus”)
")
44
C: Comminution / Pattern
“Buckle / Torus”

45
C: Comminution / Pattern
Distracted Avulsion

46
I: Intrinsic Bone Quality
Normal Osteopenia Decr’d density

47
I: Intrinsic Bone Quality
Osteopetrosis Incr’d density Normal

48
I: Intrinsic Bone Quality
Osteopoikilosis Focal areas of incr’d density Normal

49
D: Displacement, Angulation, Rotation
Extent to which Fx fragments are not axially aligned Fragments shifted in various directions relative to each other Convention: describe displacement of distal fragment relative to proximal Oblique tibial shaft Fx b/w distal & middle thirds; laterally displaced

50
D: Displacement, Angulation, Rotation
Extent to which Fx fragments are not anatomically aligned In a angular fashion Convention: describe angulation as the direction the apex is pointing relative to anatomical long axis of the bone (e.g. apex medial, apex valgus) R Tibial shaft Fx b/w prox & middle thirds, angulated apex lateral (apex varus)
 R Tibial shaft Fx b/w prox & middle thirds, angulated apex lateral (apex varus)")
51
D: Displacement, Angulation, Rotation
Valgus Apex medial Parallel No angulation Varus Apex lateral

52
D: Displacement, Angulation, Rotation
Extent to which Fx fragments are rotated relative to each other Convention: describe which direction the distal fragment is rotated relative to the proximal portion of the bone

53
D: Displacement, Angulation, Rotation
PA view of rotated hip Fx Greater trochanter perpendicular to film Normal PA view of hip Greater trochanter in profile

54
Salter-Harris Fractures

55
Other signs of fractures
Callus / Osteosclerosis Periosteal reaction

56
Other signs of fractures
Fat pad sign / “Sail sign”

57
Conclusions Know how to read X-rays
(Patients expect this & we order a lot of them) Communicate and share with your consultants (It affects patient outcomes) Pre-reading Describing fractures
 Communicate and share with your consultants. (It affects patient outcomes) Pre-reading. Describing fractures.")
58
Fracture Classification
Anat. Location Direction of fract. Line Wherther the fract. Is linear or comminuted Condition of overlying S.T. Mechnism of injury AO classification

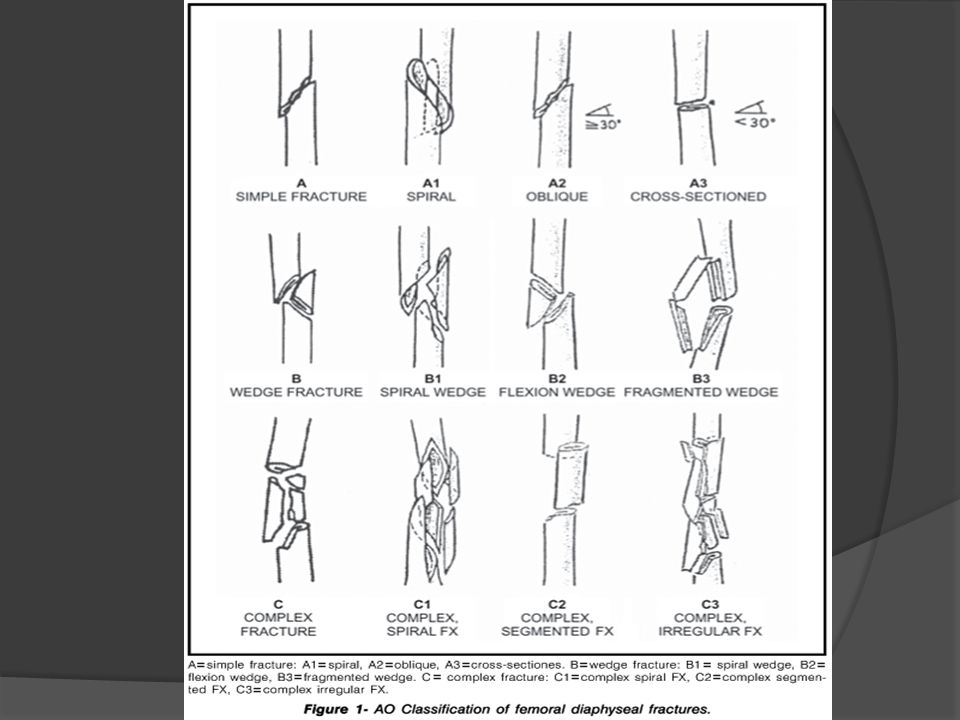
59
AO Classification A : Simple fract. B : Wedge fract.
C : Complex fract.

60
AO Classification

62
AO Classification B= wedge fract. B3 wedge fract fragmented wedge

63
AO Classification

66
Mechanism of Injury Classification
Direct trauma Indirect Trauma

67
Direct trauma : Tapping fractures Crushing fractures
Penetrating fractures - High velocity missiles > 2500 f/s - Low velocity missiles < 2500 f/s

68
Indirect Trauma : Traction or tension fract. angulation fract.
Rotational fract. Compression fract.

69
Principles of fractures Fracture repair
Fracture repair is a tissue regeneration process rather than a healing process the injured bone is replaced by bone. The process of repair varies according to: -The type of bone involved. -The amount of movement at the fracture. -The closeness of the fracture surfaces.

70
Principles of fractures Rate of union
Unfavorable factors Impairment of blood supply Infection Excessive movement Presence of tumor Synovial fluid in intraarticular Fx. Interposition of soft tissue Any form of Nicotine

71
Definitive fracture treatment
The goal of fracture treatment is to obtain union of the fracture in the most anatomical position compatible with maximal functional return of the extremity. Conservative Operative

72
Principles of Treatment
Treat the Patient, not only the fracture Restriction of movement Prevention of displacement Alleviation of pain Promote soft-tissue healing Try to allow free movement of the unaffected parts Splint the fracture, not the entire limb 72

73
Principles of Treatment
Methods of holding reduction: Sustained traction Cast splintage Functional bracing Internal fixation External fixation 73

74
Definitive Fracture Fixation Options
Casts and Splints Appropriate for many fractures especially hand and foot fractures Adults typically will get plaster splints initially transitioned to fiberglass casts as swelling decreases Kids typically will get fiberglass casts 74

76
CONSERVATIVE TREATMENT 2- CAST
CLOSED, UNDISPLACED CLOSED, REDUCIBLE CONSERVATIVE TREATMENT 2- CAST Below Knee Above Knee

77
Complications of cast splintage
Liable to appear once the patient has left the hospital; added risk of delay before the problem is attended to Tight cast Pressure sores Skin abrasion or laceration Loose cast 77

78
Functional Bracing Prevents joint stiffness while still permitting fracture splintage and loading Most commonly for fractures of the femur or tibia Since its not very rigid, it is usually applied only when the fracture is beginning to unite Comes out well on all four of the basic requirements: “hold” “move” “speed” “safe” 78

79
Definitive Fracture Fixation Options
Traction Useful in patients who are too sick for surgery Useful to maintain alignment until definitive fixation 79

80
Traction by gravity Balanced Traction Eg. Fractures of the humerus
Skin traction: adhesive strapping kept in place by bandages Skeletal traction: stiff wire/pin inserted through the bone distal to the fracture Femur fracture managed with skeletal traction and use of a Steinmann pin in the distal femur. 80

81
Operative ORIF (open reduction internal fixat.) External fixation
 External fixation")
82
Indications of ORIF - absolute - relative

83
Indications of ORIF Absolute Indications for ORIF of fractures
Unable to obtain an adequate reduction Displaced intra-articular fractures Certain types of displaced epiphyseal fractures Major avulsion fractures where there is loss of function of a joint or muscle group Non-unions Re- implantations of limbs or extremities

84
Indications of ORIF Relative Indications for ORIF of fractures
Delayed unions Multiple fractures to assist in care and general management Unable to maintain a reduction Pathological fractures To assist in nursing care To reduce morbidity due to prolonged immobilisation For fractures in which closed methods are known to be ineffective

85
Indications of ORIF Fractures accompanying nerve of vessel injury
Questionable Fractures accompanying nerve of vessel injury Open fractures Cosmetic considerations Economic considerations

86
Open Operation Operative reduction under direct vision is indicated:
When closed reduction fails When there is a large articular fragment that needs accurate positioning 86

87
Open Operation 3. For avulsion fractures in which the fragments are held apart by muscle pull 4. When an operation is needed for associated injuries 5. When a fracture will anyhow need internal fixation to hold it 87

89
Types of Internal Fixation
- Pin & wire fixat. - Screw fixat. - Plate & screws fixat. - Intra-medullary fixat.

90
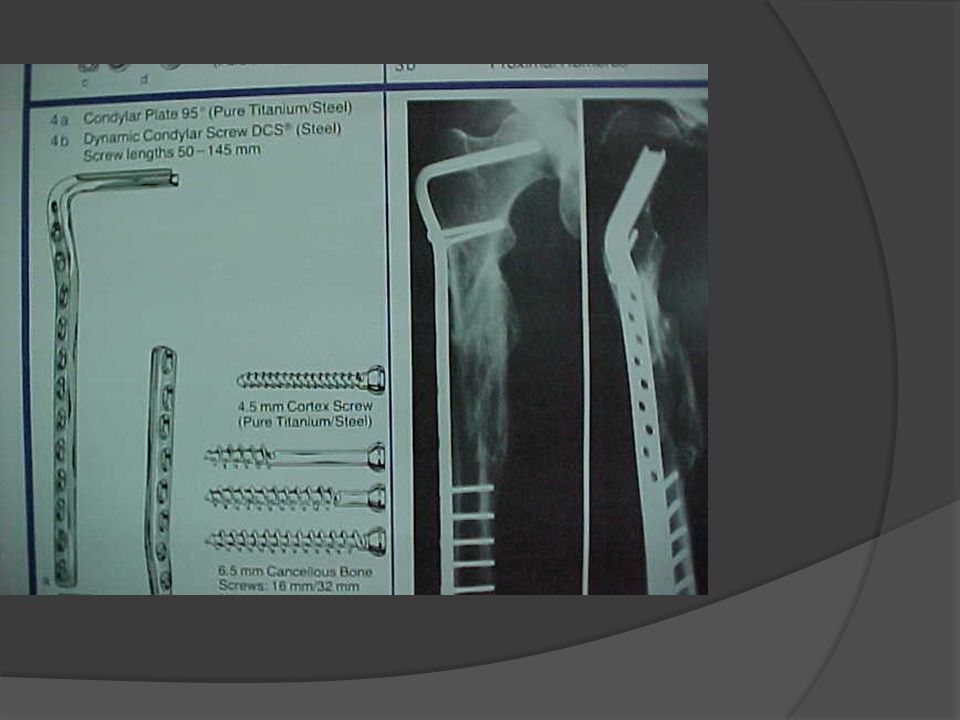
Plate & screws fixat. Functional types: Compression plates
Neutralization plates Buttress plates Bridge plates LC- DCP Liss plates Locking plates & screws

91
Definitive Fracture Fixation Options
Open Reduction and Internal fixation with Plates and screws Used for many fractures especially those involving joints 91

94
Intra-medullary fixat.
Centro-medullary - Unlocked -Interlocking(static – dynamic – double locked) Condylocephalic Cephalomedullary
 Condylocephalic. Cephalomedullary.")
95
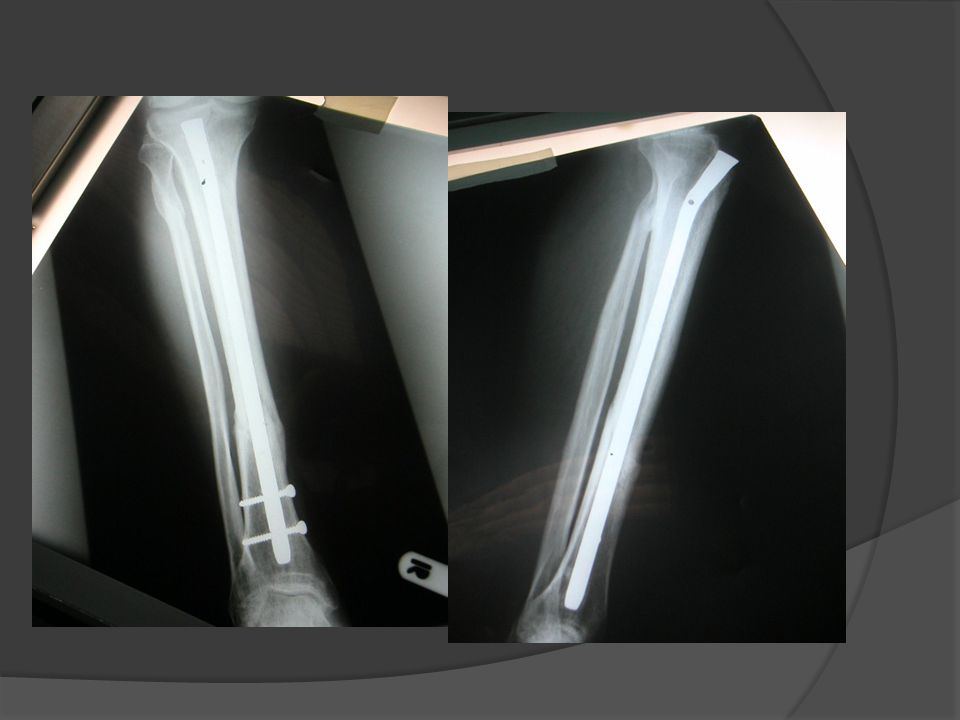
Definitive Fracture Fixation Options
Intramedullary Nails Treatment of choice for most tibia and femur fractures Used in selected humerus and forearm fractures 95

100
Internal Fixation “holds” securely with precise reduction
“movements” can begin at once (no stiffness and edema) “speed”: patient can leave hospital as soon as wound is healed, but full weight bearing is unsafe for some time “safety”= biggest problem! SEPSIS!!! Risk depends on: the patient, the surgeon, the facilities 100
 speed : patient can leave hospital as soon as wound is healed, but full weight bearing is unsafe for some time. safety = biggest problem! SEPSIS!!! Risk depends on: the patient, the surgeon, the facilities")
101
Indications for internal fixation
Fractures that cannot be reduced except by operation Fractures that are inherently unstable and prone to re-displacement after reduction Fractures that unite poorly and slowly Pathological fractures Multiple fractures Fractures in patients who present severe nursing difficulties 101

102
Interfragmentary/Lag Screws: Fixing small fragments onto the main bone
Plates and screws Metaphyseal fractures of long bones Diaphyseal fractures of the radius and ulna Intramedullary nails Long bones Locking screwsresist rotational forces Kirschner Wires Hold fragments together where fracture healing is predictably quick 102

103
Definitive Fracture Fixation Options
Joint Replacement Used in displaced femoral neck fractures in geriatric patients Allows for early ambulation Occasionally used in geriatric pts with comminuted shoulder or elbow fractures 103

104
Complications of internal fixation
Most are due to poor technique, equipment, or operating conditions Infection Iatrogenic infection is now the most common cause of chronic osteomyelitis Non-union Excessive stripping of the soft tissues unnecessary damage to the blood supply in the course of operative fixation rigid fixation with a gap between the fragments Implant failure Refracture 104

105
Definitive Fracture Fixation Options
External Fixation Used primarily in the treatment of open fractures and pelvis fractures Also useful as temporary stabilization prior to definitive fixation 105

106
External Fixation Permits adjustment of length and angulation
Some allow reduction of the fracture in all 3 planes. Especially applicable to the long bones and the pelvis. Indications: Fractures of the pelvis, which often cannot be controlled quickly by any other method. Fractures associated with severe soft-tissue damage where the wound can be left open for inspection, dressing, or definitive coverage. 106

107
External Fixation 3. Severely comminuted and unstable fractures, which can be held out to length until healing commences. 4. Fractures of the pelvis, which often cannot be controlled quickly by any other method. 5. Fractures associated with nerve or vessel damage. 6. Infected fractures, for which internal fixation might not be suitable. 7. Un-united fractures, where dead or sclerotic fragments can be excised and the remaining ends brought together in the external fixator; sometimes this is combined with elongation in the normal part of the shaft 107

108
Complications of external fixation
High degree of training and skill! Often used for the most difficult fractures increased likelihood of complications Damage to soft-tissue structures Over-distraction No contact between the fragments union delayed/prevented Pin-track infection 108

109
OPEN FRACTURES Initial Management At the scene of the accident
In the hospital 109

110
Types of Open Fractures
Gustilo’s classification of open fractures: Type 1: low-energy fracture with a small, clean wound and little soft-tissue damage Type 2: moderate-energy fracture with a clean wound more than 1 cm long, but not much soft-tissue damage and no more than moderate comminution of the fracture. Type 3: high-energy fracture with extensive damage to skin, soft tissue and neurovascular structures, and contamination of the wound. 110

111
Types of Open Fractures
Type 3 A: the fractured bone can be adequately covered by soft tissue Type 3 B: can’t be adequately covered, and there is also periosteal stripping, and severe comminution of the fracture Type 3 C: if there is an arterial injury that needs to be repaired, regardless of the amount of other soft-tissue damage 111

112
Types of Open Fractures
The incidence of wound infection correlates directly with the extent of soft-tissue damage, <2% in type 1 >10% in type 3 rises with increasing delay in obtaining soft tissue coverage of the fracture. 112

113
Principles of Treatment of Open Fractures
All open fractures assumed to be contaminated Prevent infection! The essentials: Prompt wound debridement Antibiotic prophylaxis Stabilization of the fracture Early definitive wound cover Repeated examination of the limb because open fractures can also be associated with compartment syndrome 113

114
CONTRAINDICATIONS TO SURGICAL REDUCTION AND STABILIZATION
Situations in which there is a high probability for failure with operative treatment are as follows: 1. Osteoporotic bone that is too fragile to allow stabilization by internal or external fixation. 2. Soft tissues overlying the fracture or planned surgical approach of such poor quality because of scarring, burns,active infection, or dermatitis . 3. Active infection or osteomyelitis.

115
CONTRAINDICATIONS TO SURGICAL REDUCTION AND STABILIZATION
4. Fracture comminution to a degree that does not allow successful reconstruction. This is most commonly seen in severe intraarticular fractures. 5. General medical conditions that are contraindications to anesthesia are generally contraindications to the surgical treatment of fractures. 6. Undisplaced or stable impacted fractures in acceptable position do not require surgical exposure or reduction. 7. Inadequate equipment, manpower, training, and experience.

116
Thank you

Similar presentations












, F.R.C.S.(C )>")














